This study evaluated the clinical utility of the HEMOTAG™ recording device—A non-invasive, wearable system that measures cardiac time intervals (CTIs)—in managing patients with acutely decompensated heart failure (ADHF). The prospective, single-center study enrolled 105 patients, including those hospitalized with ADHF and a control group with non-HF-related conditions. Daily measurements of isovolumetric contraction time (IVCT), a key CTI marker, were collected using the HEMOTAG device and compared with NT-proBNP levels obtained on admission and day 3. Among ADHF patients, IVCT decreased in parallel with NT-proBNP levels, indicating volume status improvement with therapy. In contrast, the control group showed no significant change in IVCT or NT-proBNP. An IVCT ≥ 40 ms demonstrated strong sensitivity and specificity to detect ADHF (NT-proBNP ≥ 1800 pg/mL). These findings suggest that IVCT trends measured by HEMOTAG correlate with short-term treatment response in ADHF and could offer a non-invasive method to guide heart failure management. The technology demonstrated feasibility, safety, and clinical relevance, supporting its potential role in future remote management strategies.

Atrial fibrillation (AF) is the most common
cardiac arrhythmia and is associated with increased morbidity and mortality.
Early prediction of AF episodes remains a clinical challenge. This study aimed
to generate physiopathological hypotheses for AF onset by analyzing
correlations among heart rate variability (HRV) parameters in patients
monitored via long-term Holter ECG. We utilized the IRIDIA-AF database,
comprising 1319 paroxysmal AF episodes from 872 patients. An XGBoost machine
learning model was developed to predict AF onset within 24 h using short- and
long-term HRV features, fragmentation indices, and non-linear metrics extracted
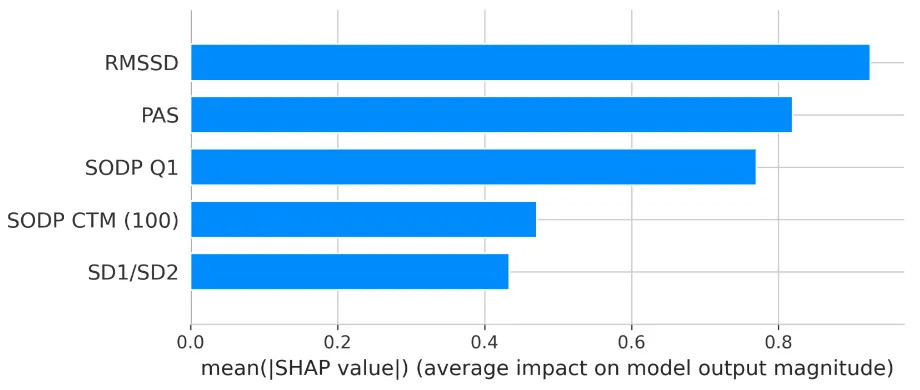
during sinus rhythm. Model interpretation was performed using SHapley Additive
exPlanations (SHAP) values, and dimensionality reduction techniques were
applied for data visualization. The model achieved an area under the receiver
operating characteristic curve of 0.919 and an area under the precision-recall
curve of 0.919, with high accuracy, sensitivity, and specificity. Key
predictive features included short-term vagal activity, HRV fragmentation
indices, and non-linear parameters, highlighting the role of the autonomic
nervous system in AF initiation. Our findings suggest that distinct
physiological profiles, detectable via HRV, may underlie AF susceptibility and
could inform personalized monitoring and prevention strategies.
Traditional indices such as dp/dt max remain widely used in assessing ventricular contractility, yet their load-dependence limits clinical precision, particularly during dynamic hemodynamic shifts. This letter to the Editor advocates for a more physiologically grounded approach using dual pressure catheters equipped with two high-fidelity sensors, one in the left ventricle (LV) and one in the aorta, to capture real-time pressure gradients and valve events with high temporal resolution. When combined with transient inferior vena cava occlusion (IVCO), this setup enables accurate identification of the true end-systolic (ES) point, typically marked by dp/dt min or the dicrotic notch on the aortic pressure waveform. This method allows for the construction of more physiologically valid end-systolic pressure-volume relationships (ESPVR). It introduces the novel peak pressure end-systolic pressure-volume relationship (PPESPVR) model, which links peak LV pressure to the ES point within a single cardiac cycle. The resulting volume intercept (Vint) and end-systolic fraction (ESF) offer new insights into myocardial performance under varying preload and afterload conditions, without requiring extensive hemodynamic manipulation. This dual-sensor approach not only enhances diagnostic accuracy but also opens the door to real-time, patient-specific contractility assessment in both research and clinical settings.