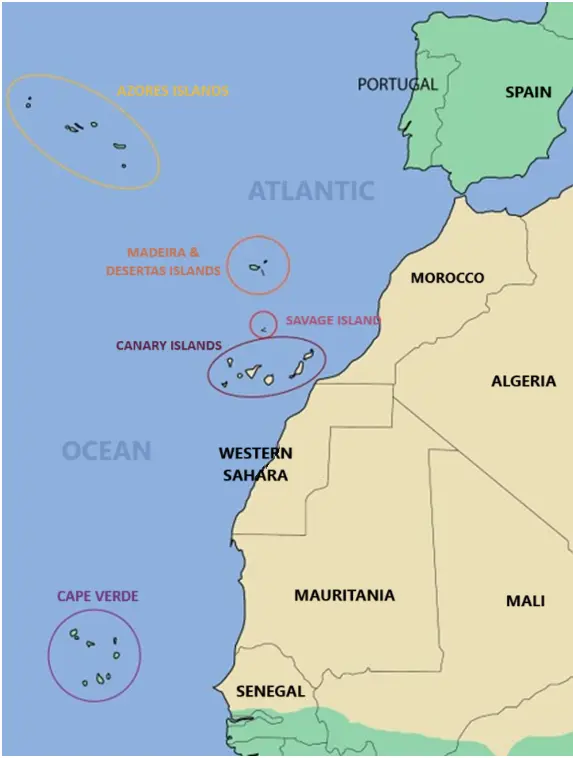
Genetic studies in the Atlantic Azores Islands (1500 km far from Portugal) show that the modern population is composed of both northern and southern European populations. However, a significant Chinese input of HLA characteristic genes is noticed, possibly with people or genes that may have been left by Zheng-He very big crew which sailed seas from China in a long-lasting expedition (1421–1423 AD). This was concluded after Azorean HLA genetics comparison with HLA genes of worldwide populations by both neighbour joining and correspondence methodology. Also, the Machado- Joseph ataxia disease gene variant (ATXN3, Chr 14) is identical in China and the Azores, where this ataxia was discovered, and it has a high frequency. Moreover, the predisposing HLA-B*2707 gene variant to ankylosing spondylitis is the same in Azores and Far East Asian countries. This data may reflect a strong founder Chinese effect followed by isolation in Azores. In addition, “Carthaginian” coins were found in Corvo Is (Azores) of Spanish fabrication. This is contradictory to the official version that pre- Portuguese Azores had been virgin and inhabited. Also, Cart–ruts in Azores indicate a (Atlantic) common culture with Canary Islands and Mediterranean area. On the other hand, genetic studies on Canarians show that they present European, Iberian and Berber characteristics. A prehistoric lunisolar megalithic calendar is found: “Quesera” (Cheeseboard) of Zonzamas, pyramids similar to those found in nearby Western Sahara (90 km far from Canary Islands). In addition, lbero-Guanche rock scripts which can be transcripted with Iberian-Tartessian signary and are also found at Tim Missaw shelter (Sahara Desert, Algeria). Populated green Sahara area dissecation after 5000 years BC and subsequent people migration could be the origin of Canary Islands, Sahara and other Mediterranean culture traits. Thus, we have defined the Saharo-Canarian Circle as a genetic, anthropological, and prehistoric culture radiation area; it might have given raise to the Iberian-Tartessian signary and to other ancient lineal Mediterranean scripts.
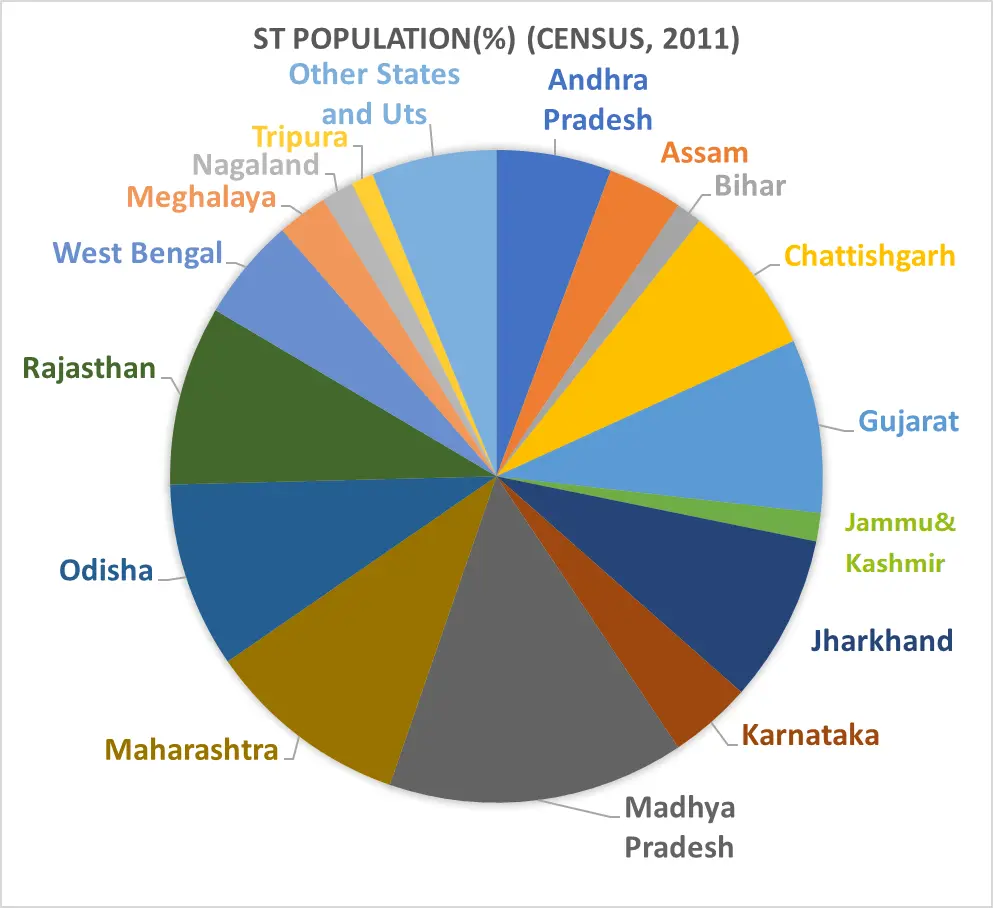
This review aimed to synthesize evidence from 2010–2024 on the nutritional status of adult tribal populations in India, with a focus on Chronic Energy Deficiency (CED) as assessed by Body Mass Index (BMI). Given the persistent health disparities among India’s Scheduled Tribes (STs), the study sought to examine geographic patterns, sex differentials, and contextual determinants of undernutrition across major tribal regions of the country. A systematic literature search was conducted using Google Scholar, PubMed, and JSTOR to identify peer-reviewed studies on adult tribal nutrition in India published between 2010 and 2024. National datasets—including the Census of India (2011) and the National Family Health Survey (NFHS-5, 2019–2021)—were used to provide demographic and health context. Eligible studies reported BMI-based nutritional assessments using the WHO (1995) BMI classification (CED defined as BMI < 18.5 kg/m2). Forty-four studies met the inclusion criteria. Extracted data were summarized by region, tribe, sex, and CED prevalence. The review reveals pronounced regional and sex-based disparities in CED among tribal adults. Northern and Northeastern tribal groups exhibited highly variable CED levels, ranging from very low in the Apatani (≤2%) to extremely high among Gujjar and Bakerwal women (90.7%). Eastern India showed consistently elevated CED, particularly among the Bhumij, Lodha, Kheria, and Santal tribes, with female CED often exceeding 50%. Central and Western tribes—including the Gonds, Kharwar, Mawasi, and Tadvi—displayed widespread undernutrition driven by food insecurity, poverty, and limited healthcare access. Southern India showed critical CED prevalence among Jenu Kuruba and Koraga adults (>90%), while island populations such as the Shompens exhibited low CED but high anaemia burdens. NFHS-5 corroborated these findings, indicating serious national-level CED prevalence among ST adults (18.4% in men, 25.5% in women). Across regions, coexisting burdens of anaemia, tuberculosis, hemoglobinopathies (e.g., sickle cell disease), leprosy, and vector-borne diseases further compounded poor nutritional status. Adult tribal populations in India experience disproportionately high levels of CED, shaped by intersecting structural and cultural determinants including poverty, geographic isolation, gender inequality, food insecurity, and limited access to health services. The wide regional variability underscores the need for targeted, culturally informed, region-specific nutritional interventions. Strengthening surveillance, improving healthcare accessibility, and promoting community-engaged, bottom-up health strategies are essential for reducing disparities and achieving national commitments to the Sustainable Development Goals, particularly the mandate to “Leave no one behind”.
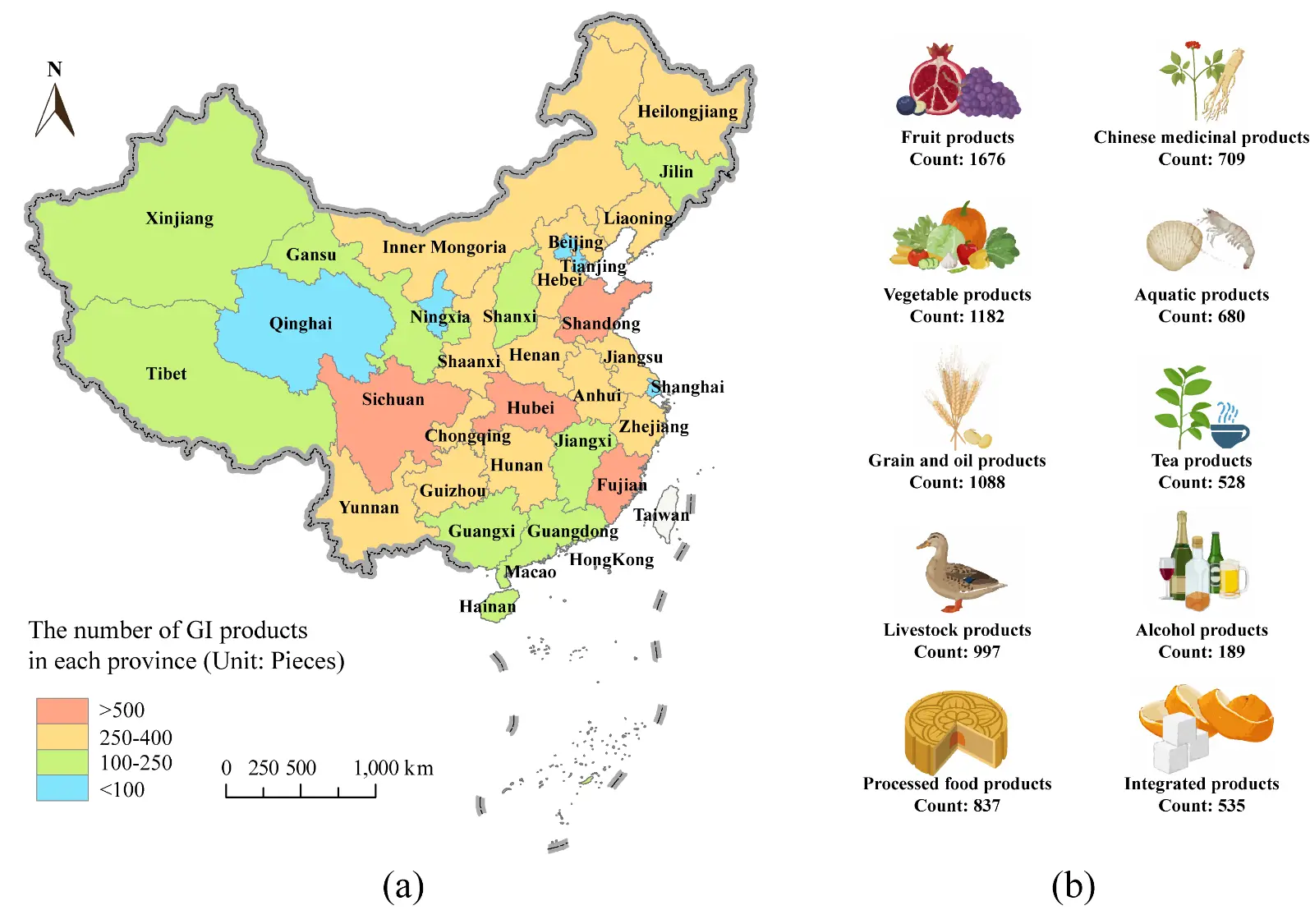
China, with its vast territory, harbors abundant regional food resources with multiple values in nutrition, ecology, and anthropology. However, simply adopting the World Trade Organization’s (WTO) Geographical Indication (GI) system for classifying and managing these agricultural products fails to fully reflect their authentic natural and anthropological attributes, which cannot support the development of local characteristic economies and food cultural ecosystems. Therefore, there is an urgent need to establish a hierarchical classification standard system for regional food resources tailored to China’s national conditions. This paper proposed a new definition for China’s endemic and characteristic food resources and summarizes interdisciplinary research methods for exploring their biological and cultural attributes. Additionally, the economic and sociological values of these resources were discussed. The proposed classification standards provide guidance for the industrialization of regional food resources in China and offer new ideas for transforming biodiversity into novel productive forces in characteristic industries.
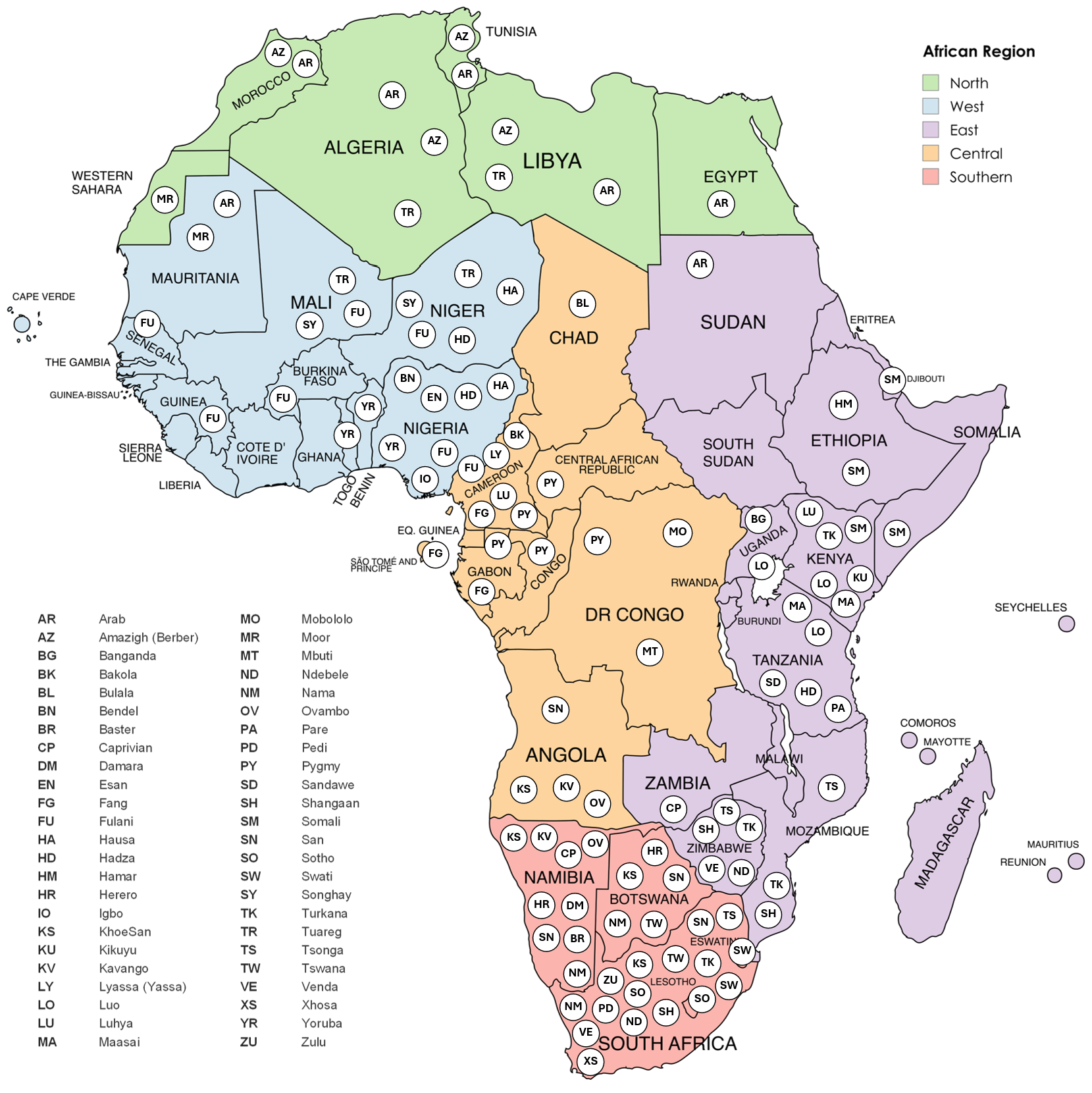
Africa harbors unparalleled genetic and cultural diversity. Yet, despite cancer being a major global non-communicable disease, African populations, particularly Indigenous groups, remain remarkably underrepresented in cancer genomics research. This review examines the current landscape of cancer genomics studies across Africa, with emphasis on population diversity and the extent to which Indigenous populations have been included. The genetic heterogeneity across African populations is discussed, and how it can influence cancer susceptibility, tumor biology, and therapeutic response, underscoring the fact that findings from non-African cohorts may not have the same significance in African cohorts. A substantial knowledge gap persists, and expanding studies in Africa could significantly provide valuable insights for global cancer biology. These factors emphasize the urgency of an African-based and African-owned biobanking infrastructure to support equitable research, strengthen local capacity and ethical stewardship of genomic resources towards the promotion of precision oncology and health equity on the continent.
This study examines how classical Islamic legal concepts are rearticulated within contemporary Indonesian halal-health governance. Focusing on the concepts of ʿurf (custom) and istiṣlāḥ (public interest), the research investigates how normative traditions are integrated into biomedical regulation and institutional decision-making. Using qualitative textual and discursive analysis, the study analyzes fatwa documents, regulatory guidelines, policy statements, and scholarly writings related to halal pharmaceuticals, vaccination, and health certification. The findings indicate that ʿurf is increasingly mediated through administrative and certification frameworks, while istiṣlāḥ is progressively proceduralized through technical evaluation and performance indicators. Religious authority is reconfigured through interdisciplinary expert networks that combine juristic reasoning with scientific and bureaucratic validation. At the discursive level, Islamic ethical vocabulary is systematically integrated with public health rationality, producing hybrid forms of moral-technical legitimacy. These transformations suggest that halal-health governance operates through negotiated continuity rather than epistemic rupture. Classical legal concepts are neither abandoned nor preserved unchanged; rather, they function as discursive interfaces between tradition and institutional governance. By highlighting the infrastructural conditions of ethical adaptation, this study contributes to a more nuanced understanding of Islamic normativity under contemporary biocultural and regulatory regimes.
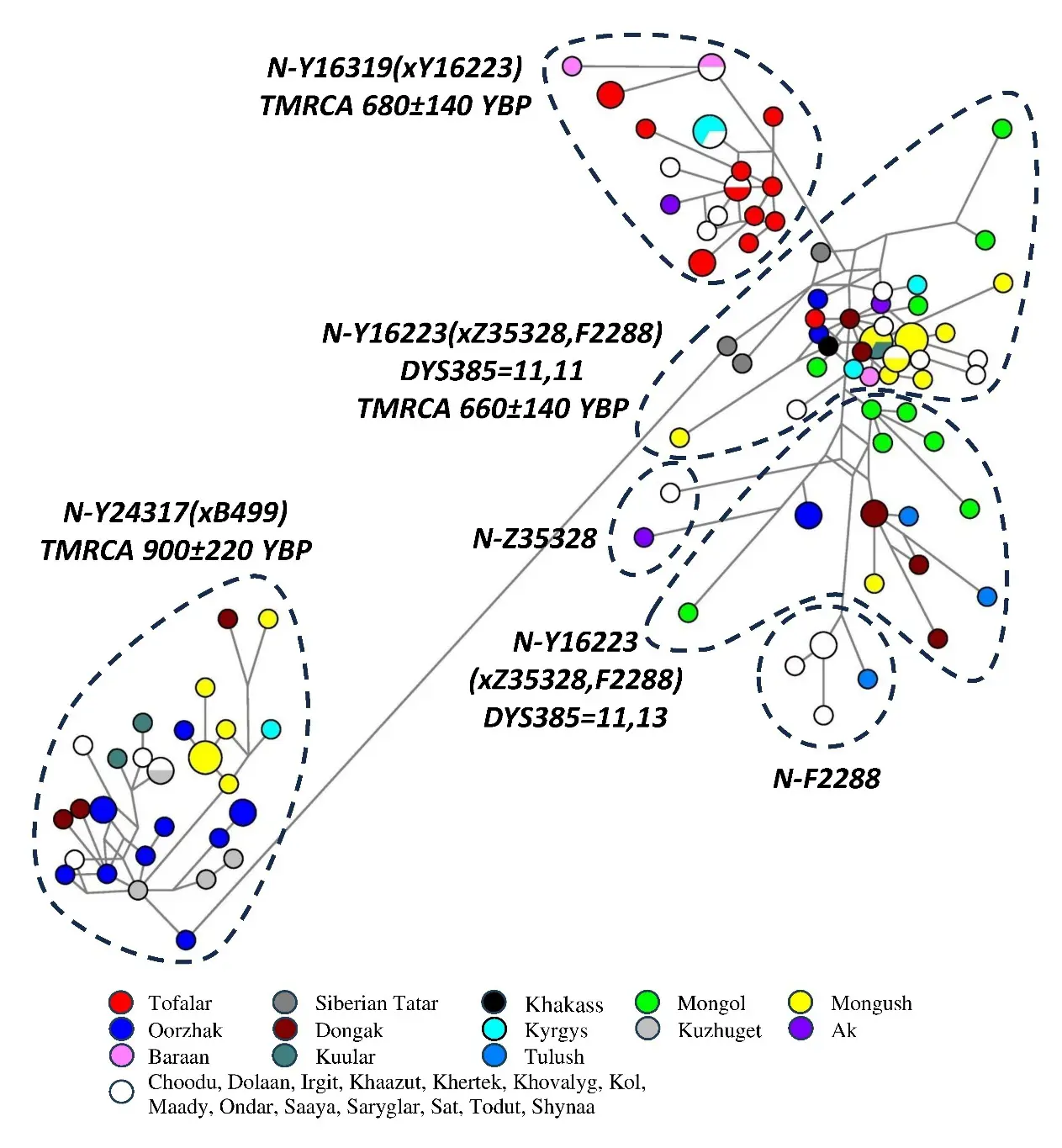
Some important aspects of the history of ethnogenesis in South Siberia have been reconstructed using data on two Y-haplogroups: N-M178 (n = 113) and O-M175 (n = 24). In Tuvans, who make up two-thirds of the indigenous South Siberian population, these haplogroups constitute 20% of the gene pool, and their branches form well discriminated ethno-specific clusters within the phylogenetic network of 37 Y-STR marker haplotypes. N-Y24317(xB499) is thought to have arrived in Tuva from Mongolia or Northwest China during the Bronze Age or Early Iron Age. According to our hypothesis, the spread of N-Y16319(xY16223) and N-Y16223(xZ35328, F2288) with DYS385 = 11,11 is linked to the development of the Ulug-Khem culture in Tuva around 2100 YBP as a result of the growth and expansion of the Xiongnu. Three branches (N-Z35328, N-F2288, N-Y16223(xZ35328, F2288) with DYS385 = 11,13) widespread among the Turkic-Mongolian populations are rare in Tuvans. The arrival of these haplogroups, as well as O-M175, in Tuva is associated with the Medieval Mongol expansion. However, the Turkic-Mongolian contribution of O-M175 to the Tuvan gene pool is insignificant: the ancestors of most Tuvan lineages might have been the Han forcibly moved by the Yuan Empire to the settlements of craftsmen and farmers located in what is now the territory of modern Tuva.
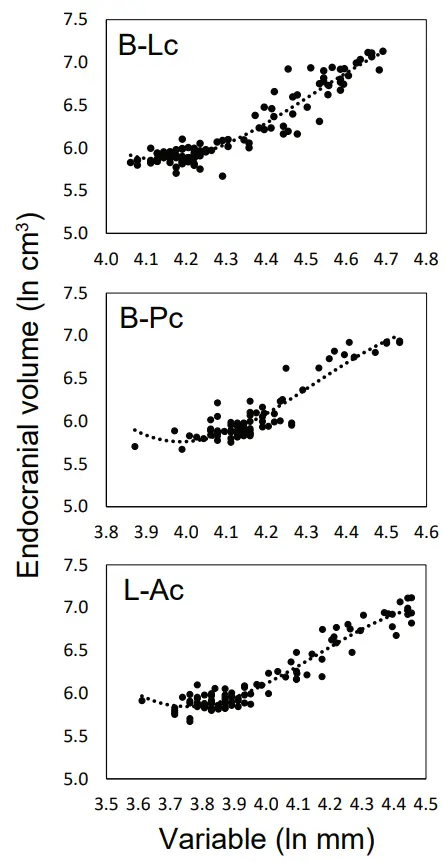
Sterkfontein specimen Sts 25 is filled with calcified sediment and still partly encased in matrix. The only published endocranial volume estimate for this specimen (350–375 cm3) falls outside the range of variation for Australopithecus africanus adults. The purpose of this study was to estimate Sts 25’s endocranial volume and to explore the usefulness of parietal regressions for estimating brain size in other fragmentary hominin specimens. We used single-variable and multivariate polynomial regressions and combined chimpanzee/early hominin comparative samples to predict endocranial volumes for Sts 25 and 10 fragmentary hominin specimens from six chord and arc variables. Point estimates for Sts 25 ranged between 412–501 cm3, with random-effects means and 95% prediction intervals of 453 cm3 (393–512 cm3) from single-variable regressions and 446 cm3 (377–514 cm3) from multivariate regressions. New endocranial volume estimates ~450 cm3 for Sts 25 are consistent with values for other A. africanus specimens with similar dimensions of the vault and basicranium. Volume estimates for Sts 58 (468–559 cm3) and MLD 1 (509–595 cm3) are larger than previous estimates for these specimens and help refine the A. africanus range. Endocranial volume estimates for other crania are largely consistent with existing predictions, establishing the value of these polynomial regression equations for estimating brain size in early hominins.