Issue 1, Volume 1 – 5 articles
Cover Story (View full-size image):
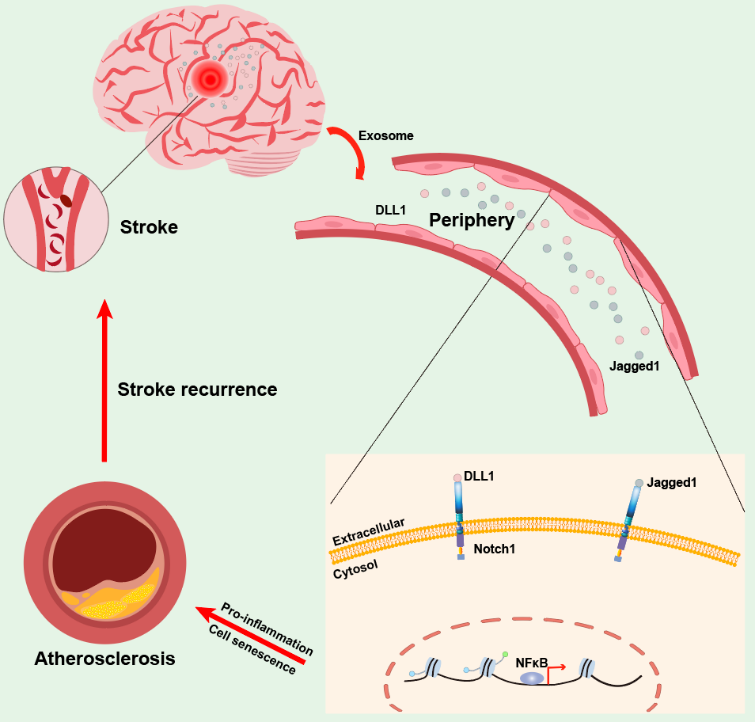
Stroke elicits persistent activation of peripheral endothelial cells, upregulation of proinflammatory molecules, and increased cellular senescence. This aberrant endothelial activity is caused by sustained Notch1 signaling, which is triggered by increased circulating Notch1 ligands DLL1 and Jagged1 after stroke. Thus, by generating senescent proinflammatory endothelial cells, leads to increased myeloid cell adhesion and atherosclerotic progression and also increases the risk of recurrent stroke. This study reveals a systemic mechanism driving sustained activation of peripheral ECs after stroke, offering novel insights for therapeutic intervention or prevention of recurrent vascular events after stroke.
View this paper