A Contemporary Analysis of Changing Payments for Surgical and Transcatheter Valve Procedures

A Contemporary Analysis of Changing Payments for Surgical and Transcatheter Valve Procedures
John A. Treffalls
1
 Sameer A. Hirji
2
Cheryl K. Zogg
3
Dina Al-Rameni
4
Tsuyoshi Kaneko
5
Kim de la Cruz
6,*
Sameer A. Hirji
2
Cheryl K. Zogg
3
Dina Al-Rameni
4
Tsuyoshi Kaneko
5
Kim de la Cruz
6,*
Received: 21 January 2026 Revised: 05 March 2026 Accepted: 23 April 2026 Published: 07 May 2026

© 2026 The authors. This is an open access article under the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
1. Introduction
In the United States, physician reimbursement rates are regulated at the federal level by the Centers for Medicare and Medicaid Services (CMS). All medical procedures are assigned a distinct Current Procedural Terminology (CPT) code linked to a relative value unit (RVU) related to the resources needed to perform the procedure. This RVU is ultimately multiplied by a conversion factor to determine a reimbursement rate in U.S. dollars for the current year.
In recent years, physicians have witnessed widespread declines in Medicare reimbursements [1,2]. These declines have occurred in the setting of inflationary pressure, rising healthcare costs, and an expanding Medicare beneficiary population [3,4]. Cardiothoracic surgeons have been disproportionately affected, facing inflation-adjusted reimbursement declines of more than 34%, more than neurosurgery, orthopedic surgery, and otolaryngology [2,5]. More recently, the CMS finalized a nearly 3% decrease in Medicare reimbursements for cardiothoracic surgery, starting in 2025, which exacerbates the problem. Interventional cardiology has witnessed similar declines in reimbursement [6].
An analysis of utilization and reimbursements for surgical and transcatheter mitral valve procedures was recently published [7]. However, an analysis of Medicare reimbursement trends for surgical and transcatheter valvular procedures has not been performed and is of particular interest, given the growth of transcatheter valvular procedures over the last two decades. This study aimed to quantify contemporary changes in physician Medicare reimbursement for surgical and transcatheter valvular procedures.
2. Methods
2.1. Data Sources
Publicly available data from CMS were used to identify annual physician reimbursement fees for four procedures: surgical aortic valve replacement (SAVR), transcatheter aortic valve replacement (TAVR), mitral valve repair (MVr), and MitraClip. Using the CPT code for each procedure, the CMS Physician Fee Schedule Look-Up Tool was used to extract reimbursement data over the study period (2015–2023) [8]. Physician reimbursement fees were adjusted for inflation into 2023 U.S. dollars using the Consumer Price Index, a measure of monetary inflation, for July of each year [9]. Because all data analyzed in this study were publicly available, institutional review board approval was not required.
2.2. Outcome Measures
The primary outcomes were temporal trends of physician reimbursement fees for SAVR, TAVR, MVr, and MitraClip. Reimbursement trends were calculated as (1) the average annual U.S. dollar decline, (2) the average annual percent change, and (3) the total percent change over the study period.
2.3. Statistical Analysis
Temporal changes were assessed using linear regression. Resultant annual changes were reported as the overall average for each group with corresponding 95% confidence intervals (95%CI). All data analyses were performed using Stata Version 17.0. Two-sided p-values < 0.05 were considered significant.
3. Results
Between 2015 and 2023, inflation-adjusted physician reimbursement fees for surgical and transcatheter valve procedures significantly declined, with average annual decreases of $94.29 (95%CI: 65.27–123.30) for SAVR, $83.80 (63.68–103.92) for TAVR, $99.22 (95%CI: 68.65–129.78) for MVr, and $80.65 (58.93–102.36) for MitraClip. These occurred in the setting of an inflationary growth of 28% over the same time period. Declines corresponded to average annual percent changes of −3.7% (SAVR), −5.1% (TAVR), −3.7% (MVr), and −4.1% (MitraClip)—representing a collective decline in physician reimbursement fee per patient of $784.96 (SAVR), $624.73 (TAVR), $823.54 (MVr), and $706.12 (MitraClip) over the nine-year study span. The combined total decrease over the study period was 28.5% (8.5% decrease before adjusting for inflation): 25.8% (SAVR; Figure 1A), 34.2% (TAVR; Figure 1B), 25.8% (MVr; Figure 1C), and 28.3% (MitraClip; Figure 1D). Reimbursement decreases did not vary by procedure type (p = 0.595). The differences between surgical (SAVR and MVr) and transcatheter (TAVR and MitraClip) approaches were not significant (aortic: p = 0.49, mitral: p = 0.74; Figure 2A). The conversion factor inflation-adjusted), used by the CMS to convert Relative Value Units to U.S. dollars, has also significantly declined over the study period (R2 = 0.88; p < 0.001), decreasing by 26.3% from 2015 ($46.00) to 2023 ($33.89; Figure 2B). Relative value units remained largely stable across all procedures, except for TAVR, which decreased from 25.13 in 2015 to 22.47 in 2023. SAVR, MVr, and Mitraclip remained stable at 41.32, 43.28, and 32.35, respectively.
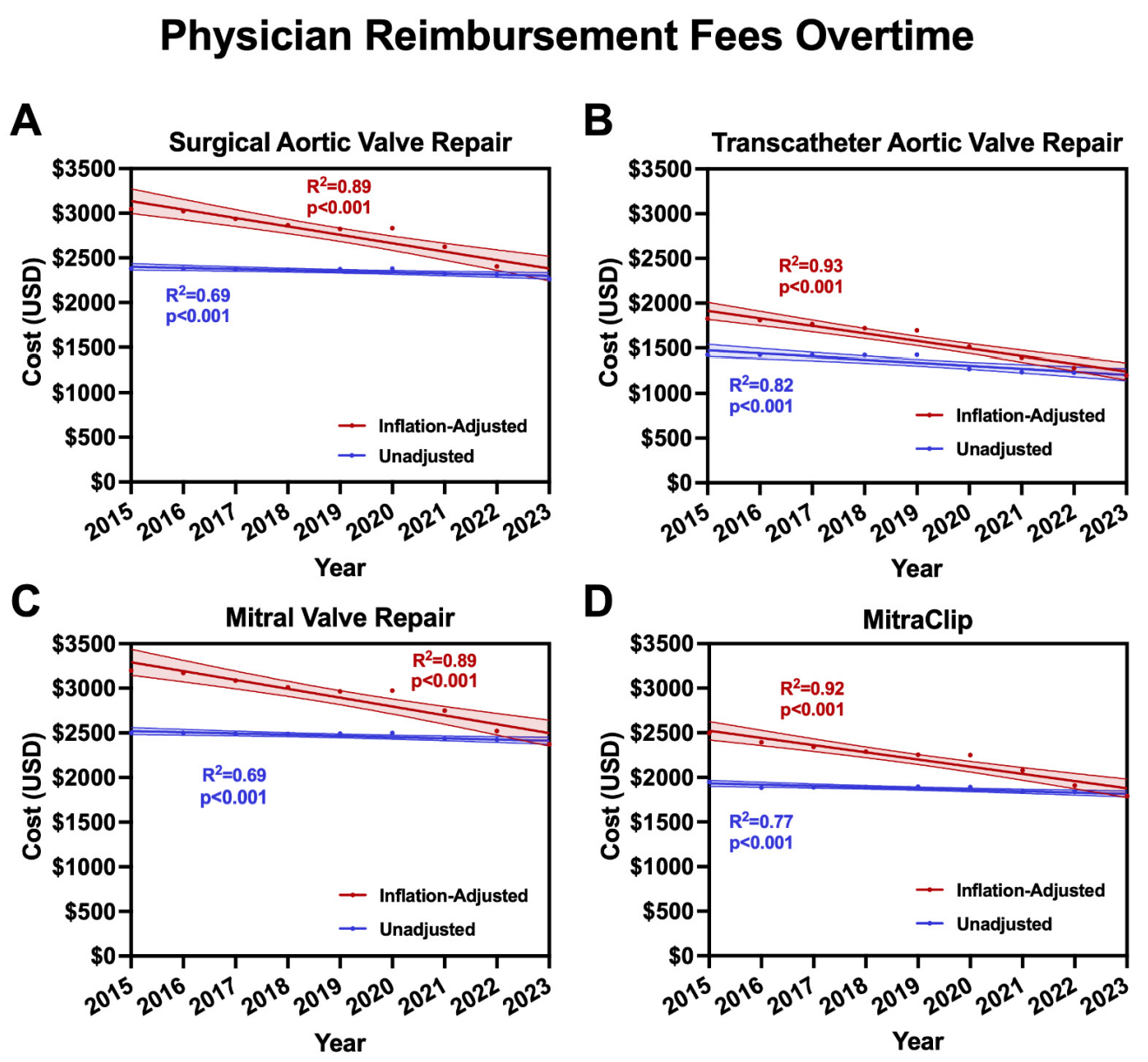
Figure 1. (A) Inflation-adjusted and unadjusted physician repayment fees for surgical aortic valve replacement, (B) transcatheter aortic valve replacement, (C) mitral valve repair, and (D) MitraClip from 2015–2023.
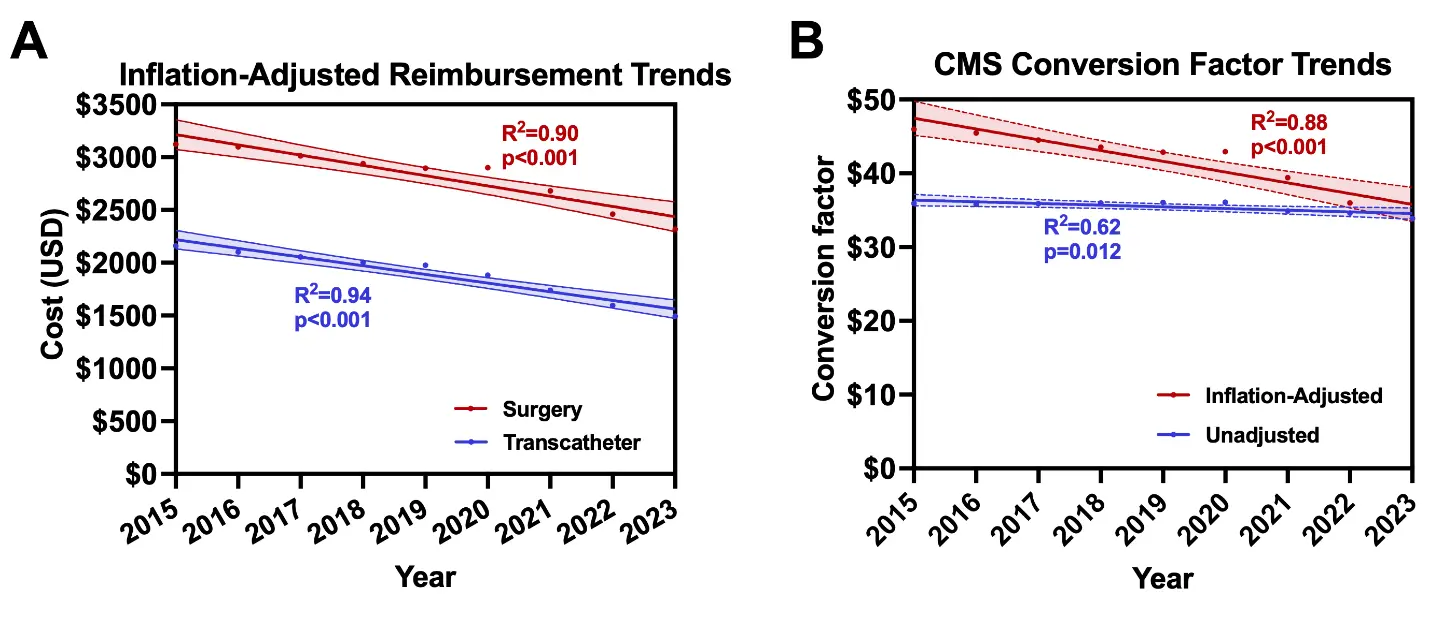
Figure 2. (A) Inflation-adjusted physician reimbursement fees for surgical (SAVR and MVr) and transcatheter (TAVR and MitraClip) valve repair from 2015–2023. (B) Inflation-adjusted and unadjusted Centers for Medicare and Medicaid Services conversion factor rates from 2015–2023.
4. Discussion
This study demonstrates that physician reimbursement for surgical and transcatheter valve procedures have significantly decreased in recent years and appear not to keep pace with rising inflation. From 2015, SAVR, TAVR, MVr, and Mitraclip reimbursements by CMS have decreased by nearly one-third, resulting in approximately a $700 per-procedure decline. These findings have significant implications for the future of interventional and surgical valve procedures and may contribute to downstream negative consequences felt by patients and physicians.
Physician reimbursement declines for transcatheter and surgical aortic and mitral valve procedures over the study period were significant and have occurred in the context of rising healthcare costs, a rising Medicare beneficiary population, and sustained inflation [3,4]. The current CMS reimbursement system does not account for inflation, which was 28% over the nine-year study period. Given the dramatic inflationary growth witnessed over the last decade, it is clear this should be accounted for when calculating physician reimbursement. Beyond the lack of inflationary correction, the CMS has recently proposed further reductions of reimbursement to cardiothoracic surgeons by nearly 3% [10]. Reforms to mitigate such cuts have been proposed by the Society of Thoracic Surgeons and the American College of Surgeons, including an inflationary update mechanism and modernization of the budget neutrality requirement [11]. As the U.S. transitions to a value-based care system, these modifications will be crucial to ensure that patients have access to high-quality care and procedures associated with reduced hospitalizations, improved functionality, and reduced long-term costs.
The reductions in reimbursement by the CMS have not been uniform across specialties. Surgical and transcatheter valve procedures decreased by 28.5% from 2015 to 2023, significantly higher than general surgical procedures, which decreased by 10.8% from 2011 to 2021, but less than reimbursement for cardiac electrophysiology procedures, which have faced striking reductions in CMS reimbursement of up to 30% starting in 2022 [12,13]. Trends in reimbursement also vary significantly by role within the healthcare system. Christensen et al. found a substantial redistribution of reimbursement fees across provider types within the budget-neutral payor system, with reimbursements tripling for non-physician practitioners and declining for physicians, with procedural specialities suffering the largest declines [1]. Although non-physician practitioners play an essential role in high-quality healthcare delivery, drastic increases in their reimbursement at the expense of physicians are inappropriate.
This study has a few important limitations, namely that the data were limited to CMS reimbursement data. As such, the results may not apply to the total reimbursement market for cardiac surgical and interventional procedures. However, reimbursement data from private insurers are generally guided by the CMS Fee Schedule [14]. Medicare beneficiaries represent the largest segment of patients undergoing cardiac intervention, with that proportion expected to rise in the coming years [4]. Thus, the trends described in this study are likely representative of overall market trends in the reimbursement of cardiac surgical and transcatheter interventions.
5. Conclusions
Over the last decade, physician reimbursement for surgical and transcatheter valve procedures have significantly decreased and appear not to keep pace with rising inflation costs. These ongoing declines may threaten access to quality cardiac care in the context of the heart team approach.
Author Contributions
Conceptualization, J.A.T., S.A.H. and C.K.Z.; Methodology, J.A.T. and C.K.Z.; Formal Analysis, J.A.T. and C.K.Z.; Writing—Original Draft Preparation, J.A.T.; Writing—Review & Editing, J.A.T., S.A.H., C.K.Z., D.A.-R., T.K. and K.d.l.C.; Supervision, S.A.H., T.K. and K.d.l.C.
Ethics Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is publically available through the Centers for Medicare & Medicaid Physician Fee Schedule Look-Up Tool.
Funding
This research received no specific grant from public, commercial, or not-for-profit funding agencies. The work described in this manuscript was presented at the 60th Annual Meeting of the Society of Thoracic Surgeons on 28 January 2024.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
Christensen EW, Nicola GN, Rula EY, Nicola LP, Hirsch JA. Medicare Volume Growth and Shift in Payments from Physicians to Non-Physician Practitioners Under Statutory Budget Neutrality. Inq. J. Health Care Organ. Provis. Financ. 2024, 61, 00469580241249076. DOI:10.1177/00469580241249076 [Google Scholar]
-
Treffalls JA, Shah AM, Worrell CM, Treffalls RN, Das NA, Hui DS, et al. Two Decades of Declining Medicare Reimbursement in Cardiac Surgery. Ann. Thorac. Surg. 2023, 116, 845–852. DOI:10.1016/j.athoracsur.2023.06.023 [Google Scholar]
-
Farmer SA, Casale PN, Gillam LD, Rumsfeld JS, Erickson S, Kirschner NM, et al. Payment Reform to Enhance Collaboration of Primary Care and Cardiology: A Review. JAMA Cardiol. 2018, 3, 77–83. DOI:10.1001/jamacardio.2017.4308 [Google Scholar]
-
Gaudette É, Tysinger B, Cassil A, Goldman DP. Health and Health Care of Medicare Beneficiaries in 2030. Forum Health Econ. Policy 2015, 18, 75–96. DOI:10.1515/fhep-2015-0037 [Google Scholar]
-
Singh R, Shahbandi A, Singh A, Li A, Hess R, Collins SAB, et al. U.S. Surgical Practice: 23-Year Trends in Medicare Procedures and Reimbursement. Ann Surg. 2025, 10-1097. DOI:10.1097/SLA.0000000000006912 [Google Scholar]
-
Lata K, Rooney C, Cigarroa JE, Box LC. Medicare Payment Cuts: A Threat to Patient Care. J. Soc. Cardiovasc. Angiogr. Interv. 2023, 2, 100630. DOI:10.1016/j.jscai.2023.100630 [Google Scholar]
-
Shah AM, Almomani AA, Sako EY, Hui DS. Surgical and Transcatheter Mitral Valve Therapy: Medicare Utilization and Reimbursement. Ann. Thorac. Surg. 2024, 118, 164–171. DOI:10.1016/j.athoracsur.2023.09.014 [Google Scholar]
-
U.S. Centers for Medicare & Medicaid Services. Physician Fee Schedule Look-Up Tool. Available online: https://www.cms.gov/medicare/physician-fee-schedule/search/overview (accessed on 10 June 2024).
-
U.S. Bureau of Labor Statistics. Consumer Price Index. Available online: https://www.bls.gov/cpi/ (accessed on 10 June 2024).
-
Calendar Year (CY) 2025 Medicare Physician Fee Schedule Final Rule. Available online: https://www.cms.gov/newsroom/fact-sheets/calendar-year-cy-2025-medicare-physician-fee-schedule-final-rule?_cldee=LGI4gXodJk_7xANrOaIBDq8Rf6Y7vy2Z8MymjeCLqCnhQYnthUtAoQuJSsezUnyD&recipientid=contact-d7a5277de1dc4d94a2673e682386b5ce-3563f7616266402bbf67d51f9128e537&esid=ee8978c5-9398-ef11-8a69-7c1e5266f3e2 (accessed on 10 October 2025).
-
Turner PL. Bolstering Chronic Care Through Physician Payment: Current Challenges and Policy Options in Medicare Part B. Published Online 14 June 2024. Available online: https://www.facs.org/media/p3hj5q3o/acs-response-senate-chronic-care-and-medicare-payment-rfi.pdf?utm_medium=email&utm_source=newsletter_advocacy_brief&utm_campaign=advocacybrief062024 (accessed on 15 August 2024).
-
Hue JJ, Paukovits JL, Bingmer K, Sugumar K, Onders RP, Hardacre JM. Medicare reimbursement for common general surgery procedures has declined over the last decade. Am. J. Surg. 2022, 223, 550–553. DOI:10.1016/j.amjsurg.2021.10.040 [Google Scholar]
-
Liu CF, Krahn AD, Kusumoto F, Selzman KA, Shanker AJ, Zeitler EP, et al. Revaluing ablation therapy: History, recent developments, and future Heart Rhythm Society strategy. Heart Rhythm 2022, 19, 1566–1568. DOI:10.1016/j.hrthm.2022.07.015 [Google Scholar]
-
Smith S. Medicare RBRVS 2022: The Physicians’ Guide. In American Medical Association; American Medical Association: Washington, DC, USA, 2022. [Google Scholar]