Utility of Ambulatory Non-Invasive Rhythm Monitoring in Pregnant Patients with Palpitations and Structurally Normal Hearts

Utility of Ambulatory Non-Invasive Rhythm Monitoring in Pregnant Patients with Palpitations and Structurally Normal Hearts
Diana Kline
1,†
Merrina Lan
1,†
 Matthew Granger
2
Lauren Hassen
2
William H. Marshall V
2,*
Matthew Granger
2
Lauren Hassen
2
William H. Marshall V
2,*
Received: 22 March 2026 Revised: 29 April 2026 Accepted: 15 May 2026 Published: 27 May 2026

© 2026 The authors. This is an open access article under the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
1. Introduction
Cardiovascular disease is the leading cause of death in pregnant and postpartum patients [1], which has brought increasing attention to maternal cardiovascular health. One common cardiac symptom that leads to cardiology referral during pregnancy is palpitations. While some arrhythmias may occur during normal pregnancy, symptoms raise concern for the well-being of the patient and fetus [2,3]. Supraventricular tachycardia (SVT) is the most common arrhythmia during pregnancy and may be associated with an increased risk of Cesarean delivery and preterm labor [4], and arrhythmias during pregnancy that lead to hospitalization are associated with maternal mortality and complications [5].
Ambulatory cardiac monitoring (ACM) can be used to evaluate symptomatic patients, and in pregnant patients with structural heart disease, it has high clinical utility in detecting arrhythmias [6,7]. However, many patients with palpitations during pregnancy do not have structural heart disease. To our knowledge, cardiac monitoring in the population has not been studied since 1997 [3]. Furthermore, little is known about the yield of cardiac monitoring in pregnant patients without heart disease and the factors that predict the likelihood of detecting abnormalities from monitoring. Because continuous cardiac monitoring can impose patient burdens and facility costs [8], clinicians may consider monitoring for patients who are more likely to benefit from it.
Given the lack of current data on the efficacy of ACM in pregnant patients without preexisting heart disease, this study aims to evaluate the frequency of clinically significant arrhythmias in pregnant patients without structural heart disease and determine how cardiac monitoring impacts clinical management.
2. Methods
2.1. Study Design
We performed a single-center, retrospective cohort study of pregnant patients with palpitations seen at the cardio-obstetrics clinic at The Ohio State University Wexner Medical Center from June 2023 to June 2024, with follow-up available through January 2025. The Ohio State University’s Biomedical Institutional Review Board (IRB) approved this study.
2.2. Patient Identification, Classification, and Data Collection
Patients were included if they were pregnant at the time of evaluation, had no structural heart disease according to chart documentation, and if a transthoracic echocardiogram (TTE, obtained at the treating provider’s discretion) revealed a structurally normal heart (defined as normal biventricular size and systolic function with no more than mild valvular disease, including mitral valve prolapse) at the initial evaluation. Thus, patients with more than mild valvular regurgitation or stenosis, congenital heart disease, or pacemakers were excluded.
Baseline characteristics were collected from the medical record and included: maternal age at initial visit, gravidity, parity, race, pre-pregnancy body mass index, pre-pregnancy comorbidities, New York Heart Association (NYHA) functional class during pregnancy, medical therapy during pregnancy, and mode of delivery (cesarean section, vaginal delivery). While a cardiac history was recorded at initial presentation, detailed symptom characterization was not uniformly available due to the retrospective study design and variable documentation. Laboratory data, electrocardiogram, and cardiac monitor findings during pregnancy closest to the initial cardio-obstetric visit were recorded.
TTE data were obtained from the report in the medical record. Left and right ventricular systolic function, ventricular size, and valvular disease were determined based on consensus guidelines [9,10]. TTE and ACM were obtained at the discretion of the treating physician.
During the study time period, our institution utilized Boston Scientific Cardiac Diagnostics, Inc. (Houston, TX, USA), a subsidiary of Boston Scientific Corporation (Marlborough, MA, USA), for ACM. Based on the indication and clinician discretion, ACM included holter monitors, mobile cardiac telemetry, or event monitors, all of which have preset arrhythmia-activated recording as well as patient activated events, with holter monitors and mobile cardiac telemetry also calculating the burden of arrhythmias. Monitoring ranged from 24 h to 30 days, based on the physician’s discretion and symptom frequency. All recordings were reviewed by the prescribing cardiologist. Data were recorded from the monitor results in the chart by the authors, D.K. and M.L.
2.3. Outcomes Studied
The primary outcome evaluated was diagnosis of a significant arrhythmia on ACM; consistent with prior reports [6], this included: SVT, atrial fibrillation, atrial flutter, atrial tachycardia, ventricular tachycardia (sustained or non-sustained), symptomatic bradycardia, and second-degree type 2 or third-degree atrioventricular block. Sustained arrhythmias were those that lasted >30 s and/or required treatment.
Secondary outcomes studied included the frequency of symptom correlation with any arrhythmia (including premature atrial complexes [PACs] and premature ventricular complexes [PVCs]) on ACM.
Finally, maternal cardiac, obstetric, and fetal outcomes (detailed below) were compared between the groups with and without ACM. Adverse maternal cardiac outcomes (during pregnancy or 6 months postpartum) included hospitalization for cardiac cause, heart failure (defined as a chart diagnosis of heart failure and/or report of dyspnea and volume overload treated with diuretics), stroke, and death. Obstetric outcomes (defined by the medical record) included gestational hypertension, pre-eclampsia, eclampsia, chorioamnionitis, and postpartum hemorrhage [11]. Fetal outcomes included birth weight, miscarriage (spontaneous pregnancy loss before 20 weeks of gestation) [12], preterm birth (delivery occurring before 37 weeks of gestation) [13], fetal demise (intrauterine fetal death at or beyond 20 weeks of gestation) [14], and neonatal mortality (death of a liveborn infant occurring within the first 28 days of birth) [15].
2.4. Statistical Analysis
Categorical data are presented as frequencies and percentages, and compared using chi-square tests. Continuous variables are reported as median (interquartile range [IQR]). The Shapiro-Wilk test of normality was performed, and the Mann-Whitney U tests were used to compare the two groups for non-normally distributed variables. A two-tailed t-test of unequal variance was used for normally distributed variables. p-values < 0.05 were considered statistically significant. Analyses performed with IBM SPSS statistics version 29.0.2.0 (20).
3. Results
3.1. Baseline Characteristics
We identified 127 pregnant people with palpitations, 124 of whom met the inclusion criteria (Figure 1). The median age at initial visit was 30 (25–33) years, and the majority (73 (59%)) of patients identified as non-Hispanic white. Chronic hypertension was present in 15 (12%), hyperlipidemia in 6 (5%), and 61 (49%) previously had a cardiac evaluation, most commonly for palpitations, postural orthostatic tachycardia syndrome (POTS), and syncope (Table 1).
Of the 124 patients, 49 (40%) completed ACM, ranging from one to 30 days, for a total of 493 total days of monitoring. There were 75 (60%) patients who did not complete cardiac monitoring, either because the physician did not feel cardiac monitoring was necessary (n = 64), the patient had previously had unremarkable monitoring (n = 7), or the monitor was ordered but not completed by the patient (n = 4) (Table 1).
No significant differences in baseline characteristics were found between the monitored and unmonitored groups (Table 1). Echocardiography results were available for most patients (113 (91%) overall, 45 (92%) of monitored group, 66 (88%) un-monitored group) with a median left ventricular ejection fraction of 65 (60–65)% (Table 2).
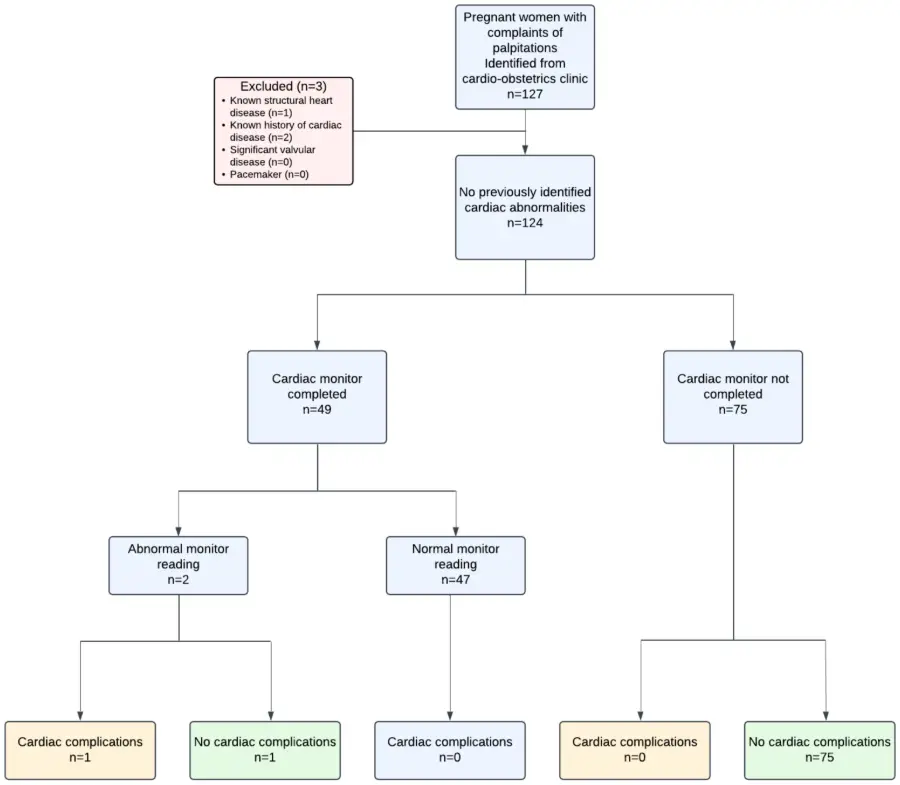
Table 1. Baseline characteristics, Maternal fetal outcome.
|
All Patients (n = 124) a |
ACM Group (n = 49) b |
No ACM Group (n = 75) c |
p-Value (Group 1 vs. Group 2) |
|
|---|---|---|---|---|
|
Age (years) |
30 (25, 33) |
30 (25, 34) |
30 (25, 33) |
0.87 |
|
GA at cardiology visit (weeks) |
25 (18, 33) |
25 (17, 30) |
25 (19, 34) |
0.44 |
|
Maternal race |
||||
|
Non-Hispanic black |
24 (19) |
11 (22) |
13 (17) |
0.48 |
|
Non-Hispanic white |
73 (59) |
27 (55) |
46 (61) |
1 |
|
Hispanic |
10 (8) |
5 (10) |
5 (7) |
1 |
|
Other |
17 (14) |
7 (14) |
10 (13) |
1 |
|
Gravida |
2 (1, 3) |
1 (1, 3) |
2 (1, 3) |
0.79 |
|
Para |
1 (0, 2) |
1 (0, 2) |
0 (0, 1) |
0.2 |
|
Body mass index (kg/m2) |
26 (23, 34) |
29 (24, 34) |
26 (23, 33) |
0.12 |
|
Chronic hypertension |
15 (12) |
8 (16) |
7 (9) |
1 |
|
Hyperlipidemia |
6 (5) |
3 (6) |
3 (4) |
1 |
|
Type 1 DM |
1 (1) |
0 (0) |
1 (1) |
1 |
|
Type 2 DM |
5 (4) |
2 (4) |
3 (4) |
1 |
|
Anxiety |
50 (40) |
23 (47) |
27 (36) |
1 |
|
Depression |
43 (35) |
14 (29) |
29 (39) |
1 |
|
Hyperthyroidism |
2 (2) |
2 (4) |
0 (0) |
1 |
|
Hypothyroidism |
10 (8) |
1 (2) |
9 (12) |
1 |
|
Prior cardiac evaluation or diagnosis |
61 (49) |
21 (43) |
40 (53) |
1 |
|
Reason for prior cardiac evaluation, n (%) |
||||
|
SVT |
7 (6) |
3 (6) |
4 (5) |
1 |
|
Murmur |
3 (2) |
1 (2) |
2 (3) |
1 |
|
POTS/syncope |
21 (17) |
4 (8) |
17 (22) |
1 |
|
Palpitations |
13 (10) |
6 (12) |
7 (9) |
1 |
|
Arrhythmia/irregular rhythm |
6 (5) |
5 (10) |
1 (1) |
1 |
|
Tachycardia |
11 (9) |
4 (8) |
7 (9) |
1 |
|
PAC/PVC |
6 (5) |
3 (6) |
3 (4) |
1 |
|
Cardiac Outcomes, n (%) |
||||
|
Hospitalization for cardiac cause during pregnancy or 6 months postpartum |
1 (1) |
1 (2) |
0 (0) |
1 |
|
Heart failure during pregnancy or within 6 months postpartum |
1 (1) |
1 (2) |
0 (0) |
1 |
|
Stroke |
0 (0) |
0 (0) |
0 (0) |
1 |
|
Death |
0 (0) |
0 (0) |
0 (0) |
1 |
|
Obstetric Outcomes, n (%) |
||||
|
Delivery mode |
||||
|
Vaginal |
79 (64) |
33 (67) |
46 (61) |
1 |
|
Cesarean Section |
41 (33) |
13 (27) |
28 (37) |
1 |
|
Gestational hypertension |
24 (19) |
9 (19) |
15 (20) |
1 |
|
Pre-eclampsia |
16 (13) |
8 (16) |
8 (11) |
1 |
|
Postpartum hemorrhage |
8 (6) |
1 (2) |
7 (9) |
1 |
|
Chorioamnionitis |
3 (2) |
2 (4) |
1 (1) |
1 |
|
Fetal Outcomes, n (%) |
||||
|
Miscarriage |
2 (2) |
1 (2) |
1 (1) |
1 |
|
Stillbirth |
0 (0) |
0 (0) |
0 (0) |
1 |
|
Preterm delivery |
14 (11) |
5 (10) |
9 (12) |
1 |
|
Gestational age (weeks) |
39 (38, 39) |
39 (38, 39) |
39 (38, 40) |
0.15 |
|
Twin gestation |
2 (2) |
0 (0) |
2 (3) |
1 |
|
Low birth weight |
12 (10) |
3 (6) |
9 (12) |
1 |
|
Neonatal mortality |
0 (0) |
0 (0) |
0 (0) |
1 |
Continuous variables are presented as median (Interquartile range). Categorical variables are presented as n (% of cohort). SVT: Supraventricular Tachycardia; POTS: Postural Orthostatic Tachycardia Syndrome; PAC: Premature Atrial Contraction; PVC: Premature Ventricular Contraction; a Unknown baseline characteristics in all patients: gestational age, n = 1; race, n = 1; BMI, n = 15. Unknown maternal fetal outcome in all patients: n = 3. b Unknown baseline characteristics in all patients with monitor: BMI, n = 7. Unknown maternal fetal outcome in all patients with monitor: n = 2; induced abortion due to trisomy 18: n = 1. c Unknown baseline characteristics in all patients without monitor: gestational age, n = 1; race, n = 1; BMI, n = 8. Unknown maternal fetal outcome in all patients without monitor: n = 1.
Table 2. Echocardiographic data.
|
All Patients (n = 124) a |
ACM Group (n = 49) b |
No ACM Group (n = 75) c |
p-Value (Group 1 vs. Group 2) |
|
|---|---|---|---|---|
|
Echocardiographic data |
||||
|
Gestational age at echo |
24 (18, 29) |
24 (18, 28) |
24 (18, 30) |
0.99 |
|
LV size |
||||
|
LV normal |
111 (98) |
45 (96) |
66 (100) |
1.00 |
|
LV enlarged |
2 (2) |
2 (4) |
0 (0) |
|
|
LVEF (%) |
65 (60, 65) |
60 (60,65) |
65 (60,65) |
0.71 |
|
RV size |
||||
|
RV enlarged |
8 (7) |
3 (6) |
5 (8) |
1 |
|
RV normal |
105 (93) |
44 (92) |
61 (92) |
|
|
LA size |
||||
|
LA normal |
104 (92) |
43 (91) |
61 (92) |
1 |
|
LA enlarged |
9 (8) |
4 (8) |
5 (8) |
|
|
RA size |
||||
|
RA normal |
110 (97) |
45 (96) |
65 (98) |
1 |
|
RA enlarged |
3 (3) |
2 (4) |
1 (2) |
|
|
TR velocity (m/s) |
2.1 (2, 2.3) |
2.1 (1.9, 2.3) |
2.1 (2.01, 2.3) |
0.53 |
|
RVSP (mmHg) |
20 (19, 24) |
21 (19, 24.8) |
20 (19, 24) |
0.66 |
LV: left ventricle; LVEF: left ventricle ejection fraction; RV: right ventricle; RA: right atrium; TR: tricuspid regurgitation; RVSP: Right Ventricular Systolic Pressure.a Unknown echocardiogram data in all patients: n = 11. b Unknown echocardiogram data in all patients with ACM: n = 2. c Unknown echocardiogram data in all patients without ACM: n = 9.
3.2. Diagnosis of Arrhythmia
Only 2 out of 49 (4%) patients who completed ACM yielded clinically significant arrhythmias. The first patient presented at 17 weeks of gestation with a self-reported history of recurrent SVT, with comorbidities of chronic hypertension, type 2 diabetes, and anxiety disorder. Echocardiogram revealed normal biventricular size and systolic function with no significant valve disease, and 14-day ACM revealed <1% burden PAC, <1% burden PVC, and a single episode of non-sustained ventricular tachycardia (NSVT), lasting 7 beats, at 220 beats per minute. Arrhythmias correlated with symptoms only 29% of the time and did not lead to changes in clinical management. The patient had a preterm delivery at 36 weeks and 5 days due to pre-eclampsia, and the patient did not have any cardiac complications.
The second patient presented to the clinic at 30 weeks’ gestation with complaints of dizziness and palpitations that began during pregnancy. Electrocardiogram from a prior hospitalization showed frequent PACs and SVT with right bundle branch aberration. The most recent echocardiogram prior to the visit showed normal biventricular size and systolic function and no significant valve disease, and 7 day ACM showed frequent PACs with a 27% burden, a 2% PVC burden, and frequent paroxysmal SVT. She was subsequently started on metoprolol, which controlled her symptoms. After a Cesarean delivery at 34 weeks in the setting of preterm premature rupture of membranes, she was seen 5 days postpartum in the hospital with sustained SVT resulting in clinical heart failure in the setting of missed metoprolol doses. She was treated with adenosine, and metoprolol was restarted with verapamil added to control the SVT. Heart failure symptoms improved with diuretic therapy, and arrhythmias remained well controlled thereafter.
3.3. Correlation of Arrhythmia with Symptoms
Symptoms of palpitations were reported in 35 of the 49 (71%) patients who completed ACM, of which 8 of 35 (23%) correlated with arrhythmias, including PVCs (n = 7), PACs (n = 2), NSVT (n = 1) (one patient had PAC, PVC, and NSVT). Additionally, 7 of 35 (20%) of patient-reported symptoms correlated with sinus tachycardia.
3.4. Cardiac, Obstetric, and Fetal Outcomes
Of the 47 (96%) patients with normal cardiac monitor readings and the 75 without ACM, none developed documented cardiac complications. There were no instances of stroke or maternal death during pregnancy or 6 months postpartum. Delivery mode and obstetric outcomes are reported in Table 1, with no significant differences between those with ACM and those without. Complete data on fetal outcomes were available in 94% of the monitored patients and 92% of the unmonitored patients, with no significant differences between the groups (Table 1).
4. Discussion
In this contemporary cohort of pregnant patients with structurally normal hearts evaluated for palpitations, we demonstrate that (1) non-invasive ambulatory cardiac monitoring without structural heart disease or prior significant arrhythmia has a low diagnostic yield and (2) only ~30% of patients with symptoms and any arrhythmia correlate on ACM, and most were not clinically significant. However, in patients with a significant history of arrhythmias, ACM may inform treatment.
The prior study evaluating ACM during pregnancy showed an increased incidence of arrhythmia in 110 pregnant patients compared to controls, but identified mostly PVCs and PACs. There was a low association between symptoms and arrhythmias, with only 10% of symptomatic episodes accompanied by an arrhythmia [3]. In our cohort, 29% did not have symptoms while wearing the ACM, and of the patients with symptoms, 23% had some arrhythmia with symptoms, though, as noted, only 2 were significant, and only 1 prompted medical therapy. Furthermore, 1/4 had only sinus tachycardia when reporting symptoms; this may be the result of physiologic hemodynamic changes associated with pregnancy [16].
Consensus guidelines recommend that the initial evaluation of a pregnant patient with palpitations should include a detailed cardiac history and characterization of symptoms, which can indicate who may benefit from further testing [17]. Data from our study support this targeted approach for patient selection for ACM. Based on our patient experience, ACM should be pursued in symptomatic patients with a prior arrhythmia; however, in patients without prior history, it may be possible to defer ACM. Prior studies of patients who experience SVT during pregnancy support this approach, as the majority have a known pre-pregnancy SVT history [4,18]. Clinicians may counsel patients about the low correlation between reported symptoms and clinically significant arrhythmias and reassure them that the vast majority of ACM results have low clinical impact. After a shared decision-making conversation, especially in the presence of financial constraints, inconvenience, or adhesive allergies, our data suggests that monitoring could be safely deferred in most patients. However, this does not render the test without value; many patients may still find reassurance from the absence of documented arrhythmias or from the correlation of symptoms with benign ectopy.
5. Limitations
Though not recommended for all patients to evaluate palpitations unless there is concern for underlying structural heart disease, in this real-world cohort, echocardiography was performed in the majority of patients. Though this limits the generalizability of ACM results, it is also a strength of the study, as it assures this cohort did not have significant underlying structural abnormalities. There are several other limitations of this study, including the non-randomized study design. Given this, ACM and TTE data were obtained at the discretion of the treating provider, and we did not have a non-pregnant control group to use for comparison. Data were collected retrospectively from medical records and were subject to inter-reader variability, and some patients had missing data due to unavailable records from outside hospitals. Detailed palpitation history prior to the initial clinic visit was not consistently documented, which limited how symptom history may have influenced ACM utilization and the subsequent diagnostic yield. Due to the retrospective nature of the study, with a limited sample size (only 49 patients completed ACM), the statistical power to detect differences in clinical outcomes is limited. Additionally, since this is a single cardio-obstetrics center with referrals from other hospitals, the patient demographics may not be generalizable to all institutions.
6. Conclusions
In this cohort of pregnant patients without structural heart disease, ACM demonstrated a low diagnostic yield for clinically significant arrhythmias. Furthermore, while 23% of patients reported symptoms with correlated rhythm abnormality, only 2 were clinically significant, and ACM likely has higher utility for patients with prior arrhythmia history. Though they require validation in larger randomized studies, these outcomes support a selective approach to ACM in low-risk patients that is guided by symptom history. These findings suggest that ACM for pregnant patients without preexisting arrhythmia or structural heart disease presenting for palpitations may safely be deferred.
Author Contributions
The authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and for the interpretation discussed. Concept/design: D.K., M.L., W.H.M.V. and L.H.; Data collection: M.G., D.K. and M.L.; Drafting and writing of article: D.K., M.L. and W.H.M.V.; Data analysis/interpretation: D.K., M.L. and W.H.M.V.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of The Ohio State University (study ID 2023H0313; Approval 12/19/23).
Informed Consent Statement
The Ohio State University Biomedical Institutional Review Board approved this study with waivered consent (study ID 2023H0313; Approval 12/19/23).
Data Availability Statement
The retrospective data used to support the findings of this study are restricted by the institutional review board in order to protect patient privacy. Data are available from the corresponding author for researchers who meet the criteria for access to confidential data.
Funding
This research received no external funding.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
American College of Obstetricians and Gynecologists’ Presidential Task Force on Pregnancy and Heart Disease and Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 212: Pregnancy and Heart Disease. Obstet. Gynecol. 2019, 133, e320–e356. DOI:10.1097/AOG.0000000000003243 [Google Scholar]
-
Adamson DL, Nelson-Piercy C. Managing palpitations and arrhythmias during pregnancy. Postgrad. Med. J. 2008, 84, 66–72. DOI:10.1136/hrt.2006.098822 [Google Scholar]
-
Shotan A, Ostrzega E, Mehra A, Johnson JV, Elkayam U. Incidence of arrhythmias in normal pregnancy and relation to palpitations, dizziness, and syncope. Am. J. Cardiol. 1997, 79, 1061–1064. DOI:10.1016/s0002-9149(97)00047-7 [Google Scholar]
-
Bekiaridou A, Coleman KM, Sharma N, George D, Liu Y, Gianos E, et al. Clinical Significance of Supraventricular Tachycardia During Pregnancy in Healthy Women. JACC Clin. Electrophysiol. 2024, 10, 1304–1312. DOI:10.1016/j.jacep.2024.03.014 [Google Scholar]
-
Vaidya VR, Arora S, Patel N, Badheka AO, Patel N, Agnihotri K, et al. Burden of Arrhythmia in Pregnancy. Circulation 2017, 135, 619–621. DOI:10.1161/CIRCULATIONAHA.116.026681 [Google Scholar]
-
Roldan P, McGrath L, Patel K, Brookfield K, Pare E, Khan A. Utility of continuous electrocardiographic monitoring in pregnant women with cardiovascular disease. Int. J. Cardiol. Congenit. Heart Dis. 2022, 7, 100305. DOI:10.1016/j.ijcchd.2021.100305 [Google Scholar]
-
Rodriguez CP, Economy KE, Duarte VE, Mehta N, Duncan ME, Chandler S, et al. Mobile Cardiac Telemetry Use to Predict Adverse Pregnancy Outcomes in Patients with Congenital Heart Disease. JACC Adv. 2023, 2, 100593. DOI:10.1016/j.jacadv.2023.100593 [Google Scholar]
-
Benjamin EM, Klugman RA, Luckmann R, Fairchild DG, Abookire SA. Impact of cardiac telemetry on patient safety and cost. Am. J. Manag. Care 2013, 19, e225-32. Available online: https://europepmc.org/article/med/23844751 (accessed on 15 July 2024).
-
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. DOI:10.1016/j.echo.2014.10.003 [Google Scholar]
-
Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography: Endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713; quiz 786–788. DOI:10.1016/j.echo.2010.05.010 [Google Scholar]
-
Committee on Practice Bulletins-Obstetrics. Practice Bulletin No. 183: Postpartum Hemorrhage. Obstet. Gynecol. 2017, 130, e168–e186. DOI:10.1097/AOG.0000000000002351 [Google Scholar]
-
Billing for Interruption of Pregnancy: Early Pregnancy Loss. Available online: https://www.acog.org/practice-management/coding/coding-library/billing-for-interruption-of-early-pregnancy-loss (accessed on 25 January 2026).
-
Preterm Labor and Birth. Available online: https://www.acog.org/womens-health/faqs/preterm-labor-and-birth (accessed on 25 January 2026).
-
Management of Stillbirth. Available online: https://www.acog.org/clinical/clinical-guidance/obstetric-care-consensus/articles/2020/03/management-of-stillbirth (accessed on 25 January 2026).
-
Pathirana J, Muñoz FM, Abbing-Karahagopian V, Bhat N, Harris T, Kapoor A, et al. Neonatal death: Case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2016, 34, 6027–6037. DOI:10.1016/j.vaccine.2016.03.040 [Google Scholar]
-
Sanghavi M, Rutherford JD. Cardiovascular Physiology of Pregnancy. Circulation 2014, 130, 1003–1008. DOI:10.1161/CIRCULATIONAHA.114.009029 [Google Scholar]
-
Joglar JA, Kapa S, Saarel EV, Dubin AM, Gorenek B, Hameed AB, et al. 2023 HRS expert consensus statement on the management of arrhythmias during pregnancy. Heart Rhythm 2023, 20, e175–e264. DOI:10.1016/j.hrthm.2023.05.017 [Google Scholar]
-
Shih-Huang L, Shih-Ann C, Tsu-Juey W, Chern-En C, Chen-Chuen C, Ching-Tai T, et al. Effects of pregnancy on first onset and symptoms of paroxysmal supraventricular tachycardia. Am. J. Cardiol. 1995, 76, 675–678. DOI:10.1016/S0002-9149(99)80195-7 [Google Scholar]