1. Introduction
Post-traumatic stress disorder (PTSD) and major depressive disorder (MDD) are prevalent and often comorbid psychiatric conditions characterized by emotional, cognitive, and somatic symptoms. Despite differences in etiology—trauma exposure for PTSD and a broader range of psychosocial factors for MDD—both disorders share overlapping pathophysiological features, including dysregulated stress responses, impaired neuroplasticity, and heightened systemic inflammation. In recent years, increasing attention has been directed toward immune dysregulation—particularly cytokine-mediated signaling—as a central contributor to the onset and maintenance of both PTSD and MDD [
1,
2]. However, the precise mechanisms linking immune alterations to behavioral symptoms remain incompletely understood, representing a critical gap in the literature.
We hypothesize that dysregulation of peripheral and central cytokine signaling is a shared pathophysiological mechanism driving the development and persistence of PTSD and MDD, contributing to structural and functional brain alterations that underlie core affective and cognitive symptoms.
Cytokines are small, secreted proteins that orchestrate immune responses and mediate communication between immune and neural systems. They are broadly categorized into pro-inflammatory (e.g, IL-1β, IL-6, TNF-α) and anti-inflammatory (e.g, IL-10) types. Under chronic stress, sustained production of pro-inflammatory cytokines can disrupt homeostatic brain-immune interactions, contributing to synaptic remodeling, hippocampal atrophy, altered neurotransmission, and dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis. These neurobiological alterations are implicated in core symptoms of PTSD and MDD, such as anhedonia, hyperarousal, and cognitive impairment.
Early studies by Yirmiya and colleagues in the 1990s demonstrated that peripheral administration of IL-1β in rodents could induce behavioral symptoms resembling depression—effects that were reversed by chronic, but not acute, antidepressant treatment [
3]. These findings provided initial evidence for a causal role of cytokine signaling in mood regulation. Human studies further supported these observations, showing that experimental immune activation (e.g, through endotoxin or vaccine challenge) could temporarily induce depressive symptoms and cognitive dysfunction, underscoring the translational relevance of cytokine-mediated pathways [
4,
5].
Subsequent research in PTSD populations has also revealed elevated levels of peripheral pro-inflammatory cytokines, including IL-2, IL-6, IL-1β, and TNF-α, indicating a chronic inflammatory state [
6,
7,
8]. These immune alterations have been associated with changes in brain structure and function, including reduced hippocampal volume and altered limbic connectivity, potentially contributing to the pathogenesis of PTSD and its frequent overlap with MDD.
In this review, we synthesize current findings on the central role of cytokines in PTSD and MDD, with an emphasis on mechanisms of pathogenesis, clinical correlations, and therapeutic implications. We examine how neuroimmune dysregulation contributes to symptom expression, the moderating effects of genetic and environmental risk factors, and the potential of anti-inflammatory and immunomodulatory treatments. In doing so, we highlight emerging precision medicine approaches—including biomarker-guided stratification and machine learning techniques—that may facilitate more targeted and effective interventions.
2. Literature Synthesis: Cytokine in PTSD
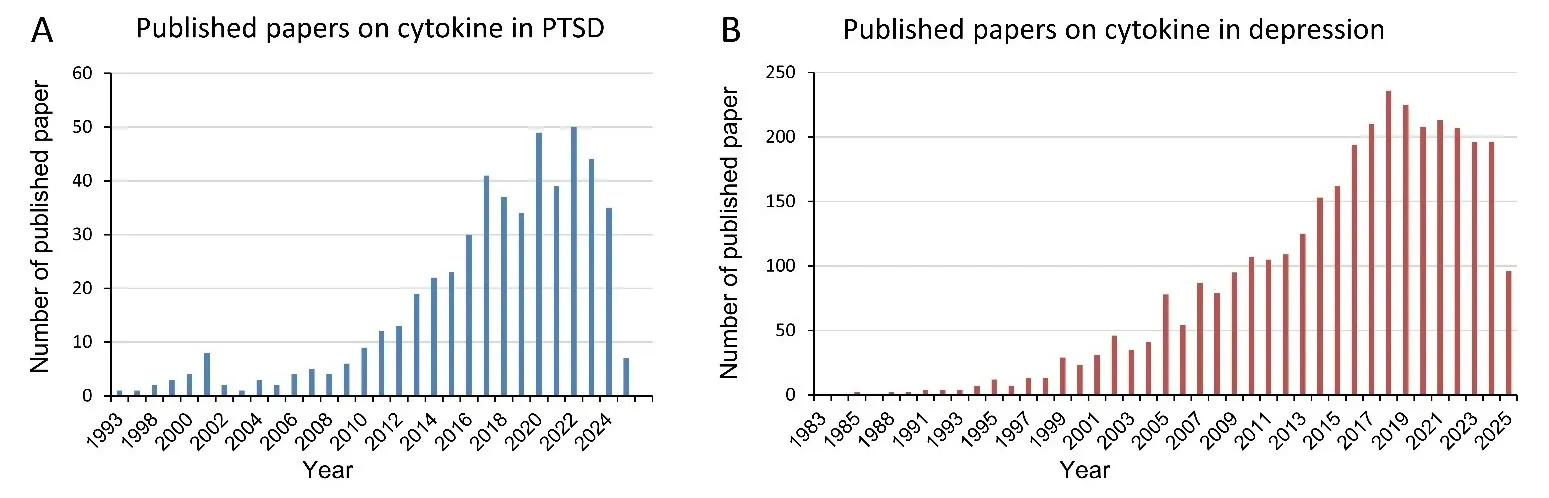
Searched in PubMed using the keywords ‘cytokine and PTSD’ and ‘cytokine and depressive disorder’, we found that there are 440 and 2884 published papers on PTSD and on depressive disorder by 29 April 2025, respectively, showing that cytokines in PTSD and MDD draw more interest over time ().
. Publications on cytokine in PTSD or MDD. shows the trend of published literatures on cytokine in PTSD (<b>A</b>) or MDD (<b>B</b>) using PubMed search engine.
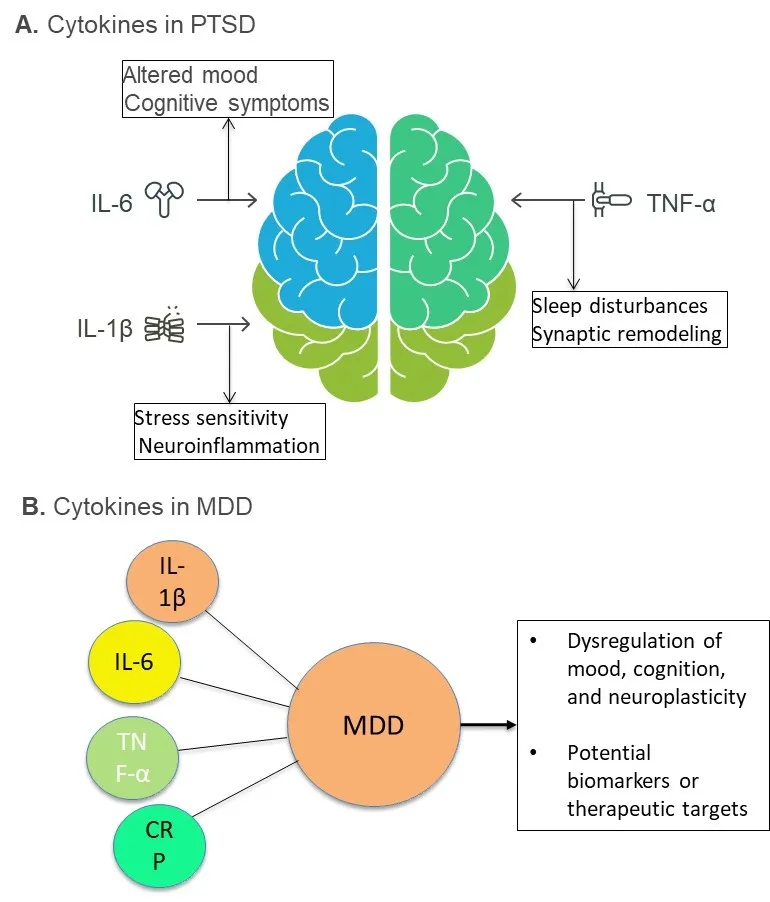
Trauma can result in a significant psychological and physiological stress response, leading to the release of inflammatory cytokines and subsequent immune cell dysfunction (A). This cascade may promote chronic inflammation and cause short- or long-term immune dysregulation, which contributes to the development or exacerbation of PTSD symptoms. For example, veterans of the Gulf War showed a remarkable higher prevalence of immune-related disorders such as rheumatism, sarcoidosis, and multiple sclerosis, suggesting the connection between war-related stress and immune dysfunction [
9]. Research has shown significant changes in circulating cytokines and chemokines—key mediators of immune signaling—in individuals with PTSD. These include interferons (IFNs), interleukins (ILs), tumor necrosis factors (TNFs), lymphokines, and chemokines [
7,
10,
11]. Moreover, remarkably elevated peripheral levels of cytokines were observed. IL-2, IL-4, IL-6, IL-8, IL-10, and TNF-α compared were significantly higher in the patients with PTSD compared to age- and sex-matched healthy controls [
11]. In addition, cross-sectional and longitudinal studies have demonstrated elevated levels of pro-inflammatory cytokines-particularly IL-6, TNF-α, and IL-1β-in individuals with PTSD [
6,
7,
11,
12,
13]. Meta-analyses reveal that PTSD is associated with higher peripheral concentrations of IL-6 and TNF-α, two canonical markers of systemic inflammation [
14,
15]. Elevated IL-6 has been linked to increased severity of re-experiencing symptoms and hyperarousal, while TNF-α correlates with impaired cognitive performance and altered sleep architecture in PTSD patients [
16].
. Immune response in PTSD (panel (<b>A</b>)). Illustration of key pro-inflammatory cytokines implicated in the pathophysiology of post-traumatic stress disorder (PTSD). Interleukin-6 (IL-6), interleukin-1β (IL-1β), and tumor necrosis factor-alpha (TNF-α) are shown interacting with the brain, reflecting their roles in neuroimmune dysregulation. Elevated IL-6 is associated with altered mood and cognitive symptoms; IL-1β is linked to stress sensitivity and neuroinflammation; TNF-α is implicated in sleep disturbances and synaptic remodeling. These cytokines contribute to the chronic low-grade inflammation observed in individuals with PTSD. Panel (<b>B</b>) shows the inflammatory markers associated with MDD. Diagram illustrating key inflammatory markers elevated in individuals with MDD. Interleukin-1β (IL-1β), interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and C-reactive protein (CRP) are consistently found at increased levels in patients with MDD. These pro-inflammatory molecules are implicated in the dysregulation of mood, cognition, and neuroplasticity, and may serve as potential biomarkers or therapeutic targets in the treatment of MDD.
Chemokines, a subclass of cytokines involved in immune cell trafficking and neuroimmune communication, also show altered profiles in PTSD. Studies report increased levels of CCL2 (MCP-1), CXCL8 (IL-8), and CXCL10 (IP-10) in both blood and cerebrospinal fluid (CSF) samples [
17,
18,
19]. Our previous study using both the before-and-after and the case-control design revealed that CCL2, CCL15, CCL22, CCL25, CXCL2, and CXCL12 are associated with PTSD onset; CCL3, CXCL11, and CXCL16 are related to stress response. CCL13, CCL20, and CXCL6 were possible PTSD risk markers; CX3CL1 is a potential resilience marker [
20]. While CCL11, CCL13, CCL20, and CCL25 are correlated to PTSD symptom severity [
20], elevated pre-deployment levels of IL-6 and CCL2 could predict post-deployment PTSD symptoms [
21]. More interestingly, tenacious elevations of CRP and IL-10 were associated with delayed-onset PTSD in the post-deployment individuals, indicating the potential utility of immune markers for PTSD [
22]. However, the literature has presented inconsistent findings. For instance, while studies reported elevated levels of IL-1β [
6,
12], IL-6 [
13], and TNF-α [
7] in the plasma of PTSD patients [
11], others have found no statistically significant differences in IL-1β [
7], IL-6 [
6,
7], or IL-8 [
6] levels between the cases and controls. These discrepancies may be attributed to several confounding variables, including differences in the type and timing of trauma (e.g, childhood
vs. adulthood), the chronicity or immediacy of trauma exposure, civilian
vs. military populations, geographical variations, the use of psychotropic medications, and methodological differences in biomarker detection (e.g, ELISA
vs. Western blot, single versus multiplex assays, saliva-
vs. blood-based sampling).
2.2. Cytokine in MDD
Alterations in cytokine levels have been observed in MDD, a commonly comorbid condition with PTSD. Cytokines may be associated with depressive symptoms [
23]. An animal study showed that injecting rats with endotoxin, which stimulates the immune system, leads to depression-like behavior [
3]. Similarly, immune challenges in humans using endotoxin administration have resulted in emotional and cognitive disturbances, indicating a role for cytokines in regulating mood and cognitive function [
24] (B).
Patients with MDD exhibit elevated inflammatory markers. IL-1β, IL-6, TNF-α, and C-reactive protein (CRP) are consistently upregulated in individuals with MDD compared to healthy controls [
4,
25,
26,
27]. Moreover, cytokine elevation is correlated with MDD severity and treatment resistance [
28]. Notably, longitudinal studies have shown that baseline elevations in IL-6 and CRP could predict future onset of depressive symptoms, suggesting a causal role in disease development [
29,
30]. Following acute trauma exposure, IL-6 and IL-1RA (IL-1 receptor antagonist) levels were significantly increased and associated with increased risk of developing MDD [
31]. These findings underscore the prognostic value of inflammatory markers and support their inclusion in early screening protocols for stress-related psychopathology.
Growing data point to increased levels of CCL2, CCL11, and CXCL10, particularly in individuals with treatment-resistant MDD [
32,
33,
34]. These chemokines are known to promote leukocyte infiltration into the central nervous system (CNS), supporting the hypothesis that MDD is, at least in part, an inflammatory disorder of the brain.
CRP is correlated with [
35] and a risk factor for MDD [
36]. However, it is present only in a subset of individuals with MDD [
37]. The inconsistency is probably related to many factors, e.g, the size of samples and symptom heterogeneity. In a large sample size (
n = 4157), Moriarity et al. report that the elevated CRP group has greater symptom connectivity (stronger total associations between symptoms). Difficult concentrating and psychomotor difficulties have higher expected influence (concordance with other symptoms) in the elevated CRP group. In addition, several symptoms are moderated by CRP [
38]. Also, a meta-analysis in 5166 patients and 5083 controls out of 107 studies demonstrates that levels of CRP, IL-3, IL-6, IL-12, IL-18, sIL-2R, and TNFα are significantly higher in patients with MDD. Furthermore, Moriarity et al. report CRP is simultaneously associated with latent depression, appetite, and fatigue after analyzing a 27,730 adults [
39].
2.3. Shared Immune Profiles by Both PTSD and MDD
PTSD and MDD frequently co-occur, with comorbidity rates as high as 50% in some populations [
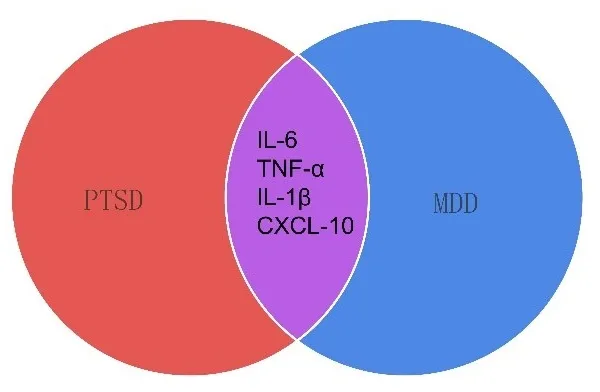
40]. They often share inflammatory profiles with each other. Both disorders show elevations in IL-6, TNF-α, IL-1β, and chemokines like CXCL10. Therefore, this convergence suggests common upstream drivers, such as chronic stress, hypothalamic-pituitary-adrenal (HPA) axis dysregulation, and altered glucocorticoid sensitivity, which are known to modulate immune function [
41,
42]. Trauma-exposed individuals who developed either PTSD, depression, or both demonstrated that the magnitude and duration of cytokine dysregulation may differ depending on the clinical outcome. While elevated IL-6 and TNF-α were observed in all trauma-exposed individuals, those with comorbid PTSD and MDD exhibited the highest cytokine levels [
43], showing a possible additive or synergistic inflammatory burden in dual-diagnosis cases ().
. Shared and distinct inflammatory profiles in PTSD and MDD. Venn diagram illustrating the overlap in immune dysregulation between post-traumatic stress disorder (PTSD) and major depressive disorder (MDD). Both disorders exhibit shared immune signatures, including elevated pro-inflammatory cytokines such as IL-6, IL-1β, and TNF-α. These overlapping inflammatory markers suggest a common pathophysiological mechanism underlying stress-related psychiatric conditions. Disorder-specific immune patterns may also exist, but are not depicted here.
3. Mechanistic Pathways Linking Immune Dysregulation to PTSD
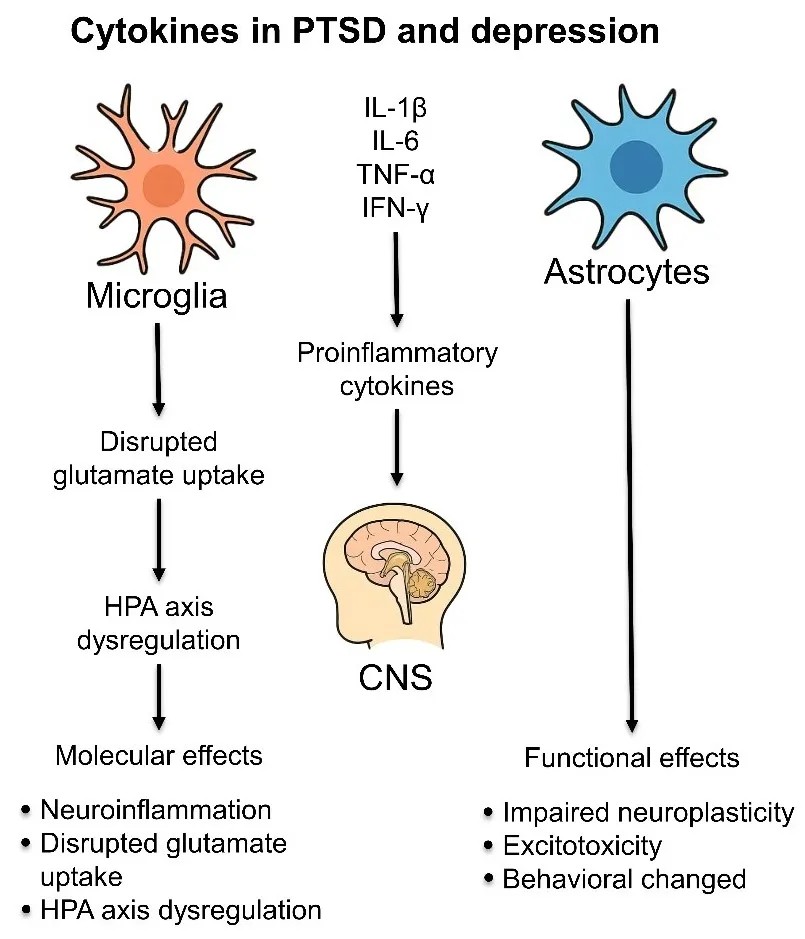
A complex network of neuroimmune interactions underpins the relationship between immune system dysfunction and PTSD. Cytokines may link peripheral immune activation to CNS alterations that led to the onset of psychiatric symptoms. Here, we summarize the major mechanistic pathways through which immune dysregulation contributes to PTSD ().
. Neuroimmune mechanisms linking cytokine dysregulation to depression and PTSD pathology. This schematic illustrates how peripheral and central pro-inflammatory cytokines (e.g, IL-1β, IL-6, TNF-α, IFN-γ) influence central nervous system (CNS) function in the context of post-traumatic stress disorder (PTSD) and major depressive disorder (MDD). Stress and trauma activate the immune system, leading to increased peripheral cytokine release and blood-brain barrier (BBB) permeability. Cytokines access the brain via humoral routes or activating afferent nerves (e.g, vagus nerve), subsequently activating glial cells—particularly astrocytes and microglia. Activated astrocytes release further cytokines and reduce glutamate clearance by downregulating excitatory amino acid transporters (EAAT1/2), contributing to excitotoxicity, synaptic dysfunction, and impaired neurogenesis, especially in the hippocampus and prefrontal cortex. These changes are associated with core symptoms of depression and PTSD, including cognitive deficits, anhedonia, and hyperarousal. Cytokine signaling modulates HPA axis activity by altering corticotropin-releasing hormone (CRH), adrenocorticotropic hormone (ACTH), and glucocorticoid receptor sensitivity, thereby sustaining maladaptive stress responses. Chronic neuroinflammation reinforces behavioral pathology and may define a biological subtype of inflammatory-driven mood and trauma-related disorders.
Psychological stress activates the HPA axis and the sympathetic nervous system, leading to the release of glucocorticoids and catecholamines. Acute stress typically suppresses immune activity
via glucocorticoid-mediated anti-inflammatory effects. However, chronic or repeated stress can result in glucocorticoid receptor resistance in immune cells, impairing the resolution of inflammation and promoting a sustained pro-inflammatory state [
44,
45,
46].
This paradoxical activation of the immune system may increase production of pro-inflammatory cytokines (e.g, IL-1β, IL-6, TNF-α) and chemokines (e.g, CXCL8, CCL2), which can then influence brain function through both humoral and neural pathways [
47].
3.2. Cytokine Signaling Across the Blood-Brain Barrier
Pro-inflammatory cytokines may affect CNS processes through several mechanisms: (1) passive diffusion
via regions with reduced blood-brain barrier (BBB) integrity (e.g, circumventricular organs), (2) active transport mechanisms, (3) signaling through vagal afferent neurons, and (4) activation of endothelial cells to release secondary messengers into the brain parenchyma [
48,
49,
50]. Once in the brain, cytokines can directly interact with neurons and glial cells to modulate neurobiological processes relevant to mood and stress responses, including neurotransmitter metabolism, neuroendocrine regulation, and synaptic plasticity.
3.3. Microglial Activation and Neuroinflammation
Microglia, the resident immune cells of the CNS, play a central role in mediating the neuroinflammatory effects of peripheral cytokine signaling. Chronic peripheral inflammation primes microglia, making them hyperresponsive to subsequent stimuli. This leads to exaggerated production of pro-inflammatory mediators such as IL-1β, TNF-α, and reactive oxygen species (ROS) within the brain [
47,
51,
52]. Sustained microglial activation has been implicated in hippocampal atrophy, reduced neurogenesis, and impaired synaptic function in patients with PTSD and MDD [
53]. Neuroinflammation also disrupts the balance between excitatory and inhibitory neurotransmission, contributing to anxiety, anhedonia, and cognitive deficits commonly seen in these disorders. Chronic stress activates microglial P2Y12 receptors, leading to synaptic loss in the prefrontal cortex; this synaptic remodeling is associated with behavioral deficits relevant to depression [
54]. Moreover, stress may cause microglia to deviate from their finely tuned homeostasis, as both clinical and preclinical studies show. Triggering factors include dysregulation of the neuroendocrine system, the noradrenergic system, the gut-brain axis, and an imbalance between pro- and anti-inflammatory milieus composed of diverse cytokines and neurotransmitters. Therefore, functional changes in microglia may strongly influence neuronal network activity through dysregulated cytokine secretion, ultimately contributing to pathological outcomes under stress conditions [
55].
3.4. Impact on Monoaminergic Systems
Inflammatory cytokines impact monoaminergic neurotransmission by altering the synthesis, reuptake, and metabolism of key neurotransmitters such as serotonin, dopamine, and norepinephrine. For instance, IL-1β and IFN-α upregulate the enzyme indoleamine 2,3-dioxygenase (IDO), which degrades tryptophan—the precursor to serotonin—into kynurenine [
56,
57]. This shift not only reduces serotonin availability but also leads to the accumulation of neurotoxic kynurenine metabolites (e.g, quinolinic acid), which can impair glutamatergic signaling and promote neurotoxicity [
58]. These processes contribute to the development of symptoms such as low mood, fatigue, and impaired cognition, which are often seen in PTSD or MDD.
3.5. Disruption of Neuroendocrine Feedback Loops
Inflammatory cytokines interfere with HPA axis regulation by influencing the release and receptor sensitivity of corticotropin-releasing hormone (CRH), adrenocorticotropic hormone (ACTH), and cortisol. For example, IL-6 and TNF-α can increase CRH expression in the hypothalamus, leading to elevated cortisol levels [
59,
60,
61]. Over time, chronic cortisol exposure and cytokine-induced glucocorticoid receptor resistance contribute to impaired feedback inhibition of the HPA axis—a hallmark feature in PTSD and MDD [
62,
63,
64]. IL-6 can directly stimulate the HPA axis independently of CRH. IL-6 administration significantly increased plasma ACTH levels in both wild-type and CRH knockout mice. The findings suggest that IL-6 can act directly on pituitary corticotrophs and adrenal cells, influencing ACTH and corticosterone release, thereby modulating the HPA axis during immune activation [
65]. Compared to IL6, IL-1 was a more potent activator of the HPA axis [
66].
3.6. Chemokine-Mediated Neuroplasticity and Neural Circuit Remodeling
In addition to their roles in immune cell trafficking, chemokines directly influence neurodevelopment, synaptic plasticity, and neurogenesis. Dysregulated expression of chemokines such as CXCL12 and CCL2 in response to chronic stress is associated with impaired adult hippocampal neurogenesis and altered neuronal connectivity in limbic regions [
67,
68].
Altered chemokine signaling may contribute to the structural and functional brain changes observed in PTSD and MDD, including reduced hippocampal and prefrontal cortex volumes and altered amygdala reactivity. These brain alterations correlate with symptom domains such as emotional dysregulation, impaired memory, and heightened threat sensitivity.
4. Clinical Implications: Diagnostic and Prognostic Value
Understanding the clinical implications of immune dysregulation in PTSD and MDD has opened new avenues for biomarker discovery, personalized treatment approaches, and improved prediction of disease trajectory. Cytokines and chemokines, due to their dynamic responsiveness to stress and neurobiological effects, are emerging as potential tools for diagnostic classification, prognostic evaluation, and therapeutic monitoring ().
. Exploring cytokines and chemokines in mental health. Conceptual model illustrating the implications of immune dysregulation in post-traumatic stress disorder (PTSD) and depression. Chronic alterations in immune signaling, particularly involving cytokines and chemokines, may contribute to disease pathophysiology and serve as a foundation for translational applications. These include: (1) biomarker discovery to aid in diagnosis and monitoring, (2) personalized treatment approaches guided by individual immune profiles, and (3) prediction of disease trajectory and treatment response. This framework supports the development of precision psychiatry strategies targeting immune-related mechanisms.
The identification of reliable biomarkers for PTSD and MDD has long been a challenge due to the heterogeneity of these disorders. Recent findings suggest that specific inflammatory profiles may help differentiate patients with psychiatric conditions from healthy individuals and even distinguish subtypes within disorders.
In PTSD, elevated peripheral levels of IL-6, TNF-α, and CRP have been consistently reported, with some studies proposing thresholds that differentiate PTSD patients from trauma-exposed but resilient individuals [
69,
70,
71,
72]. Similarly, in MDD, meta-analyses have shown that elevated IL-1β, IL-6, and CRP levels are associated with the presence of MDD [
73]. The integration of inflammatory markers with clinical interviews and neuroimaging may improve diagnostic accuracy, especially in ambiguous or comorbid presentations.
Importantly, chemokines such as CCL2, CXCL10, and CX3CL1 are gaining attention due to their specificity for neuroimmune pathways. For example, elevated CXCL10 levels are associated with intrusive re-experiencing symptoms in PTSD, while CCL11 elevation has been linked to cognitive dysfunction in MDD [
74,
75].
4.2. Prognostic Utility and Risk Prediction
Longitudinal studies have highlighted the prognostic potential of cytokines and chemokines in predicting the onset and course of stress-related disorders. Elevated baseline levels of IL-6, IL-10, or CRP have been associated with an increased risk of developing PTSD or MDD following trauma exposure, suggesting that immune activation precedes symptom emergence in vulnerable individuals [
21,
22,
39,
76,
77].
Additionally, persistently elevated inflammatory markers are associated with chronicity and poorer outcomes. For instance, PTSD patients with sustained elevations in IL-6 and CRP are more likely to exhibit treatment resistance and comorbid conditions such as cardiovascular disease [
78]. In MDD, high IL-1β and IL-6 levels have been linked to poor response to standard antidepressant therapies, reinforcing the need for inflammation-informed treatment selection [
79].
4.3. Stratification and Personalized Medicine
Cytokine and chemokine profiles may aid in stratifying patients into biologically distinct subgroups, thereby facilitating personalized interventions. Several studies have identified a subset of patients with high inflammation (“inflammatory biotype”) who may benefit from adjunctive anti-inflammatory therapies or specific antidepressants with immunomodulatory effects [
80,
81,
82].
Trauma and its associated PTSD have been linked to elevated inflammation in numerous studies. Systemic inflammation, in turn, has been implicated in the pathophysiology of several common chronic physical diseases that are more prevalent following trauma. Moreover, inflammation may contribute to the development of PTSD and depression symptoms. In PTSD, immune profiling may help distinguish individuals more likely to benefit from exposure-based therapies versus those who might respond better to interventions targeting systemic inflammation, such as aerobic exercise, mindfulness-based stress reduction, or pharmacological agents like minocycline or ketamine [
83,
84,
85]. Research suggests that adjunctive anti-inflammatory therapies and certain antidepressants with immunomodulatory effects may offer benefits in treating PTSD [
86].
This precision psychiatry approach has been explored through the use of anti-cytokine therapies. The anti-cytokine drug infliximab, a TNF-α inhibitor, has been shown to reduce depressive symptoms, particularly in patients with elevated baseline C-reactive protein (CRP) levels. Clinical trials have demonstrated significant reductions in anhedonia and depressive symptoms. However, the efficacy of infliximab is not generalized across all patients; studies indicate that its effectiveness is largely limited to individuals with higher baseline inflammatory biomarkers, including high-sensitivity CRP (hs-CRP) [
87]. In addition, non-steroidal anti-inflammatory drugs (NSAIDs) and cytokine inhibitors have been found to exhibit antidepressant effects. Anti-inflammatory agents have been examined in the treatment of depression and have yielded positive results [
87,
88,
89,
90,
91]. Meta-analysis studies showed that anti-inflammatory agents reduced depressive symptoms, with higher response and remission rates when used alongside antidepressants. A meta-analysis of 14 RCTs on various non-steroidal anti-inflammatory drugs (NSAIDs) and cytokine inhibitors suggested that these interventions reduced depressive symptoms compared with placebo, in both patients with depression and those with primary inflammatory disorders and comorbid depressive symptoms [
92]. However, there was a significant heterogeneity among included studies. Another meta-analysis of 30 RCTs suggested that anti-inflammatory agents, including NSAIDs, omega 3 fatty acids, statins, and minocyclines, reduced depressive symptoms and resulted in higher response and remission rates compared with placebo, an effect that was more pronounced when the anti-inflammatory agents were used as adjunctive treatments to antidepressants, rather than monotherapies [
93] This finding illustrates the value of cytokine-based stratification in enhancing treatment efficacy and minimizing unnecessary exposure to ineffective therapies.
4.4. Integration into Multimodal Assessment Tools
As stand-alone markers, cytokines and chemokines may have limited specificity. However, their integration into multimodal diagnostic models—including neuroimaging, genetic, epigenetic, and behavioral data—could enhance clinical utility. Machine learning approaches have begun to identify immune-related biosignatures that predict PTSD and MDD onset, symptom clusters, and treatment responses with greater accuracy than clinical assessments alone [
94,
95,
96].
Moreover, dynamic changes in inflammatory markers may serve as early indicators of therapeutic response. A decrease in IL-6 or CRP following psychotherapy or pharmacotherapy has been associated with symptomatic improvement, suggesting their utility in monitoring treatment efficacy [
97]. Elevated levels of CRP, IL-6, and TNF-α were more pronounced in female versus male MDD patients, while one meta-analysis found that the three cytokines were significantly elevated at baseline in MDD patients, but their treatment trajectories differed [
98,
99].
5. Therapeutic Targeting of Cytokine and Chemokine Pathways
As the role of inflammation in the pathophysiology of PTSD and MDD becomes increasingly evident, there is growing interest in immunomodulatory therapies that specifically target cytokine, including chemokine, signaling. These strategies include repurposing anti-inflammatory agents, developing biologics targeting key immune mediators, and lifestyle interventions known to impact immune health. This section highlights current and experimental approaches to restore immune balance in stress-related psychiatric disorders.
5.1. Anti-Inflammatory Pharmacological Agents
Several conventional anti-inflammatory drugs have been evaluated for their antidepressant and anxiolytic properties, particularly in individuals with elevated inflammatory markers. Minocycline, a tetracycline antibiotic with anti-inflammatory and neuroprotective properties, has also shown promise. A 12-week RCT of minocycline augmentation in MDD found significant improvement in depressive symptoms, particularly in patients with high inflammatory profiles [
100]. Although limited data exist in PTSD populations, a small RCT of the COX-2 inhibitor rofecoxib in PTSD showed improved symptom scores, and several preclinical studies support the efficacy of cytokine-modulating strategies in stress-exposed rodents [
101].
5.1.1. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
NSAIDs such as celecoxib, a COX-2 inhibitor, have shown promise as adjunctive treatments in major depressive disorder (MDD), particularly in patients with high baseline levels of CRP or IL-6 [
89,
92]. Although less explored in PTSD, some preliminary studies suggest that COX-2 inhibitors may reduce re-experiencing symptoms and irritability by dampening systemic inflammation.
5.1.2. Cytokine Antagonists
Recognition of immune dysregulation—particularly involving pro-inflammatory cytokines—as a key mechanism in PTSD and MDD has fueled growing interest in anti-inflammatory therapies as adjunctive treatments. We hypothesize that pro-inflammatory cytokine dysregulation contributes to a distinct immune-biological subtype of PTSD and MDD that is associated with treatment resistance and can be effectively targeted through immunomodulatory interventions, including anti-cytokine agents, repurposed anti-inflammatory drugs, and behavioral interventions that reduce systemic inflammation. Traditional antidepressants, including selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs), are only partially effective for many individuals, particularly those with elevated peripheral inflammatory markers. Meta-analyses suggest that inflammation contributes to treatment resistance, underscoring the rationale for targeting immune pathways in specific subgroups.
Monoclonal antibodies targeting pro-inflammatory cytokines have shown mixed results in the treatment of PTSD or MDD. The TNF-α blocker infliximab demonstrated antidepressant effects in a subset of MDD patients with elevated CRP (>5 mg/L), but not in the broader population [
81]. Similarly, IL-6 receptor antagonists (e.g, tocilizumab) are under investigation for mood and cognitive symptoms associated with chronic inflammation and autoimmune disease, with emerging relevance to PTSD. Unfortunately, it seems that the IL-6 receptor antagonist tocilizumab does not improve and may actually worsen depression and related symptoms—including anxiety, pain, and sleep—among medically ill individuals undergoing allogeneic cell transplantation [
102]. The immunosuppressive nature of these biologics raises concerns regarding infection risk, cost, and long-term safety, limiting their widespread use in psychiatric populations without co-occurring inflammatory disease. However, the evidence for tocilizumab directly affecting PTSD symptoms is limited. More research is needed to determine if tocilizumab or other anti-inflammatory treatments could be beneficial in managing PTSD.
5.2. Glucocorticoid and HPA Axis Modulation
Given the interaction between immune dysregulation and the HPA axis, pharmacologic agents that restore glucocorticoid sensitivity have been explored. Agents such as mifepristone (a glucocorticoid receptor antagonist) have demonstrated symptom reduction in subsets of patients with psychotic depression and trauma-related disorders, possibly via normalization of feedback inhibition and immune modulation. It is being investigated as a potential treatment for PTSD, particularly in individuals who haven’t responded well to standard therapies like SSRIs or psychotherapy [
103].
Hydrocortisone administration immediately following trauma exposure has also been investigated as a preventive measure against PTSD, with some evidence suggesting reduced inflammation and symptom severity when administered early [
104]. Recently, it has been reported that hydrocortisone promotes an accelerated degradation of sensory-perceptual representations underlying traumatic intrusive memories in PTSD treatment [
105].
5.3. Immunomodulatory Properties of Psychotropics
Several conventional psychotropic medications exert immunomodulatory effects independent of their neurotransmitter actions. For example:
-
-
Selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine and sertraline reduce peripheral levels of IL-1β and TNF-α, which may contribute to their efficacy in both MDD and PTSD [106,107]. Several clinical trials have evaluated anti-cytokine therapies in mood disorders. Notably, a randomized controlled trial (RCT) of the TNF-α antagonist infliximab in patients with treatment-resistant depression (TRD) found that although infliximab was not effective overall. However, infliximab was not effective overall, it significantly improved depressive symptoms in patients with elevated baseline C-reactive protein (CRP ≥ 5 mg/L) [29]. Similarly, the COX-2 inhibitor celecoxib has demonstrated antidepressant efficacy in combination with SSRIs, particularly in patients with major depression and elevated inflammatory markers [87,89]. A meta-analysis of 10 RCTs found that celecoxib augmentation significantly reduced depressive symptoms compared to placebo [92]. Ketamine, an NMDA receptor antagonist with rapid antidepressant effects, has been shown to reduce IL-6 and TNF-α levels post-administration in treatment-resistant depression, and may influence microglial activation states [108].
-
-
Atypical antipsychotics (e.g, quetiapine, risperidone) can reduce CRP and other pro-inflammatory cytokines and have been used off-label in PTSD, particularly for managing hyperarousal and psychotic symptoms [109].
The immune-modulating properties of these agents may partly explain differential treatment responses among individuals with varying levels of inflammation.
5.4. Lifestyle Interventions Targeting Inflammation
In addition to pharmacological interventions, non-pharmacological lifestyle modifications known to reduce systemic inflammation—such as aerobic exercise, mindfulness-based stress reduction (MBSR), and anti-inflammatory diets—are increasingly being integrated into treatment plans. Exercise has been shown to reduce IL-6 and TNF-α levels and improve depressive symptoms [
110]. Similarly, dietary interventions such as the Mediterranean diet have been associated with lower systemic inflammation and lower depression risk [
111].
5.4.1. Physical Activity
Regular aerobic exercise has well-documented anti-inflammatory effects, including reduced IL-6 and TNF-α levels and improved immune cell function. Exercise also enhances hippocampal neurogenesis and is associated with symptom improvement in PTSD [
112] and MDD [
113,
114].
5.4.2. Dietary Interventions
Anti-inflammatory diets rich in omega-3 fatty acids, antioxidants, and polyphenols (e.g, Mediterranean diet) are associated with lower rates of depression and anxiety. Omega-3 supplementation, particularly eicosapentaenoic acid (EPA), has demonstrated mood-stabilizing effects, possibly suppressing IL-1β and TNF-α [
115,
116].
5.4.3. Mind-Body Practices
Mindfulness-based stress reduction (MBSR), yoga, and meditation have been shown to decrease pro-inflammatory cytokines and normalize immune cell function in individuals with PTSD and MDD. These practices may work by downregulating SNS and HPA axis activity and promoting parasympathetic tone [
117,
118].
5.5. Emerging and Experimental Approaches
5.5.1. Chemokine Receptor Antagonists
Novel agents targeting chemokine receptors (e.g, CCR2, CXCR3) are under investigation for their neuroimmune regulatory roles. Preclinical studies suggest blocking CCL2-CCR2 signaling may reduce microglial activation and behavioral symptoms in stress-exposed rodents [
119]. While human studies remain limited, this represents a promising area of therapeutic development.
5.5.2. Microbiome-Based Interventions
The gut microbiota significantly influences systemic inflammation and neuroimmune signaling. Dysbiosis has been linked to both increased gut permeability and elevated cytokine production. Probiotics, prebiotics, and dietary fiber can promote a favorable microbial environment, potentially reducing IL-6 and TNF-α levels and improving psychiatric symptoms [
120,
121].
5.5.3. Neuromodulation Techniques
Transcranial magnetic stimulation (TMS) and vagus nerve stimulation (VNS) have demonstrated anti-inflammatory effects via central modulation of autonomic and immune networks. VNS, in particular, enhances cholinergic anti-inflammatory pathways and may lower peripheral TNF-α and IL-1β, showing promise in treatment-resistant depression and PTSD [
122,
123,
124].
As the field moves toward precision psychiatry, peripheral inflammatory markers such as IL-6, TNF-α, and CRP are increasingly evaluated for treatment stratification. These markers may help identify inflammation-related subtypes of depression or PTSD that respond preferentially to immunomodulatory strategies [
125]. Despite growing interest, challenges remain. Anti-inflammatory agents may have limited efficacy in unselected populations, and long-term safety—especially in psychiatric use—requires further study. Future trials should incorporate biomarker-guided stratification, focus on reproducible inflammatory subtypes, and include PTSD cohorts to better characterize therapeutic targets in trauma-related disorders.
6. Future Directions and Conclusions
Despite considerable progress, research gaps remain in understanding the role of cytokines and chemokines in PTSD and MDD. Longitudinal and mechanistic studies are needed to clarify whether immune dysregulation precedes, coincides with, or follows the onset of these disorders. Research using both in vitro and in vivo models is essential to identify specific immune mechanisms underlying psychopathology. A major challenge ahead is establishing standardized protocols for biomarker sampling, assay techniques, and statistical adjustments for confounding factors such as medication use, circadian rhythms, BMI, and smoking, which are necessary to improve reproducibility and comparability across studies. Additionally, immune signatures may vary among individuals; therefore, identifying stable inflammatory biotypes that span PTSD and MDD could promote the development of personalized, immune-targeted treatments. Integration of cytokine and chemokine profiles with machine learning algorithms and digital health technologies may provide new avenues for dynamic, individualized treatment strategies. Translational research that stratifies participants by immune status could facilitate testing immunomodulatory therapies. Combining biological and psychological treatments may offer greater benefits for both patients and clinicians. Ultimately, precision psychiatry frameworks that incorporate endocrine and immune profiles could optimize early interventions and improve the prediction of clinical outcomes. In conclusion, targeting the immune system in stress-related psychiatric disorders holds great promise. Cytokines and chemokines, long studied as downstream correlates of stress and trauma, are now emerging as active contributors to disease mechanisms and clinical trajectories. By advancing biomarker-guided treatment and personalized medicine, the immune-based approach may pave the way for more effective, tailored interventions for individuals suffering from PTSD and MDD.
Author Contributions
Conceptualization, X.-Z.H. & L.Z.; Formal Analysis, X.-Z.H. & L.Z.; Resources, X.-Z.H. & L.Z.; Writing—Original Draft Preparation, L.Z.; Writing—Review & Editing, X.-Z.H. & L.Z.; Visualization, X.-Z.H. & L.Z.
Ethics Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable.
Funding
This research received no external funding.
Declaration of Competing Interest
No conflict of interests has been declared.
Disclaimer Statement
The opinions and assertions expressed herein are those of the authors and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences or the Department of Defense and Henry M. Jackson Foundation for the Advancement of Military Medicine.
References
-
1.
Gratacos J, Collado A, Filella X, Sanmarti R, Canete J, Llena J, et al. Serum cytokines (IL-6, TNF-alpha, IL-1 beta and IFN-gamma) in ankylosing spondylitis: a close correlation between serum IL-6 and disease activity and severity.
Br. J. Rheumatol. 1994,
33, 927–931. doi:10.1093/rheumatology/33.10.927.
[Google Scholar]
-
2.
Bonne O, Gill JM, Luckenbaugh DA, Collins C, Owens MJ, Alesci S, et al. Corticotropin-releasing factor, interleukin-6, brain-derived neurotrophic factor, insulin-like growth factor-1, and substance P in the cerebrospinal fluid of civilians with post-traumatic stress disorder before and after treatment with paroxetine.
J. Clin. Psychiatry 2011,
72, 1124–1128. doi:10.4088/JCP.09m05106blu.
[Google Scholar]
-
3.
Yirmiya R. Endotoxin produces a depressive-like episode in rats.
Brain Res. 1996,
711, 163–174. doi:10.1016/0006-8993(95)01415-2.
[Google Scholar]
-
4.
Dantzer R, O'Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain.
Nat. Rev. Neurosci. 2008,
9, 46–56. doi:10.1038/nrn2297.
[Google Scholar]
-
5.
Dantzer R, Wollman EE, Vitkovic L, Yirmiya R. Cytokines, stress, and depression. Conclusions and perspectives.
Adv Exp Med. Biol. 1999,
461, 317–329. doi:10.1007/978-0-585-37970-8_17.
[Google Scholar]
-
6.
Von Känel R, Hepp U, Kraemer B, Traber R, Keel M, Mica L, et al. Evidence for low-grade systemic pro-inflammatory activity in patients with post-traumatic stress disorder.
J. Psychiatr. Res. 2007,
41, 744–752. doi:10.1016/j.jpsychires.2006.06.009.
[Google Scholar]
-
7.
Gill JM, Saligan L, Woods S, Page G. PTSD is associated with an excess of inflammatory immune activities.
Perspect Psychiatr. Care 2009,
45, 262–277. doi:10.1111/j.1744-6163.2009.00229.x.
[Google Scholar]
-
8.
Spivak B, Shohat B, Mester R, Avraham S, Gil-Ad I, Bleich A, et al. Elevated levels of serum interleukin-1 beta in combat-related post-traumatic stress disorder.
Biol. Psychiatry 1997,
42, 345–348. doi:10.1016/s0006-3223(96)00375-7.
[Google Scholar]
-
9.
Nkiliza A, Joshi U, Evans JE, Ait-Ghezala G, Parks M, Crawford F, et al. Adaptive Immune Responses Associated with the Central Nervous System Pathology of Gulf War Illness.
Neurosci. Insights 2021,
16, 26331055211018458. doi:10.1177/26331055211018458.
[Google Scholar]
-
10.
Passos IC, Vasconcelos-Moreno MP, Costa LG, Kunz M, Brietzke E, Quevedo J, et al. Inflammatory markers in post-traumatic stress disorder: a systematic review, meta-analysis, and meta-regression.
Lancet Psychiatry 2015,
2, 1002–1012. doi:10.1016/S2215-0366(15)00309-0.
[Google Scholar]
-
11.
Lindqvist D, Wolkowitz OM, Mellon S, Yehuda R, Flory JD, Henn-Haase C, et al. Pro-inflammatory milieu in combat-related PTSD is independent of depression and early life stress.
Brain Behav. Immun. 2014,
42, 81–88. doi:10.1016/j.bbi.2014.06.003.
[Google Scholar]
-
12.
Maes M, Lin AH, Delmeire L, Van Gastel A, Kenis G, De Jongh R, et al. Elevated serum interleukin-6 (IL-6) and IL-6 receptor concentrations in post-traumatic stress disorder following accidental man-made traumatic events.
Biol. Psychiatry 1999,
45, 833–839. doi:10.1016/s0006-3223(98)00131-0.
[Google Scholar]
-
13.
Pace TW, Heim CM. A short review on the psychoneuroimmunology of post-traumatic stress disorder: from risk factors to medical comorbidities.
Brain Behav. Immun. 2011,
25, 6–13. doi:10.1016/j.bbi.2010.10.003.
[Google Scholar]
-
14.
Deslauriers J, Powell S, Risbrough VB. Immune signaling mechanisms of PTSD risk and symptom development: insights from animal models.
Curr. Opin. Behav. Sci. 2017,
14, 123–132. doi:10.1016/j.cobeha.2017.01.005.
[Google Scholar]
-
15.
Michopoulos V, Powers A, Gillespie CF, Ressler KJ, Jovanovic T. Inflammation in Fear- and Anxiety-Based Disorders: PTSD, GAD, and Beyond.
Neuropsychopharmacology 2017,
42, 254–270. doi:10.1038/npp.2016.146.
[Google Scholar]
-
16.
Brenhouse HC, Danese A, Grassi-Oliveira R. Neuroimmune Impacts of Early-Life Stress on Development and Psychopathology.
Curr. Top Behav. Neurosci. 2019,
43, 423–447. doi:10.1007/7854_2018_53.
[Google Scholar]
-
17.
Haroon E, Miller AH, Sanacora G. Inflammation, Glutamate, and Glia: A Trio of Trouble in Mood Disorders.
Neuropsychopharmacology 2017,
42, 193–215. doi:10.1038/npp.2016.199.
[Google Scholar]
-
18.
Kruse M, Steudte-Schmiedgen S, Wessa M. From inflammation to PTSD: a review of biomarkders and pathways.
Curr. Opin. Psychol. 2021,
41, 72–78.
[Google Scholar]
-
19.
Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression.
Biol. Psychiatry 2009,
65, 732–741. doi:10.1016/j.biopsych.2008.11.029.
[Google Scholar]
-
20.
Zhang L, Hu XZ, Li X, Chen Z, Benedek DM, Fullerton CS, et al. Potential chemokine biomarkers associated with PTSD onset, risk and resilience as well as stress responses in US military service members.
Transl. Psychiatry 2020,
10, 31. doi:10.1038/s41398-020-0693-1.
[Google Scholar]
-
21.
Yehuda R, Flory JD, Pratchett LC, Buxbaum J, Ising M, Holsboer F. Putative biological mechanisms for the association between early life adversity and the subsequent development of PTSD.
Psychopharmacology 2010,
212, 405–417. doi:10.1007/s00213-010-1969-6.
[Google Scholar]
-
22.
Gola H, Engler H, Sommershof A, Adenauer H, Kolassa S, Schedlowski M, et al. Post-traumatic stress disorder is associated with an enhanced spontaneous production of pro-inflammatory cytokines by peripheral blood mononuclear cells.
BMC Psychiatry 2013,
13, 40. doi:10.1186/1471-244X-13-40.
[Google Scholar]
-
23.
Martinac M, Pehar D, Karlović D, Babić D, Marčinko D, Jakovljević M. Metabolic syndrome, activity of the hypothalamic-pituitary-adrenal axis and inflammatory mediators in depressive disorder.
Acta Clin. Croat. 2014,
53, 55–71.
[Google Scholar]
-
24.
Reichenberg A, Yirmiya R, Schuld A, Kraus T, Haack M, Morag A, et al. Cytokine-associated emotional and cognitive disturbances in humans.
Arch. Gen. Psychiatry 2001,
58, 445–452. doi:10.1001/archpsyc.58.5.445.
[Google Scholar]
-
25.
Felger JC, Haroon E, Patel TA, Goldsmith DR, Wommack EC, Woolwine BJ, et al. What does plasma CRP tell us about peripheral and central inflammation in depression?
Mol. Psychiatry 2020,
25, 1301–1311. doi:10.1038/s41380-018-0096-3.
[Google Scholar]
-
26.
Hodes GE, Kana V, Menard C, Merad M, Russo SJ. Neuroimmune mechanisms of depression.
Nat. Neurosci. 2015,
18, 1386–1393. doi:10.1038/nn.4113.
[Google Scholar]
-
27.
Kiecolt-Glaser JK, Derry HM, Fagundes CP. Inflammation: depression fans the flames and feasts on the heat.
Am J Psychiatry 2015,
172, 1075–1091. doi:10.1176/appi.ajp.2015.15020152.
[Google Scholar]
-
28.
Rosenblat JD, Cha DS, Mansur RB, McIntyre RS. Inflamed moods: a review of the interactions between inflammation and mood disorders.
Prog. Neuropsychopharmacol. Biol. Psychiatry 2014,
53, 23–34. doi:10.1016/j.pnpbp.2014.01.013.
[Google Scholar]
-
29.
Raison CL, Rutherford RE, Woolwine BJ, Shuo C, Schettler P, Drake DF, et al. A randomized controlled trial of the tumor necrosis factor antagonist infliximab for treatment-resistant depression: the role of baseline inflammatory biomarkers.
JAMA Psychiatry 2013,
70, 31–41. doi:10.1001/2013.jamapsychiatry.4.
[Google Scholar]
-
30.
Tyring S, Gottlieb A, Papp K, Gordon K, Leonardi C, Wang A, et al. Etanercept and clinical outcomes, fatigue, and depression in psoriasis: double-blind placebo-controlled randomised phase III trial.
Lancet 2006,
367, 29–35. doi:10.1016/S0140-6736(05)67763-X.
[Google Scholar]
-
31.
Gupta MA, Jarosz P, Gupta AK. Post-traumatic stress disorder (PTSD) and the dermatology patient.
Clin. Dermatol. 2017,
35, 260–266. doi:10.1016/j.clindermatol.2017.01.005.
[Google Scholar]
-
32.
Schmidt FM, Schröder T, Kirkby KC, Sander C, Suslow T, Holdt LM, et al. Pro- and anti-inflammatory cytokines, but not CRP, are inversely correlated with severity and symptoms of major depression.
Psychiatry Res. 2016,
239, 85–91. doi:10.1016/j.psychres.2016.02.052.
[Google Scholar]
-
33.
Savitz J, Drevets WC. Bipolar and major depressive disorder: neuroimaging the developmental-degenerative divide.
Neurosci. Biobehav. Rev. 2009,
33, 699–771. doi:10.1016/j.neubiorev.2009.01.004.
[Google Scholar]
-
34.
Yirmiya R, Goshen I. Immune modulation of learning, memory, neural plasticity and neurogenesis.
Brain Behav. Immun. 2011,
25, 181–213. doi:10.1016/j.bbi.2010.10.015.
[Google Scholar]
-
35.
Haapakoski R, Mathieu J, Ebmeier KP, Alenius H, Kivimäki M. Cumulative meta-analysis of interleukins 6 and 1β, tumour necrosis factor α and C-reactive protein in patients with major depressive disorder.
Brain Behav. Immun. 2015,
49, 206–215. doi:10.1016/j.bbi.2015.06.001.
[Google Scholar]
-
36.
Working Group I Contribution to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. In Climate Change 2013—The Physical Science Basis; Cambridge University Press: Cambridge, UK, 2014; 1–30.
-
37.
Colasanto M, Madigan S, Korczak D. Depression and inflamation among children and adolescents: A meta-analysis.
J. Affect. Disord. 2020,
277, 940–948. doi:10.1016/j.jad.2020.09.025.
[Google Scholar]
-
38.
Moriarity DP, van Borkulo C, Alloy L. B. Inflammatory phenotype of depression symptom structure: A network perspective.
Brain Behav. Immun. 2021,
93, 35–42. doi:10.1016/j.bbi.2020.12.005.
[Google Scholar]
-
39.
Osimo EF, Pillinger T, Rodriguez IM, Khandaker GM, Pariante CM, Howes OD. Inflammatory markers in depression: A meta-analysis of mean differences and variability in 5,166 patients and 5,083 controls.
Brain Behav. Immun. 2020,
87, 901–909. doi:10.1016/j.bbi.2020.02.010.
[Google Scholar]
-
40.
Breen MS, Tylee DS, Maihofer AX, Neylan TC, Mehta D, Binder EB, et al. PTSD Blood Transcriptome Mega-Analysis: Shared Inflammatory Pathways across Biological Sex and Modes of Trauma.
Neuropsychopharmacology 2018,
43, 469–481. doi:10.1038/npp.2017.220.
[Google Scholar]
-
41.
Krabbe KS, Reichenberg A, Yirmiya R, Smed A, Pedersen BK, Bruunsgaard H. Low-dose endotoxemia and human neuropsychological functions.
Brain Behav. Immun. 2005,
19, 453–460. doi:10.1016/j.bbi.2005.04.010.
[Google Scholar]
-
42.
Miller AH, Raison CL. The role of inflammation in depression: from evolutionary imperative to modern treatment target.
Nat. Rev. Immunol. 2016,
16, 22–34. doi:10.1038/nri.2015.5.
[Google Scholar]
-
43.
Felger JC, Lotrich FE. Inflammatory cytokines in depression: neurobiological mechanisms and therapeutic implications.
Neuroscience 2013,
246, 199–229. doi:10.1016/j.neuroscience.2013.04.060.
[Google Scholar]
-
44.
Cohen H, Zohar J, Gidron Y, Matar MA, Belkind D, Loewenthal U, et al. Blunted HPA axis response to stress influences susceptibility to post-traumatic stress response in rats.
Biol. Psychiatry 2006,
59, 1208–1218. doi:10.1016/j.biopsych.2005.12.003.
[Google Scholar]
-
45.
Sher L. Post-traumatic stress disorder and suicidal behavior.
Exper. Rev. Neurother. 2020,
20, 559–568.
[Google Scholar]
-
46.
Spivak B, Radwan M, Mester R, Ovadia H, Moisa R, Weizman A. Reduced platelet responsiveness to serotonin in post-traumatic stress disorder.
Psychiatry Res. 2000,
94, 1–6.
[Google Scholar]
-
47.
Zhang W, Xiao D, Mao Q, Xia H. Role of neuroinflammation in neurodegeneration development.
Signal Trans. Target. Ther. 2023,
8, 267. doi:10.1038/s41392-023-01486-5.
[Google Scholar]
-
48.
Barrett E, Ross RP, O'Toole PW, Fitzgerald GF, Stanton C. gamma-Aminobutyric acid production by culturable bacteria from the human intestine.
J. Appl. Microbiol. 2012,
113, 411–417. doi:10.1111/j.1365-2672.2012.05344.x.
[Google Scholar]
-
49.
Cheung SG, Goldenthal AR, Uhlemann AC, Mann JJ, Miller JM, Sublette ME. Systematic Review of Gut Microbiota and Major Depression.
Front. Psychiatry 2019,
10, 34. doi:10.3389/fpsyt.2019.00034.
[Google Scholar]
-
50.
Sanders ME, Merenstein DJ, Reid G, Gibson GR, Rastall RA. Probiotics and prebiotics in intestinal health and disease: from biology to the clinic.
Nat. Rev. Gastroenterol. Hepatol. 2019,
16, 605–616. doi:10.1038/s41575-019-0173-3.
[Google Scholar]
-
51.
Muzio L, Viotti A, Martino G. Microglia in Neuroinflammation and Neurodegeneration: From Understanding to Therapy.
Front. Neurosci. 2021,
15, 742065. doi:10.3389/fnins.2021.742065.
[Google Scholar]
-
52.
Woodburn SC, Bollinger JL, Wohleb ES. The semantics of microglia activation: neuroinflammation, homeostasis, and stress.
J. Neuroinflamm. 2021,
18, 258. doi:10.1186/s12974-021-02309-6.
[Google Scholar]
-
53.
Enomoto S, Kato TA. Stress Mediated Microglial Hyper-Activation and Psychiatric Diseases.
Brain Nerve 2021,
73, 795–802 (). doi:10.11477/mf.1416201837.
[Google Scholar]
-
54.
Bollinger JL, Dadosky DT, Flurer JK, Rainer IL, Woodburn SC, Wohleb ES. Microglial P2Y12 mediates chronic stress-induced synapse loss in the prefrontal cortex and associated behavioral consequences.
Neuropsychopharmacology 2023,
48, 1347–1357. doi:10.1038/s41386-022-01519-7.
[Google Scholar]
-
55.
Li B, Yang W, Ge T, Wang Y, Cui R. Stress induced microglial activation contributes to depression.
Pharmacol. Res. 2022,
179, 106145. doi:10.1016/j.phrs.2022.106145.
[Google Scholar]
-
56.
Comai S, Bertazzo A, Brughera M, Crotti S. Advances in Clinical Chemistry; Makowski GS, Ed.; Elsevier: Amsterdam, The Netherlands, 2020; Volume 95, pp. 165–218.
-
57.
Salminen A. Role of indoleamine 2,3-dioxygenase 1 (IDO1) and kynurenine pathway in the regulation of the aging process.
Ageing Res. Rev. 2022,
75, 101573. doi:10.1016/j.arr.2022.101573.
[Google Scholar]
-
58.
Carpenedo R, Pittaluga A, Cozzi A, Attucci S, Galli A, Raiteri M, et al. Presynaptic kynurenate-sensitive receptors inhibit glutamate release.
Eur. J. Neurosci. 2001,
13, 2141–2147. doi:10.1046/j.0953-816x.2001.01592.x.
[Google Scholar]
-
59.
Dunn AJ. Techniques in the Behavioral and Neural Sciences; Steckler T, Kalin NH, Reul JMHM, Eds.; Elsevier: Amsterdam, The Netherlands, 2005; Volume 15, pp. 157–174.
-
60.
Mahmood Z, Davidsson A, Olsson E, Leanderson P, Lundberg AK, Jonasson L. The effect of acute exercise on interleukin-6 and hypothalamic–pituitary–adrenal axis responses in patients with coronary artery disease.
Sci. Rep. 2020,
10, 21390. doi:10.1038/s41598-020-78286-2.
[Google Scholar]
-
61.
Judd AM, Call GB, Barney M, McILMOIL CJ, Balls AG, Adams A, et al. Possible function of IL-6 and TNF as intraadrenal factors in the regulation of adrenal steroid secretion.
Ann. N. Y. Acad. Sci. 2000,
917, 628–637. doi:10.1111/j.1749-6632.2000.tb05428.x.
[Google Scholar]
-
62.
Karin O, Raz M, Tendler A, Bar A, Korem Kohanim Y, Milo T, et al. A new model for the HPA axis explains dysregulation of stress hormones on the timescale of weeks.
Mol. Syst. Biol. 2020,
16, e9510. doi:10.15252/msb.20209510.
[Google Scholar]
-
63.
Pariante CM, Lightman SL. The HPA axis in major depression: classical theories and new developments.
Trends Neurosci. 2008,
31, 464–468. doi:10.1016/j.tins.2008.06.006.
[Google Scholar]
-
64.
Castro-Vale I, Carvalho D. The Pathways between Cortisol-Related Regulation Genes and PTSD Psychotherapy.
Healthcare 2020,
8, 376. doi:10.3390/healthcare8040376.
[Google Scholar]
-
65.
Bethin KE, Vogt SK, Muglia LJ. Interleukin-6 is an essential, corticotropin-releasing hormone-independent stimulator of the adrenal axis during immune system activation.
Proc. Natl. Acad. Sci. USA 2000,
97, 9317–9322. doi:10.1073/pnas.97.16.9317.
[Google Scholar]
-
66.
Besedovsky HO, Del Rey A, Klusman I, Furukawa H, Arditi GM, Kabiersch A. Cytokines as modulators of the hypothalamus-pituitary-adrenal axis.
J. Steroid Biochem. Mol. Biol. 1991,
40, 613–618. doi:10.1016/0960-0760(91)90284-c.
[Google Scholar]
-
67.
Chen L, Qin Q, Huang P, Cao F, Yin M, Xie Y, et al. Chronic pain accelerates cognitive impairment by reducing hippocampal neurogenesis may via CCL2/CCR2 signaling in APP/PS1 mice.
Brain Res. Bulletin 2023,
205, 110801. doi:10.1016/j.brainresbull.2023.110801.
[Google Scholar]
-
68.
Yan Y, Su J, Zhang Z. The CXCL12/CXCR4/ACKR3 Response Axis in Chronic Neurodegenerative Disorders of the Central Nervous System: Therapeutic Target and Biomarker.
Cell. Mol. Neurobiol. 2022,
42, 2147–2156. doi:10.1007/s10571-021-01115-1.
[Google Scholar]
-
69.
Bruenig D, Mehta D, Morris CP, Harvey W, Lawford B, Young RM, et al. Genetic and serum biomarker evidence for a relationship between TNFα and PTSD in Vietnam war combat veterans.
Compr. Psychiatry 2017,
74, 125–133. doi:10.1016/j.comppsych.2017.01.015.
[Google Scholar]
-
70.
Friend SF, Nachnani R, Powell SB, Risbrough VB. C-Reactive Protein: Marker of risk for post-traumatic stress disorder and its potential for a mechanistic role in trauma response and recovery.
Eur. J. Neurosc. 2022,
55, 2297–2310. doi:10.1111/ejn.15031.
[Google Scholar]
-
71.
Kim TD, Lee S, Yoon S. Inflammation in Post-Traumatic Stress Disorder (PTSD): A Review of Potential Correlates of PTSD with a Neurological Perspective.
Antioxidants 2020,
9, 107. doi:10.3390/antiox9020107.
[Google Scholar]
-
72.
Teche SP, Rovaris DL, Aguiar BW, Hauck S, Vitola ES, Bau CH, et al. Resilience to traumatic events related to urban violence and increased IL10 serum levels.
Psychiatry Res. 2017,
250, 136–140. doi:10.1016/j.psychres.2017.01.072.
[Google Scholar]
-
73.
Paganin W, Signorini S. Inflammatory biomarkers in depression: scoping review.
BJPsych. Open 2024,
10, e165. doi:10.1192/bjo.2024.787.
[Google Scholar]
-
74.
Rocha NP, Scalzo PL, Barbosa IG, Souza MS, Morato IB, Vieira ÉL, et al. Cognitive Status Correlates with CXCL10/IP-10 Levels in Parkinson’s Disease.
Parkinson's Dis. 2014,
2014, 903796. doi:10.1155/2014/903796.
[Google Scholar]
-
75.
Teixeira AL, Gama CS, Rocha NP, Teixeira MM. Revisiting the Role of Eotaxin-1/CCL11 in Psychiatric Disorders.
Front. Psychiatry 2018,
9, 241. doi:10.3389/fpsyt.2018.00241.
[Google Scholar]
-
76.
Peruzzolo TL, Pinto JV, Roza TH, Shintani AO, Anzolin AP, Gnielka V, et al. Inflammatory and oxidative stress markers in post-traumatic stress disorder: a systematic review and meta-analysis.
Mol. Psychiatry 2022,
27, 3150–3163. doi:10.1038/s41380-022-01564-0.
[Google Scholar]
-
77.
Solmi M, Sharma MS, Osimo EF, Fornaro M, Bortolato B, Croatto G, et al. Peripheral levels of C-reactive protein, tumor necrosis factor-α, interleukin-6, and interleukin-1β across the mood spectrum in bipolar disorder: A meta-analysis of mean differences and variability.
Brain, Behav. Immun. 2021,
97, 193–203. doi:10.1016/j.bbi.2021.07.014.
[Google Scholar]
-
78.
Katrinli S, Oliveira NCS, Felger JC, Michopoulos V, Smith AK. The role of the immune system in posttraumatic stress disorder.
Tranlational Psychiatry 2022,
12, 313.
[Google Scholar]
-
79.
Benedetti F, Poletti S, Vai B, Mazza MG, Lorenzi C, Brioschi S, et al. Higher baseline interleukin-1β and TNF-α hamper antidepressant response in major depressive disorder.
Eur. Neuropsychopharmacol 2021,
42, 35–44. doi:10.1016/j.euroneuro.2020.11.009.
[Google Scholar]
-
80.
Fitton R, Sweetman J, Heseltine-Carp W, van der Feltz-Cornelis C. Anti-inflammatory medications for the treatment of mental disorders: A scoping review.
Brain Behav. Immun. Health 2022,
26, 100518. doi:10.1016/j.bbih.2022.100518.
[Google Scholar]
-
81.
Rizk MM, Bolton L, Cathomas F, He H, Russo SJ, Guttman-Yassky E, et al. Immune-Targeted Therapies for Depression: Current Evidence for Antidepressant Effects of Monoclonal Antibodies.
J. Clin. Psychiatry 2024,
85, 23nr15243. doi:10.4088/JCP.23nr15243.
[Google Scholar]
-
82.
Gong H, Su WJ, Deng SL, Luo J, Du ZL, Luo Y, et al. Anti-inflammatory interventions for the treatment and prevention of depression among older adults: a systematic review and meta-analysis.
Transl. Psychiatry 2025,
15, 114. doi:10.1038/s41398-025-03317-3.
[Google Scholar]
-
83.
Saban KL, Collins EG, Mathews HL, Bryant FB, Tell D, Gonzalez B, et al. Impact of a Mindfulness-Based Stress Reduction Program on Psychological Well-Being, Cortisol, and Inflammation in Women Veterans.
J. General Int. Med. 2022,
37, 751–761. doi:10.1007/s11606-022-07584-4.
[Google Scholar]
-
84.
Almeida TM, da Silva UR, Pires JP, Borges IN, Martins CR, Cordeiro Q, et al. Effectiveness of Ketamine for the Treatment of Post-Traumatic Stress Disorder - A Systematic Review and Meta-Analysis.
Clin. Neuropsychiatry 2024,
21, 22–31. doi:10.36131/cnfioritieditore20240102.
[Google Scholar]
-
85.
Wang W, Wang R, Xu J, Qin X, Jiang H, Khalid A, et al. Minocycline Attenuates Stress-Induced Behavioral Changes via Its Anti-inflammatory Effects in an Animal Model of Post-traumatic Stress Disorder.
Front. Psychiatry 2018,
9, 558. doi:10.3389/fpsyt.2018.00558.
[Google Scholar]
-
86.
Lee TD, Lee JY, Hong DY, Lee EC, Park SW, Lee MR, et al. Neuroinflammation in Post-Traumatic Stress Disorder.
Biomedicines 2022,
10, 953. doi:10.3390/biomedicines10050953.
[Google Scholar]
-
87.
Abbasi S-H, Hosseini F, Modabbernia A, Ashrafi M, Akhondzadeh S. Effect of celecoxib add-on treatment on symptoms and serum IL-6 concentrations in patients with major depressive disorder: Randomized double-blind placebo-controlled study.
J. Affect. Disord. 2012,
141, 308–314. doi:10.1016/j.jad.2012.03.033.
[Google Scholar]
-
88.
Kohler O, Krogh J, Mors O, Benros ME. Inflammation in Depression and the Potential for Anti-Inflammatory Treatment.
Curr. Neuropharmacol. 2016,
14, 732–742. doi:10.2174/1570159x14666151208113700.
[Google Scholar]
-
89.
Müller N, Schwarz MJ, Dehning S, Douhe A, Cerovecki A, Goldstein-Müller B, et al. The cyclooxygenase-2 inhibitor celecoxib has therapeutic effects in major depression: results of a double-blind, randomized, placebo controlled, add-on pilot study to reboxetine.
Mol. Psychiatry 2006,
11, 680–684. doi:10.1038/sj.mp.4001805.
[Google Scholar]
-
90.
Du Y, Dou Y, Qang M, Wang Y, Fan H, Fan N, et al. Efficacy and acceptability of anti-infelammatory agents in major depressive disorder: a systematc review and meta-analysis.
Front. Psychiatry 2024,
15. doi:10.3389/fpsyt.2024.1407529.
[Google Scholar]
-
91.
Akhondzadeh S, Jafari S, Raisi F, Nasehi AA, Ghoreishi A, Salehi B, et al. Clinical trial of adjunctive celecoxib treatment in patients with major depression: a double blind and placebo controlled trial.
Depress. Anxiety 2009,
26, 607–611. doi:10.1002/da.20589.
[Google Scholar]
-
92.
Köhler O, Benros ME, Nordentoft M, Farkouh ME, Iyengar RL, Mors O, et al. Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials.
JAMA Psychiatry 2014,
71, 1381–1391. doi:10.1001/jamapsychiatry.2014.1611.
[Google Scholar]
-
93.
Bai S, Guo W, Feng Y, Deng H, Li G, Nie H, et al. Efficacy and safety of anti-inflammatory agents for the treatment of major depressive disorder: A systematic review and meta-analysis of randomised controlled trials.
J. Neurol. Neurosurg. Psychiatry 2020,
91, 21–32. doi:10.1136/jnnp-2019-320912.
[Google Scholar]
-
94.
Chen B, Sun X, Huang H, Feng C, Chen W, Wu D. An integrated machine learning framework for developing and validating a diagnostic model of major depressive disorder based on interstitial cystitis-related genes.
J. Affect. Disord. 2024,
359, 22–32. doi:10.1016/j.jad.2024.05.061.
[Google Scholar]
-
95.
McQuaid RJ. Transdiagnostic biomarker approaches to mental health disorders: Consideration of symptom complexity, comorbidity and context.
Brain Behav. Immun. Health 2021,
16, 100303. doi:10.1016/j.bbih.2021.100303.
[Google Scholar]
-
96.
Papini S, Iturralde E, Lu Y, Greene JD, Barreda F, Sterling SA, et al. Development and validation of a machine learning model using electronic health records to predict trauma- and stressor-related psychiatric disorders after hospitalization with sepsis.
Transl. Psychiatry 2023,
13, 400. doi:10.1038/s41398-023-02699-6.
[Google Scholar]
-
97.
Ma H, Xu J, Li R, McIntyre RS, Teopiz KM, Cao B, et al. The Impact of Cognitive Behavioral Therapy on Peripheral Interleukin-6 Levels in Depression: A Systematic Review and Meta-Analysis.
Front. Psychiatry 2022,
13, 844176. doi:10.3389/fpsyt.2022.844176.
[Google Scholar]
-
98.
Kraus C, Kadriu B, Lanzenberger R, Zarate CA Jr, Kasper S. Prognosis and improved outcomes in major depression: a review.
Transl. Psychiatry 2019,
9, 127. doi:10.1038/s41398-019-0460-3.
[Google Scholar]
-
99.
Strawbridge R, et al. Inflammation and clinical response to treatment in depression: A meta-analysis.
Eur. Neuropsychopharmacol 2015,
25, 1532–1543. doi:10.1016/j.euroneuro.2015.06.007.
[Google Scholar]
-
100.
Dean OM, Maes M, Ashton M, Berk L, Kanchanatawan B, Sughondhabirom A, et al. Protocol and rationale-the efficacy of minocycline as an adjunctive treatment for major depressive disorder: a double blind, randomised, placebo controlled trial.
Clin. Psychopharmacol. Neurosci. 2014,
12, 180–188. doi:10.9758/cpn.2014.12.3.180.
[Google Scholar]
-
101.
Wang M, Duan F, Wu J, Min Q, Huang Q, Luo M, et al. Effect of cyclooxygenase‑2 inhibition on the development of post‑traumatic stress disorder in rats.
Mol. Med. Rep. 2018,
17, 4925–4932. doi:10.3892/mmr.2018.8525.
[Google Scholar]
-
102.
Knight JM, Costanzo ES, Singh S, Yin Z, Szabo A, Pawar DS, et al. The IL-6 antagonist tocilizumab is associated with worse depression and related symptoms in the medically ill.
Transl. Psychiatry 2021,
11, 58. doi:10.1038/s41398-020-01164-y.
[Google Scholar]
-
103.
Howland RH. Mifepristone as a Therapeutic Agent in Psychiatry.
J. Psychosoc. Nurs. Mental Health Serv. 2013,
51, 11–14. doi:10.3928/02793695-20130513-01.
[Google Scholar]
-
104.
Kothgassner OD, Pellegrini M, Goreis A, Giordano V, Edobor J, Fischer S, et al. Hydrocortisone administration for reducing post-traumatic stress symptoms: A systematic review and meta-analysis.
Psychoneuroendocrinology 2021,
126, 105168. doi:10.1016/j.psyneuen.2021.105168.
[Google Scholar]
-
105.
Hennessy VE, Troebinger L, Iskandar G, Das RK, Kamboj SK. Accelerated forgetting of a trauma-like event in healthy men and women after a single dose of hydrocortisone.
Transl. Psychiatry 2022,
12, 354. doi:10.1038/s41398-022-02126-2.
[Google Scholar]
-
106.
Wang L, Wang R, Liu L, Qiao D, Baldwin DS, Hou R. Effects of SSRIs on peripheral inflammatory markers in patients with major depressive disorder: A systematic review and meta-analysis.
Brain Behav. Immun. 2019,
79, 24–38. doi:10.1016/j.bbi.2019.02.021.
[Google Scholar]
-
107.
Hannestad J, DellaGioia N, Bloch M. The effect of antidepressant medication treatment on serum levels of inflammatory cytokines: a meta-analysis.
Neuropsychopharmacology 2011,
36, 2452–2459. doi:10.1038/npp.2011.132.
[Google Scholar]
-
108.
Jóźwiak-Bębenista M, Sokołowska P, Wiktorowska-Owczarek A, Kowalczyk E, Sienkiewicz M. Ketamine - A New Antidepressant Drug with Anti-Inflammatory Properties.
J. Pharmacol. Exp. Ther. 2024,
388, 134–144. doi:10.1124/jpet.123.001823.
[Google Scholar]
-
109.
Alvarez-Herrera S, Escamilla R, Medina-Contreras O, Saracco R, Flores Y, Hurtado-Alvarado G, et al. Immunoendocrine Peripheral Effects Induced by Atypical Antipsychotics.
Front. Endocrinol. (Lausanne) 2020,
11, 195. doi:10.3389/fendo.2020.00195.
[Google Scholar]
-
110.
Eyre HA, Papps E, Baune BT. Treating depression and depression-like behavior with physical activity: an immune perspective.
Front. Psychiatry 2013,
4, 3. doi:10.3389/fpsyt.2013.00003.
[Google Scholar]
-
111.
Jacka FN, O’Neil A, Opie R, Itsiopoulos C, Cotton S, Mohebbi M, et al. A randomised controlled trial of dietary improvement for adults with major depression (the 'SMILES' trial).
BMC Med. 2017,
15, 23. doi:10.1186/s12916-017-0791-y.
[Google Scholar]
-
112.
Noushad S, Ansari B, Ahmed S. Effect of nature-based physical activity on post-traumatic growth among healthcare providers with post-traumatic stress.
Stress Health 2022,
38, 813–826. doi:10.1002/smi.3135.
[Google Scholar]
-
113.
Mafla-España MA, Cauli O. Non-Pharmacological Interventions for Managing the Symptoms of Depression in Women with Breast Cancer: A Literature Review of Clinical Trials.
Diseases 2025,
13, 80. doi:10.3390/diseases13030080.
[Google Scholar]
-
114.
Dudek KA, Paton SE, Binder LB, Collignon A, Dion-Albert L, Cadoret A, et al. Astrocytic cannabinoid receptor 1 promotes resilience by dampening stress-induced blood-brain barrier alterations.
Nat. Neurosci. 2025,
28, 766–782. doi:10.1038/s41593-025-01891-9.
[Google Scholar]
-
115.
Trebaticka J, Durackova Z. Psychiatric disorders and omega-3 fatty acids.
Free Radic. Biol. Med. 2014,
75 Suppl 1, S52. doi:10.1016/j.freeradbiomed.2014.10.824.
[Google Scholar]
-
116.
Hankenson KD, Watkins BA, Schoenlein IA, Allen KG, Turek JJ. Omega-3 fatty acids enhance ligament fibroblast collagen formation in association with changes in interleukin-6 production.
Proc. Soc. Exp. Biol. Med. 2000,
223, 88–95. doi:10.1046/j.1525-1373.2000.22312.x.
[Google Scholar]
-
117.
Chiarpenello C, Brodmann K.
What can the psychoneuroimmunology of yoga teach us about depression's psychopathology? Brain Behav. Immun. -Health 2024,
42, 100877. doi:10.1016/j.bbih.2024.100877.
[Google Scholar]
-
118.
Wang X, Sundquist K, Palmér K, Hedelius A, Memon AA, Sundquist J. Macrophage Migration Inhibitory Factor and microRNA-451a in Response to Mindfulness-based Therapy or Treatment as Usual in Patients with Depression, Anxiety, or Stress and Adjustment Disorders.
Int. J. Neuropsychopharmacol. 2018,
21, 513–521. doi:10.1093/ijnp/pyy001.
[Google Scholar]
-
119.
Yao Y, Tsirka SE. The CCL2-CCR2 system affects the progression and clearance of intracerebral hemorrhage.
Glia 2012,
60, 908–918. doi:10.1002/glia.22323.
[Google Scholar]
-
120.
Shah BR, Li B, Al Sabbah H, Xu W, Mráz J. Effects of prebiotic dietary fibers and probiotics on human health: With special focus on recent advancement in their encapsulated formulations.
Trends Food Sci. Technol. 2020,
102, 178–192. doi:10.1016/j.tifs.2020.06.010.
[Google Scholar]
-
121.
Clapp M, Aurora N, Herrera L, Bhatia M, Wilen E, Wakefield S. Gut microbiota's effect on mental health: The gut-brain axis.
Clin. Pract. 2017,
7, 987. doi:10.4081/cp.2017.987.
[Google Scholar]
-
122.
Asadizeidabadi A, Hosseini S, Pyatkov A. Effects of Repetitive Transcranial Magnetic Stimulation on Tumor Necrosis Factor Alpha in Neuropsychological Disorders: A Systematic Review and Meta-Analysis.
Brain Behav. 2025,
15, e70329. doi:10.1002/brb3.70329.
[Google Scholar]
-
123.
Rajkumar RP. Immune-inflammatory markers of response to repetitive transcranial magnetic stimulation in depression: A scoping review.
Asian J. Psychiatr. 2024,
91, 103852. doi:10.1016/j.ajp.2023.103852.
[Google Scholar]
-
124.
Kavakbasi E, Van Assche E, Schwarte K, Hohoff C, Baune BT. Long-Term Immunomodulatory Impact of VNS on Peripheral Cytokine Profiles and Its Relationship with Clinical Response in Difficult-to-Treat Depression (DTD).
Int. J. Mol. Sci. 2024,
25, 4196. doi:10.3390/ijms25084196.
[Google Scholar]
-
125.
Khandaker GM, Oltean BP, Kaser M, Dibben CR, Ramana R, Jadon DR, et al. Protocol for the insight study: a randomised controlled trial of single-dose tocilizumab in patients with depression and low-grade inflammation.
BMJ Open 2018,
8, e025333. doi:10.1136/bmjopen-2018-025333.
[Google Scholar]