Type 2 diabetes mellitus and cardiovascular disease are interrelated conditions that disproportionately affect underserved populations, with compounded risk in communities facing systemic barriers to care. This review synthesizes clinical trial evidence, preclinical research, and public health perspectives to evaluate sitagliptin’s pharmacologic profile, safety, and potential vascular effects, particularly in resource-limited settings. Sitagliptin, the first FDA-approved oral DPP-4 inhibitor, demonstrates weight neutrality, minimal hypoglycemia risk, and renal dosing flexibility. Large cardiovascular outcomes trials confirm cardiovascular neutrality, while preclinical and animal studies suggest possible microvascular benefits. Despite superior cardiovascular outcomes with newer agents like GLP-1 receptor agonists and SGLT2 inhibitors, sitagliptin remains a practical option for patients who cannot access or tolerate these therapies, supported by oral dosing, low side-effect burden, and anticipated generic availability in the US. Its continued value is evident in U.S. safety-net systems such as federally qualified health centers (FQHCs), and globally in low- and middle-income countries where newer drugs remain unaffordable. Achieving meaningful public health impact will require pairing pharmacologic safety with structural access improvements, including expanded insurance coverage, protection of safety-net drug pricing programs, culturally tailored interventions, and inclusive research practices. Sitagliptin illustrates a broader principle in chronic disease care: even safe therapies cannot close disparities until equitable access.
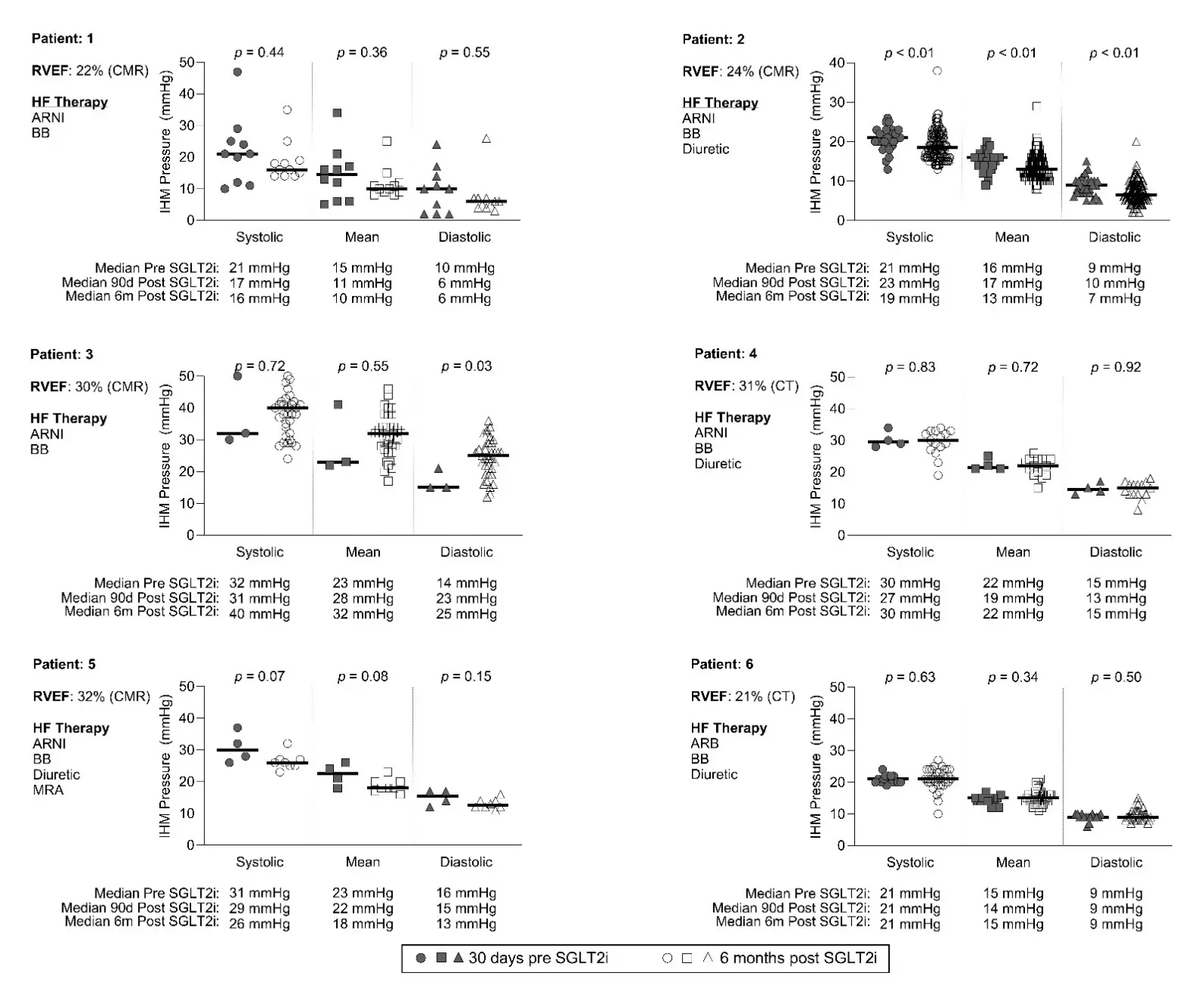
Heart failure (HF) is the leading cause of mortality in adults with congenital heart disease (ACHD), including patients with systemic right ventricles, such as those with dextro-transposition of the great arteries with an atrial switch (DTGA-AS). With more ACHD patients surviving well into adulthood, there is an increase in advanced heart failure (HF) and pulmonary hypertension (PH), many of whom are being treated with SGLT2-inhibitors (SGLT2-i). However, there is a paucity of data supporting SGLT2-i inhibitor use in the ACHD population and on how they may impact pulmonary artery pressures (PAP). This single center retrospective study aimed to evaluate the impact of SGLT2-i on (PAP) in patients with DTGA-AS. Six patients were studied, all male (mean age 41 [range 38–52] years), with a mean systemic right ventricular ejection fraction of 27% (range 22–32%), with an implanted hemodynamic CardioMEMs monitor data were recorded one month prior to medication start and six months afterwards. Half of the patients had normal PAP, and the addition of SGLT2i did not result in a significant change in PAP in all patients. However, half of the patients demonstrated a trend towards improvement. In conclusion, in this study with a small sample size of DTGA-AS patients, there was no significant reduction in PAP.
Absent pulmonary valve syndrome (APVS) is a rare cardiac malformation that is almost always associated with a Fallot-type ventricular septal defect (VSD). More rarely, it can occur with an intact ventricular septum or muscular VSD. The limited number of observations reported in the medical literature affects the quality of prenatal counselling given to the families concerned. We report 3 new cases of APVS without Fallot-type VSD, with 1 case associated with a muscular VSD, and have carried out a review of the literature on this rare malformation. Two of the fetuses had hydrops fetalis and one of these two had intra-uterine death. A 16p13.11 microduplication transmitted by the father was found in one fetus whose post-natal evolution was favorable following surgical ligation of an aneurysmal ductus arteriosus. A newborn with hydrops fetalis had a favorable outcome after spontaneous closure of the ductus arteriosus on the third day of life. Unlike Fallot-type APVS, non-Fallot type APVS is characterized antenatally by the constant presence of a large ductus arteriosus, the absence of aneurysmal pulmonary branches, a high frequency of chromosomal anomalies, but the absence of 22q11 micro deletion. After birth, early closure of the ductus may be indicated in cases of significant heart failure.

Despite its tendency to produce hypotension, propofol is used widely to induce general anesthesia and to facilitate endotracheal intubation in critically ill patients. Both dose reduction and routine co-administration of vasopressors have been used to offset this unfavorable hemodynamic effect in this subset of individuals. There are potential problems associated with each of these corrective measures, however, and criticism of other intravenous hypnotics used for this purpose—particularly etomidate—may be unwarranted. Choice of the appropriate pharmacology to induce anesthesia to assist with intubation should likely be based on individual clinical assessment, together with an understanding of the drug profile and realistic adverse effects.
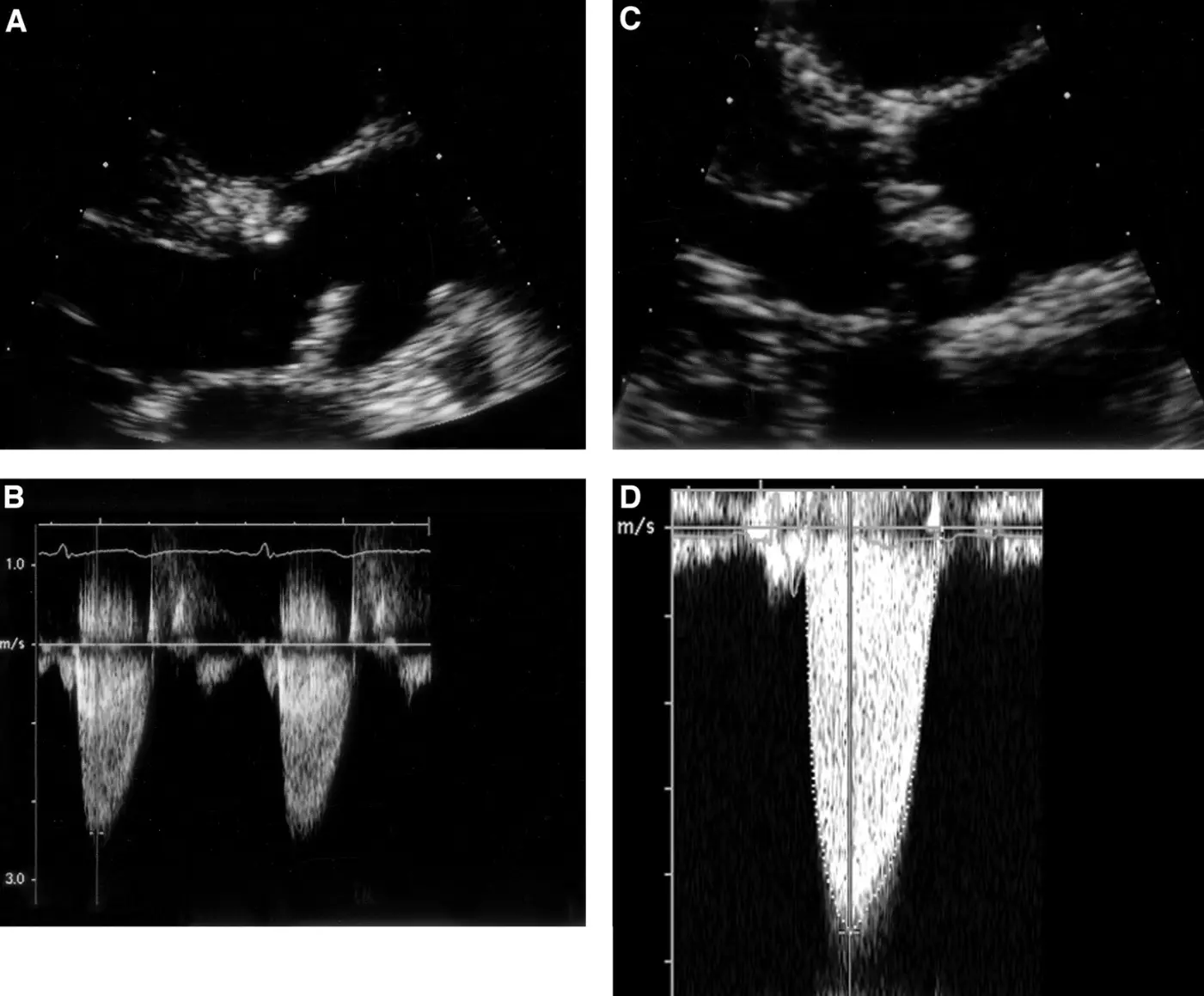
Aortic stenosis (AS) is the most prevalent valvular heart disease in developed nations, with increasing incidence driven by population aging. Early and accurate diagnosis is crucial, as timely intervention significantly improves outcomes. Contemporary imaging plays a central role in the assessment of AS, enabling precise evaluation of valve anatomy, disease severity, left ventricular remodeling, and procedural planning. Transthoracic echocardiography remains the first-line modality, providing essential hemodynamic and structural data. However, limitations in cases of low-flow states, discordant grading, and atypical presentations necessitate adjunctive tools. Transesophageal echocardiography enhances visualization of valve morphology and annular dimensions, particularly for pre-procedural assessment. Cardiac computed tomography (CT) has emerged as a cornerstone in transcatheter aortic valve replacement (TAVR) planning, offering unparalleled spatial resolution for annular sizing, coronary height measurement, and vascular access evaluation. Meanwhile, cardiac magnetic resonance (CMR) provides robust quantification of ventricular volumes, fibrosis, and myocardial strain, serving as a prognostic marker in asymptomatic and borderline cases. The integration of multimodality imaging offers a comprehensive framework, addressing diagnostic ambiguities and guiding individualized management strategies. This review highlights current advances, clinical applications, and future directions in multimodality imaging for AS, emphasizing its pivotal role in optimizing patient selection, risk stratification, and procedural outcomes.