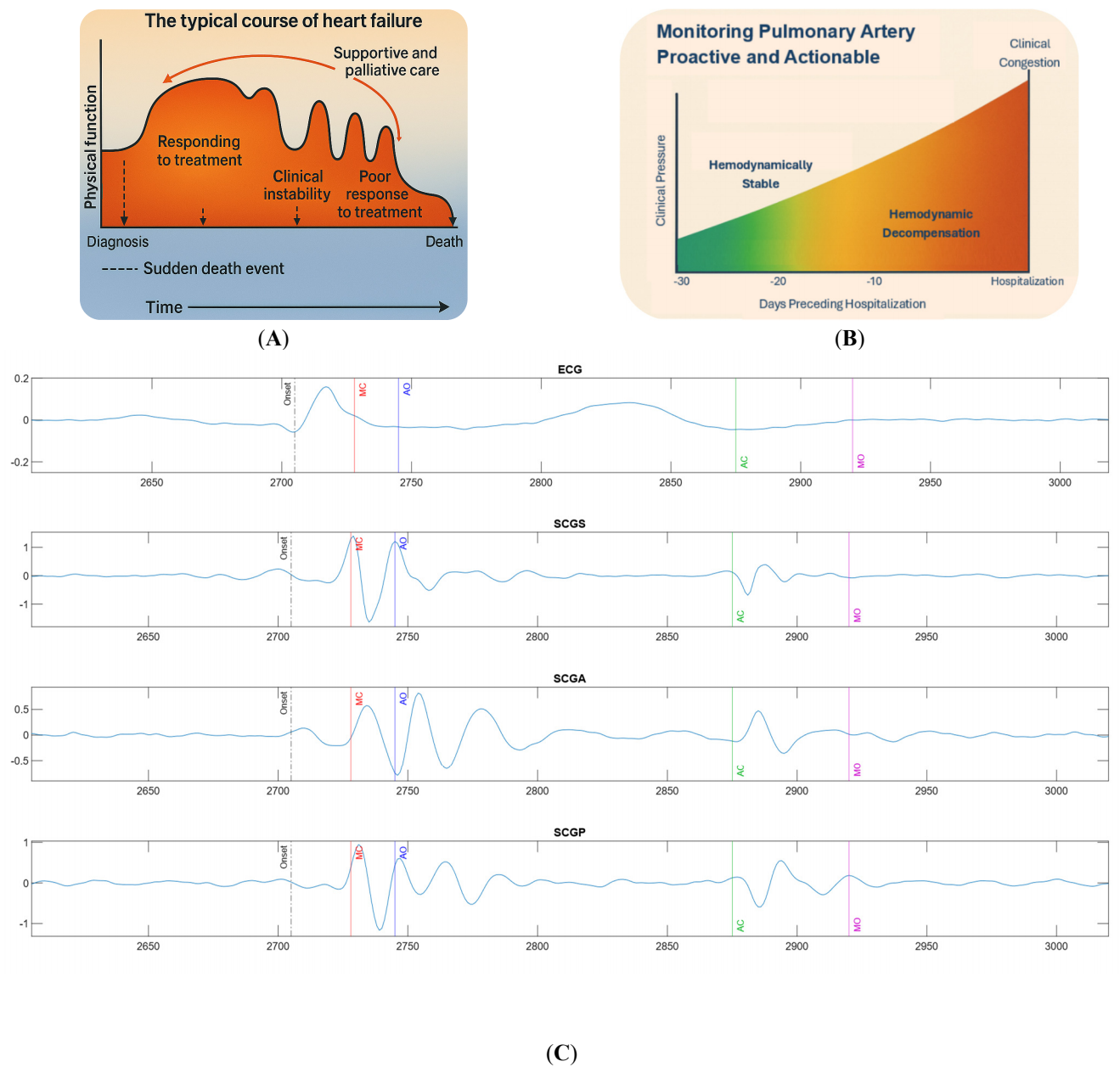
Congestive heart failure (CHF) encompasses both reduced and preserved ejection fraction phenotypes. Modern management increasingly demands actionable insights into cardiac function beyond standard vitals. Cardiac time intervals (CTIs), including mitral valve closure (MVC), aortic valve opening (AVO), aortic valve closure (AVC), and mitral valve opening (MVO), as well as isovolumetric contraction time (IVCT) and isovolumetric relaxation time (IVRT), offer a window into the electromechanical timing of systole and diastole. These intervals provide clinically relevant markers of systolic function, diastolic filling dynamics, and chamber compliance. In HFrEF (reduced ejection fraction), CTI monitoring captures deterioration in contractile efficiency; in HFpEF (preserved ejection fraction), diastolic stiffness and shortened filling times can be tracked. Remote CTI monitoring facilitates timely therapy adjustments, prevents hospitalizations, empowers patients in their disease management, and provides clinicians with early warning signals of worsening physiology. CTIs enable a comprehensive, non-invasive assessment of cardiac chamber performance. This is especially relevant across the full spectrum of heart failure, including both HFrEF and HFpEF. The ability to deliver precise cardiac timing data outside of traditional clinical settings makes it a transformative tool for proactive, physiology-based heart failure management.
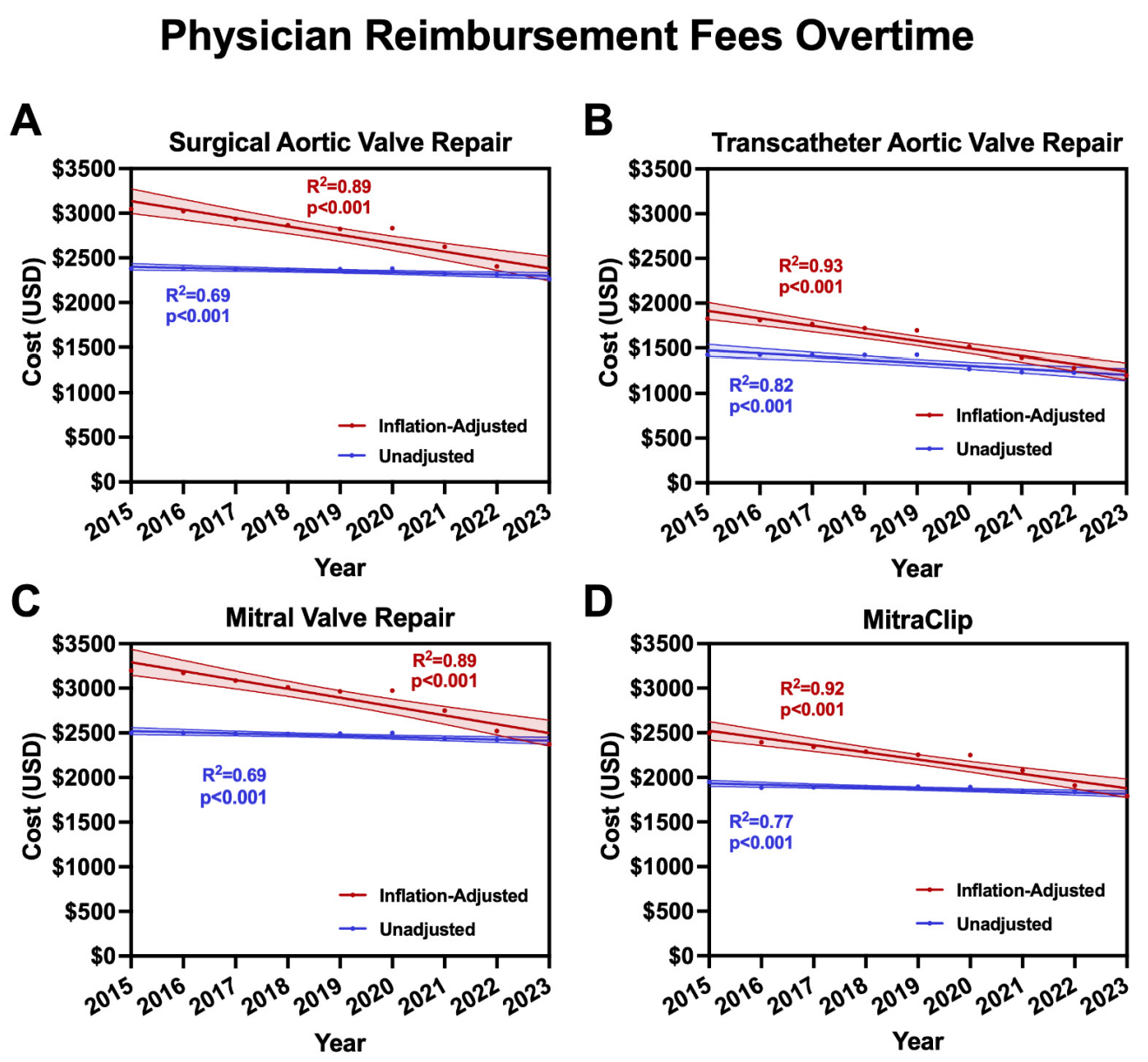
We aimed to quantify contemporary changes in physician Medicare reimbursement for surgical and transcatheter valvular procedures. Publicly available 2015–2023 data from the Centers for Medicare & Medicaid Services were used to identify annual physician reimbursement fees for four procedures: surgical aortic valve replacement (SAVR), transcatheter aortic valve replacement (TAVR), mitral valve repair (MVr), and MitraClip. Physician reimbursement fees were adjusted for inflation into 2023 U.S. dollars. Changes over time were analyzed using linear regression to account for differences in average annual U.S. dollar decline, average annual percent change, and total percent change over the study period. Reimbursement for surgical and transcatheter valve procedures declined by a combined total of 28.5%: 25.8% SAVR, 34.2% TAVR, 25.8% MVr, and 28.3% MitraClip. They corresponded to average annual percent changes of −3.7% (SAVR), −5.1% (TAVR), −3.7% (MVr), and −4.1% (MitraClip)—representing a collective decline in reimbursement fee per patient of $784.96 (SAVR), $624.73 (TAVR), $823.54 (MVr), and $706.12 (MitraClip) over the nine-year study span. Over the last decade, physician reimbursement for surgical and transcatheter valve procedures has significantly decreased, potentially threatening access to quality cardiac care within the heart team approach.
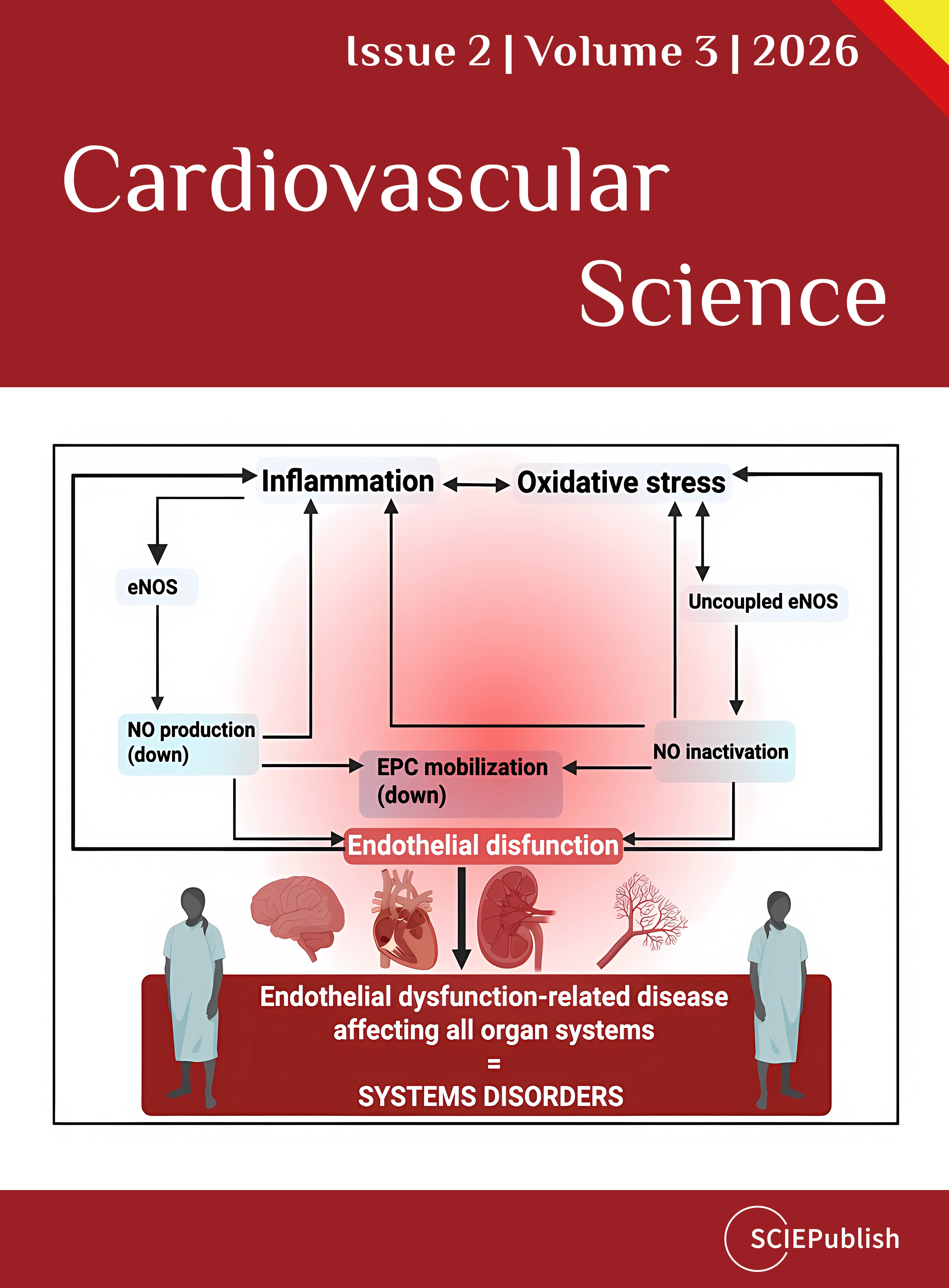
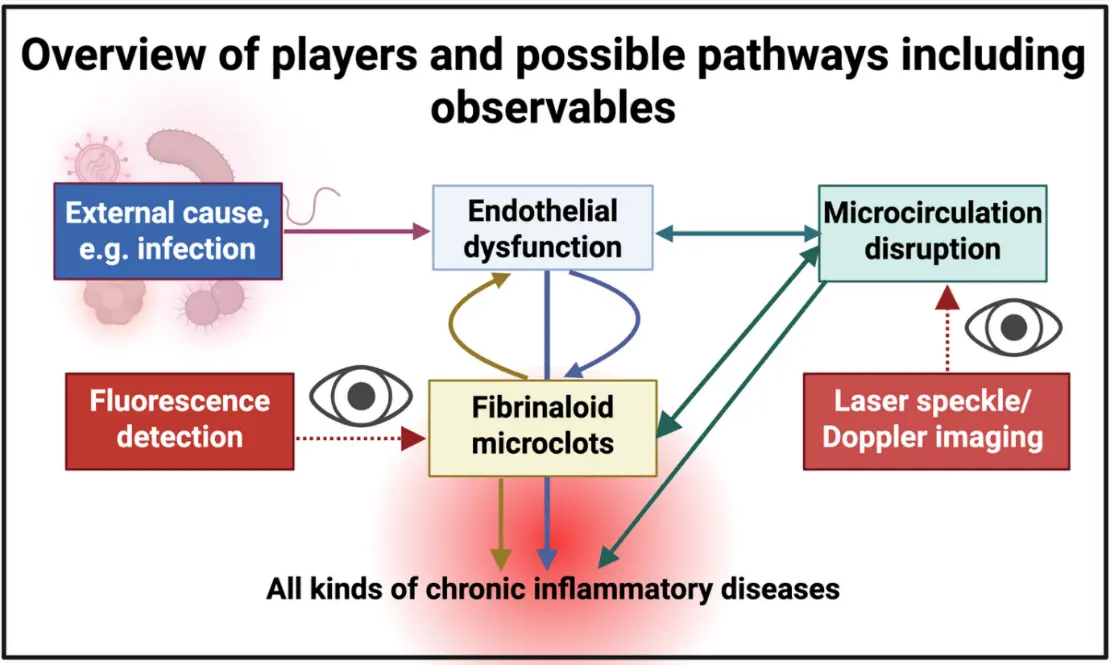
The microcirculation typically refers to those capillaries less than 100 μm in diameter. We have shown that blood can clot into an anomalous amyloid form, manifesting as microclots of typically 2–200 μm equivalent diameter that are rather resistant to fibrinolysis. Because they contain fibrin and other proteins in an amyloid form, we have referred to them as fibrinaloid microclot complexes. We have also previously developed the idea that endothelial dysfunction can both lead to and be caused by the fibrinaloid microclots so formed, such that this can slow or block entirely parts of the microcirculation. The microclots might be thought of as a ‘structural’ manifestation in that they are actual, observable structures. This impairment of the microcirculation is referred to in Traditional Chinese Medicine (TCM) as ‘blood stasis’. It is thus desirable to have ‘functional’ methods that can measure these effects on the microcirculation directly. As a complement to a recent survey of nailfold capillaroscopy, the present paper provides a wide-ranging review of the utility of laser speckle imaging (LSI) and laser Doppler imaging (LDI) for assessing the microcirculation in a large variety of diseases in which it is considered to be involved. These include Long COVID, sepsis, and ischaemic stroke. In all cases in which fibrinaloid microclots have been observed, so too do these methods detect an impairment of the microcirculation. Notably, blood pressure is raised while blood flow in the microcirculation is lower; this clearly speaks to occlusion and/or capillary rarefaction, and indicates that the raised blood pressure is the effect and not the cause of the decrease in flow rate or stasis of the microcirculation. As rapid, information-rich and non-invasive methods, LSI and LDI seem to have outstanding potential for assessing the role of fibrinaloid microclots in affecting blood stasis in the microcirculation, in a huge variety of inflammatory diseases and syndromes.
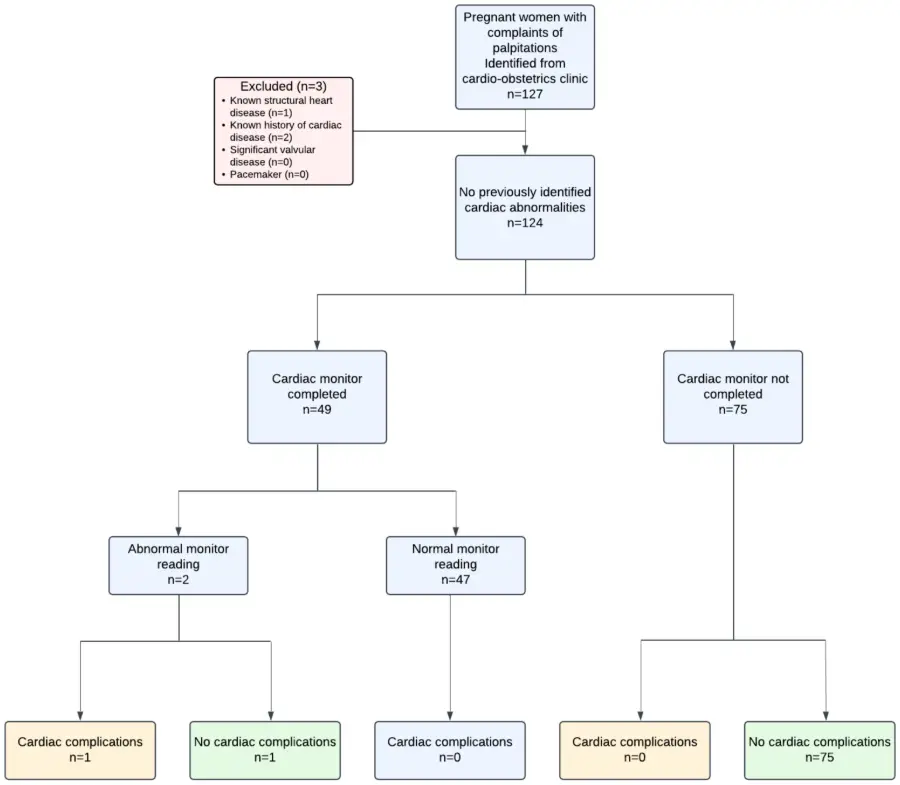
Ambulatory Cardiac Monitoring (ACM) is often used to evaluate pregnant patients with palpitations without structural heart disease; however, the diagnostic yield is not well defined. This single-center retrospective cohort study included pregnant patients without structural heart disease evaluated in a tertiary care cardio-obstetrics clinic between June 2023 and June 2024. The primary outcome was the detection of a clinically significant arrhythmia. Secondary outcomes included symptom–rhythm correlation and adverse maternal cardiac, obstetric, and fetal outcomes. Out of 124 patients identified, 49 (40%) completed ACM. Two patients had symptomatic clinically significant arrhythmias detected on ACM, including non-sustained ventricular tachycardia that did not alter management (n = 1), and symptomatic supraventricular tachycardia (SVT) resulting in medical therapy (n = 1). Palpitations occurred during monitoring in 35 of the 49 remaining monitored patients; of those, symptoms correlated with non-significant arrhythmias (premature atrial and ventricular contractions) in 11 (31%). No adverse cardiac events occurred in the remaining patients. Obstetric and fetal outcomes did not differ between monitored and unmonitored patients. In this small single center study, ACM in pregnant patients without structural heart disease has a low diagnostic yield. These findings could be used in shared decision-making for pregnant patients being evaluated for palpitations.
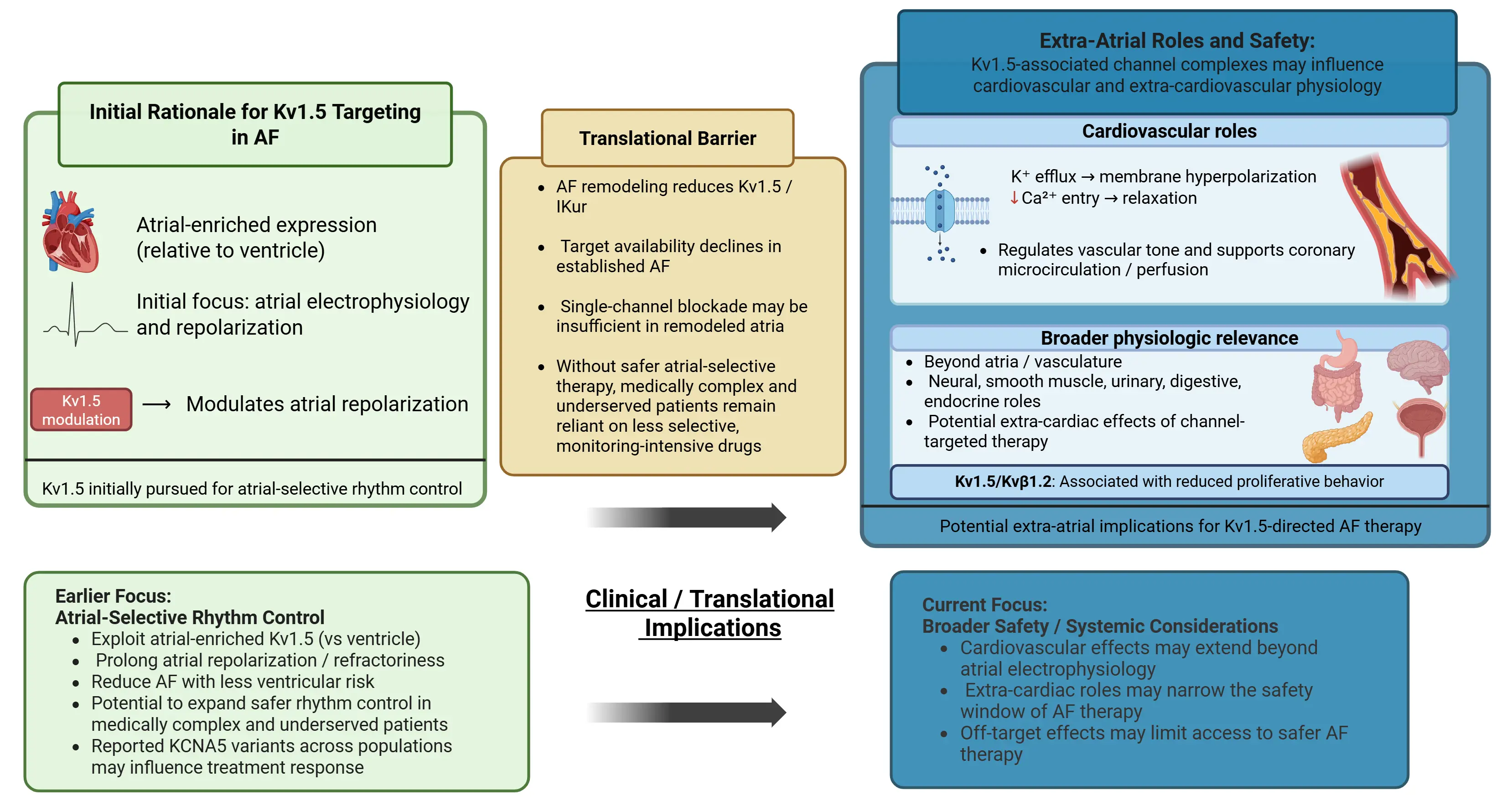
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and a growing source of cardiovascular morbidity, stroke, heart failure, and death. Current pharmacologic rhythm-control strategies rely predominantly on antiarrhythmic agents with significant ventricular proarrhythmia risk and systemic toxicity, limiting their use in medically complex and underserved patient populations. The Kv1.5 channel, encoded by KCNA5, generates the atrial-selective ultrarapid delayed rectifier current (IKur) and has long been considered a promising target for safer rhythm control. This review focuses on the molecular biology of Kv1.5, including its regulation by auxiliary Kvβ1.2 subunits, redox signaling, oxidative stress, and extra-atrial vascular roles, and examines the preclinical and clinical evidence for Kv1.5-targeted therapy. We analyzed why selective IKur inhibitors, including XEN-D0103 and MK-0448, have failed to translate into effective antiarrhythmic therapy, with particular attention to the role of atrial electrical remodeling and reduced IKur density in established AF. We also review the limitations of existing class III and class Ic antiarrhythmic agents and discuss how genetic variation in KCNA5 across ethnic populations may inform more precise and equitable approaches to rhythm control. Together, these findings highlight the promise of Kv1.5 as an atrial-selective target and the major barriers limiting its clinical translation in AF.