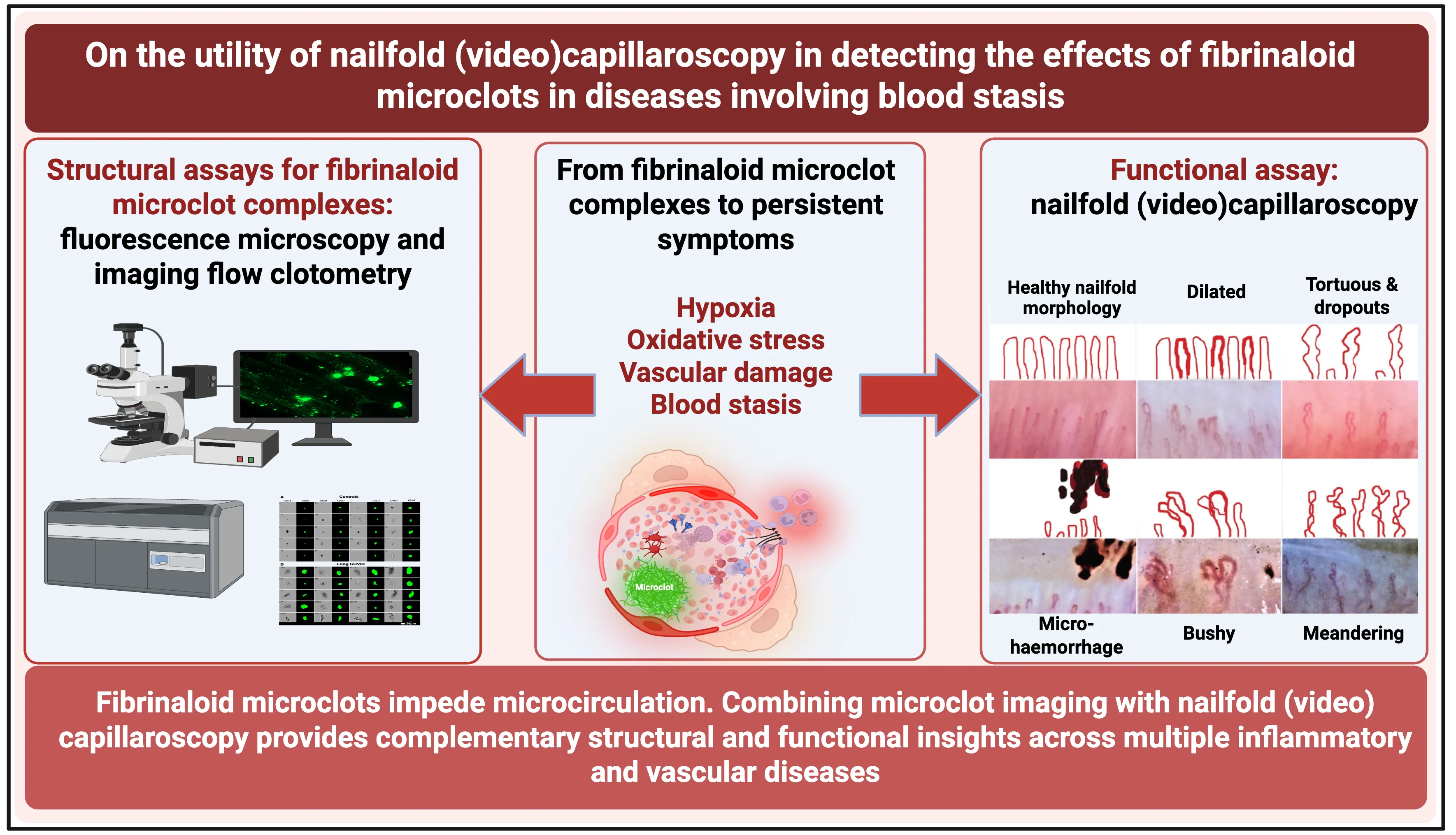
More than a decade ago it was discovered, via scanning electron microscopy, that blood can clot into a highly anomalous form, which in contrast to the normal thrombi with individual fibres that appear like nicely cooked spaghetti, adopted a morphology, referred to as ‘dense matted deposits’, that instead resembled parboiled spaghetti that had congealed into an amorphous mass (e.g., [
1,
2,
3]). It was subsequently recognised (e.g., [
4,
5,
6]) that the ‘anomalous form’ was amyloid in nature, as it could be stained with the well-established amyloid stain thioflavin T [
7,
8,
9,
10]. Such clots were commonly in the range 2–200 μm diameter, were found in a variety of chronic, inflammatory diseases [
11] (including Alzheimer’s [
12,
13,
14], Parkinson’s [
15,
16], type 2 diabetes [
12,
17,
18] and rheumatoid arthritis [
19]) and—as all amyloids—were significantly resistant to the normal routes of fibrinolysis via plasmin(ogen) [
20]. Because of their amyloid nature, we have come to refer to them as fibrinaloid microclots [
21,
22,
23,
24,
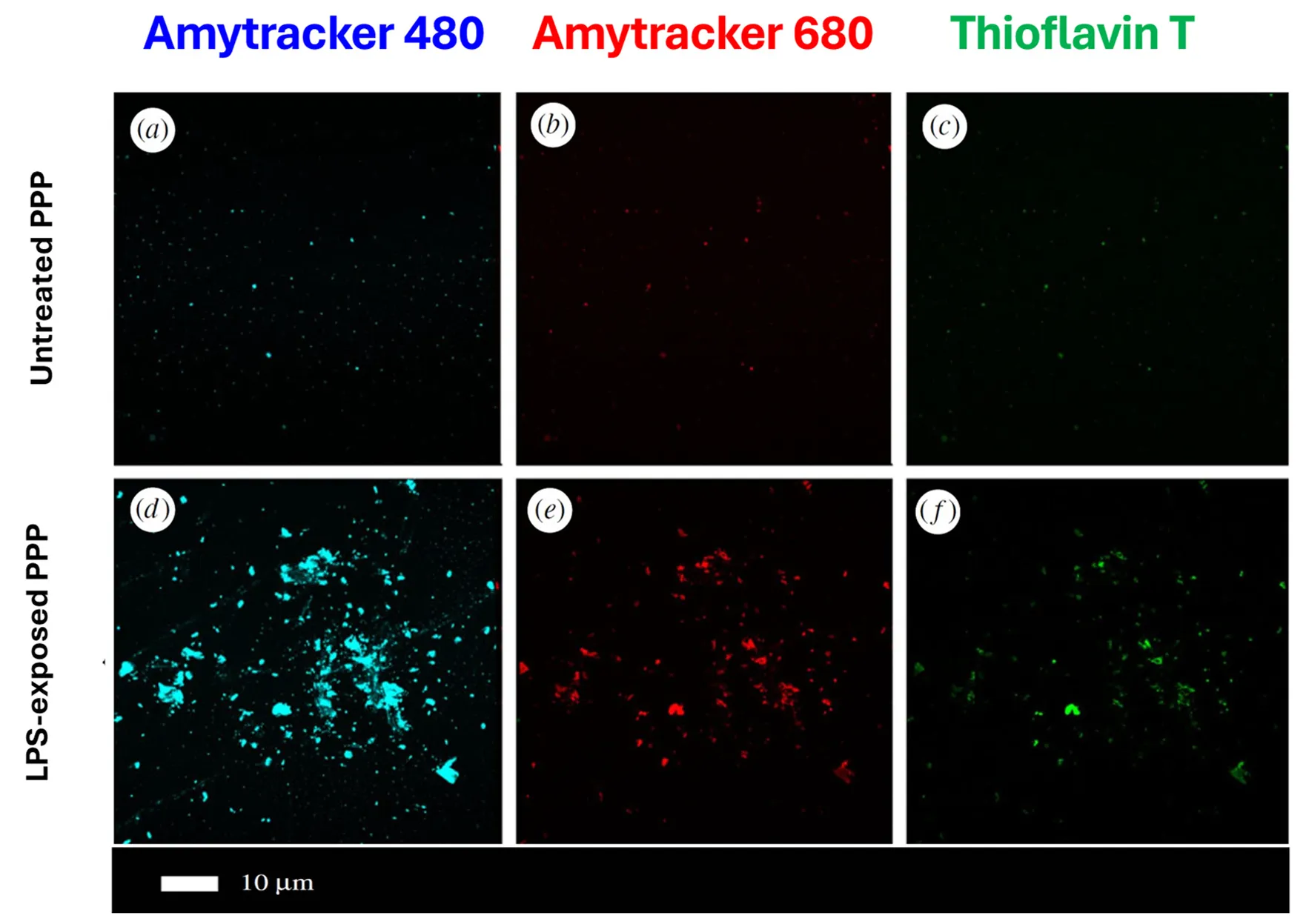
25]. shows a typical example of the microclots as stained with three different amyloid-selective stains.
. A typical example of fibrinaloid microclots. Platelet-poor plasma was treated with thrombin and stained either with one of two oligothiophene [<a href="#B26" class="html-bibr">26</a>,<a href="#B27" class="html-bibr">27</a>,<a href="#B28" class="html-bibr">28</a>] Amytracker™ dyes (<strong>a</strong>,<strong>b</strong>,<strong>d</strong>,<strong>e</strong>) or with thioflavin T (<strong>c</strong>,<strong>f</strong>) . In one case (<strong>d</strong>–<strong>f</strong>), a small amount of bacterial lipopolysaccharide was added prior to the thrombin. Modified from the CC-BY 4.0 publication [<a href="#B6" class="html-bibr">6</a>].
More recently, fibrinaloid microclots have been recognised as a major feature accompanying both acute [
18,
29] and Long COVID [
24,
30,
31,
32,
33,
34,
35,
36], as well as in the related Myalgic encephalopathy/chronic fatigue syndrome (ME/CFS) [
23,
34,
37] and sepsis [
38]. As with any inert matter of this type and size (including microplastics [
39,
40,
41]), fibrinaloid microclots can become trapped in microcapillaries, thereby restricting blood flow and oxygen transport to tissues. This provides ready explanations for a variety of phenomena, especially those associated with Long COVID, such as fatigue [
21], post-exertional symptom exacerbation [
42], postural orthostatic tachycardia syndrome (POTS) [
43], and fibromyalgia [
44].
Proteomic studies [
30,
38,
45] indicate [
46] a high prevalence of amyloidogenic proteins in fibrinaloid microclots that, in contrast to normal clots [
47], do
not reflect those in the typical normal plasma proteome [
46], and this has predictive power [
48,
49]. In addition, both the microclots [
50,
51,
52] and the thrombectomised macroclots observed [
53,
54] following an ischaemic stroke are amyloid in nature. Amyloidogenic cross-seeding can significantly change the conformation of other proteins, and this can also explain the generation of autoantibodies since such proteins would then be seen as not-self [
22].
A chief consequence of the blockage of microcapillaries by fibrinaloid microclots is a slowing down of the blood flow, sometimes referred to (including by Virchow in his ‘triad’ [
55,
56,
57]) as Blood Stasis. ‘Blood stasis’ is also a highly important concept in Traditional Asian Medicines (see e.g., [
58,
59,
60,
61]), and seems strongly correlated with the presence of fibrinaloid microclots [
62]. Ischaemia or hypoxia are inevitable consequences, and indeed this property, leading to oxidative stress, is consequently common to all the chronic, inflammatory syndromes being considered here (e.g., [
11,
63,
64,
65,
66,
67,
68,
69,
70,
71,
72,
73]).
To date, the most frequent types of measurements of fibrinaloid microclots have mainly been ‘structural’ using thioflavin T staining and observation by fluorescence microscopy (e.g., [
4,
6,
12,
31,
33,
38,
74]) or flow cytometry [
32] (‘flow clotometry’ [
34]). A more ‘functional’ assay would be highly desirable to complement this. Although many of the phenomena may occur deep inside the body, our chief focus here is on the human skin microcirculation [
75] and its attendant disorders (e.g., [
76,
77,
78,
79]).
Capillaroscopy refers to a general technique that can potentially determine blood flow rates in the microcirculation in a simple and non-invasive manner, and, given the above, might potentially serve as an excellent functional assay for blood stasis and microclot presence. Sublingual microscopy [
80], retinal [
81], and nailfold capillaroscopy (NFC) are in common use and—while other methods such as laser speckle contrast imaging [
82,
83,
84,
85,
86,
87,
88] and thermography [
89,
90] may also be used—we focus here on NFC. To this end, the chief purpose of the present review is to develop the idea that NFC, including in particular its derivative nailfold videocapillaroscopy (NVC), will be of value in understanding syndromes in which fibrinaloid microclots are involved, and to provide the evidence-based reasoning for this. A preprint has been lodged [
91].
2.1. History and Modern Implementations
Capillaroscopy is a technique for looking at the microcirculation [
75]. The idea that the study of capillaries might have disease-diagnostic value goes back to the 17th Century, when Johan Christophorous Kolhaus used a primitive microscope to observe the small blood vessels surrounding the nails, and later Giovanni Rasori, using a magnifying glass, related the observed properties to conjunctival inflammation [
92]. A list of recent reviews is given in .
Modern microscopes, commonly using 200× magnification, coupled to well engineered illumination and focusing optics, are all that is necessary to acquire static (capillaroscopy) and dynamic (videocapillaroscopy) images, with a second element being how these images are interpreted—manually or computationally—to provide useful diagnostic information (). Because our focus lies on the relationship with fibrinaloid microclots, we do not provide detailed analyses of the precise procedures involved (e.g., [
93,
94,
95]). Many commercial systems are available, although we neither seek to discriminate among them nor recommend particular models. They provide interfaces with laptops and even cellphones. Since interpretation by the human eye alone is neither straightforward nor objective [
96,
97], the more refined instrumentation usually comes with software to assist or even provide interpretation. It typically costs a few hundred pounds for entry-level models. Parameters (strictly, variables) that are measured or calculated include capillary density [
98,
99] and percentage of abnormal and giant capillaries, tortuosities, and haemorrhages [
94,
97,
100,
101,
102,
103]. EULAR (The European League Against Rheumatism) has agreed on a consented standardised capillaroscopic description protocol [
93,
104,
105,
106,
107].
. Cartoon illustrating the basic steps in nailfold capillaroscopy. Image includes elements of the Open Access (CC-BY 4.0) materials at [
94,
100,
108]. The three fingers adjacent to the thumb may be profiled, with 4 regions on each [
100]. The normal or healthy pattern (as illustrated) displays a regular architecture with uniform distribution and diameter and a hairpin shape [
109].
also illustrates the kinds of capillary structure seen in healthy controls (and see e.g., [
75,
94,
110]).
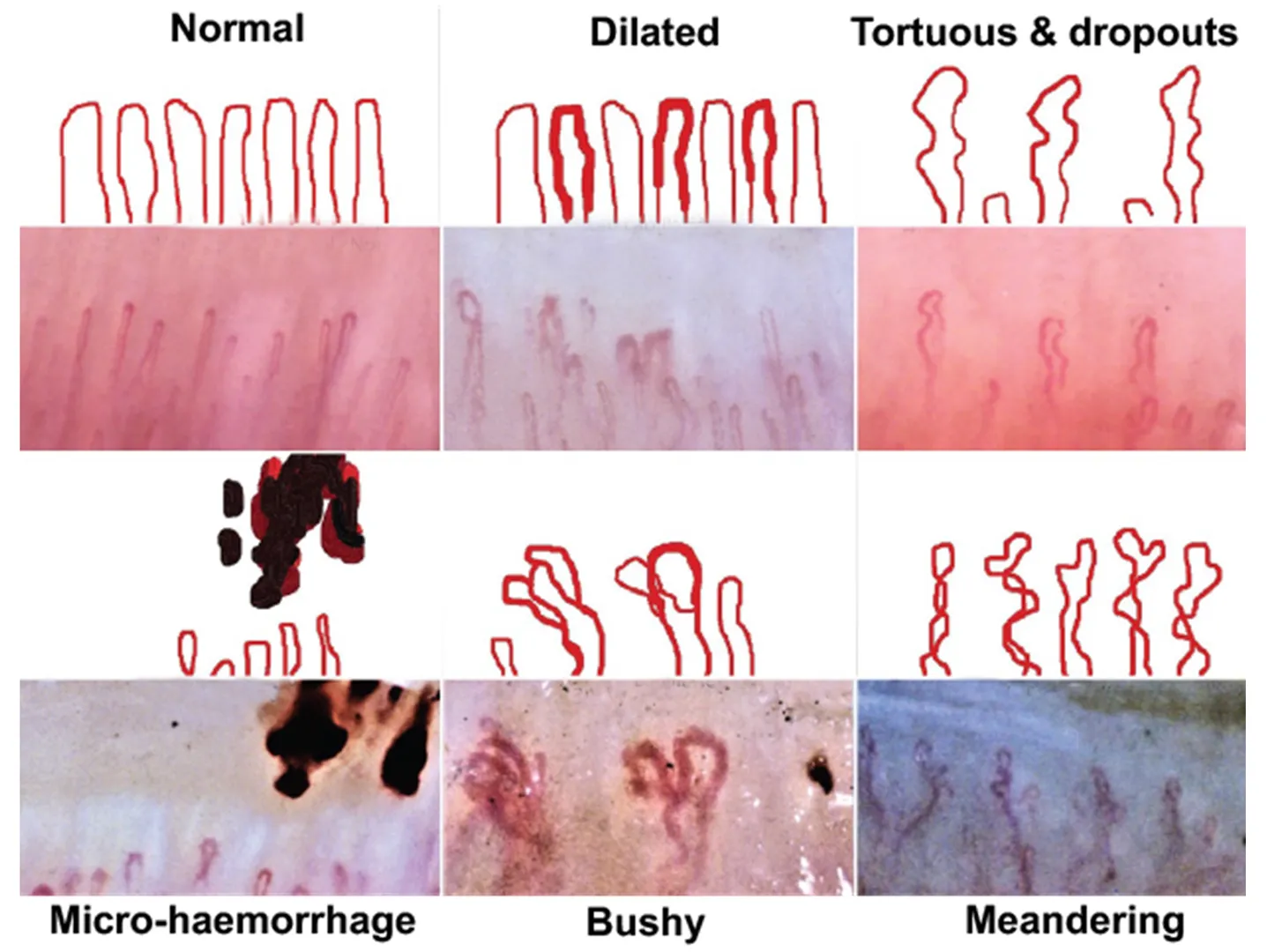
provides a feel for the kinds of images that are obtainable under different conditions.
. Some images and explanatory cartoons of various nailfold capillary morphologies. Taken from the CC-BY 4.0 Open Access paper [
94].
Clearly, the strategy is generic, and while possibly the majority of studies have focused on Raynaud’s disease, rheumatology, and systemic sclerosis (scleroderma), the range is very wide. This is partly because many are chronic inflammatory diseases with common vascular causes and/or symptoms [
11], including endothelial dysfunction. Systemic sclerosis is recognised as a vascular disease involving endothelial dysfunction [
111,
112,
113,
114,
115,
116,
117], thus bearing significant similarities to COVID-19 [
118] that most certainly does [
36,
119,
120,
121,
122,
123,
124,
125], so it is not surprising that such commonalities exist. In a sense, this survey thus adds weight to the view that there are common co-occurrences of various symptoms. The advantage of nailfold capillaroscopy over, e.g., cytokine-based assessment of inflammation is that capillaroscopy is non-invasive, quick, and cheap, providing useful information for diagnosis and treatment. To illustrate its broad general utility, a sample of such studies in which it has been used is included in . While these are seen mostly as immunological in character, we recognise that the symptoms of many other syndromes can be reflected in the microcirculation. Specifically, has three purposes. These are to show readers (i) that every disease where microclots have been measured shows abnormalities in the microcirculation as judged by NFC/NVC, (ii) for the microclot community to see how widespread and valuable the usage of NFC/NVC is and thus to encourage them to try it, and (iii) to point the NFC/NVC community at other diseases where (based on microclot measurements) we suggest their methods would be of value.
.
Some disorders involving the microcirculation in which (mainly) nailfold (video) capillaroscopy has been found to have diagnostic utility or where fibrinaloid microclots have been demonstrated. Disorders in which fibrinaloid microclots have been demonstrated are rendered in bold face; note that every disorder in which microclots have been demonstrated has anomalies as assessed using nailfold capillaroscopy.
| Disease or Syndrome |
Comments |
Selected Nailfold Capillaroscopy References |
Selected Fibrinaloid Microclot References
(Where Tested) |
| Acute COVID-19 |
Capillary tortuosity, meandering, haemosiderin deposition, and microhaemorrhage increased; capillary density and length, and blood flow decreased |
[126,127,128,129,130,131,132,133,134,135,136,137,138] |
[18,29,139,140,141,142] |
| Alzheimer’s dementia |
Greater nailfold capillary tortuosity in individuals with Alzheimer’s dementia |
[143,144] |
[12,13,14,145,146] |
| Anderson-Fabry disease |
Also known as Fabry disease. Promising but underexplored. Subclasses detected depend on the α-galactosidase A variant. |
[147,148,149,150] |
|
| Anorexia nervosa |
Related to connective tissue disorders |
[151,152] |
|
| Antineutrophil Cytoplasmic Antibody-Associated (ANCA) Vasculitis |
Neoangiogenesis, capillary
loss, microhaemorrhages, and bushy and enlarged capillaries
|
[153,154,155,156] |
|
| Atopic dermatitis |
Many more lesions, e.g., pitting, capillary density, tortuosity |
[157] |
|
| Behçet’s disease |
Increases in capillary dilatation, tortuous and branched capillaries, and microhaemorrhages |
[158,159] |
|
| Biliary cirrhosis |
Multiple abnormalities |
[160] |
|
| Cancer |
Not yet widely deployed, but some suggestive data imply it could have diagnostic or prognostic value. |
[161] |
|
| Chronic obstructive pulmonary disorder (COPD) |
Review |
[162] (but cf. [163]) |
|
| Chronic smokers |
Abnormalities are more common in chronic smokers |
[164] |
|
| Chronic urticaria |
Lower capillary density, more capillary malformations, and more irregular capillary dilations |
[165] |
|
| Connective tissue disorders |
Various |
[166,167,168] |
|
| Coronary heart disease |
Assessment of capillary blood flow and relation to erythrocyte aggregation |
[169] |
|
| Dermatomyositis |
Diminished capillary density and abnormal capillary morphology (including enlargement) in patients. It can be related to antibody levels. Haemosiderin deposits can occur. |
[104,170,171,172,173,174,175,176,177,178,179] |
|
| Diabetes mellitus, type 1 |
General |
[180,181] |
|
|
Use of deep learning |
[182] |
|
Diabetes mellitus,
type 2
|
Capillary dilatation, avascular zones, and tortuous capillaries |
[183,184,185] |
[12,17,18,186,187] |
|
Peak capillary blood flow velocity (CBFV) post-occlusion is much lower |
[188] |
|
|
Use of deep learning |
[182] |
|
|
Changes closely related to the quality of glucose control |
[189,190] |
|
|
Capillaries are larger but less dense |
[191] |
|
|
Various differences |
[192,193] |
|
| Diabetic complications |
Listed separately below |
|
|
| Diabetic foot |
Significant difference in pulp of the big toe |
[194] |
|
| Diabetic nephropathy |
Significant correlation between lowered glomerular filtration rate and e.g., reduced fundus transparency and visibility of the sub-venous plexus |
[195,196] |
|
| Diabetic neuropathy |
Improved by α-lipoic acid |
[197] |
|
| Diabetic retinopathy |
Decreased capillary length, width, number, and turbidity, crossing capillaries, and other abnormalities |
[183,184,198,199,200,201] |
|
| Digital ulcers |
A common accompaniment to systemic sclerosis and Raynaud’s disease |
[202,203,204] |
|
| Endothelial dysfunction |
Reviews |
[117,128] |
[125] |
|
In livedoid vasculopathy |
[205] |
|
|
Association with rheumatoid arthritis |
[206] |
|
| Fibromyalgia |
Raynaud’s disease and impaired microvascular function are common in patients with fibromyalgia, where nailfold abnormalities are common. |
[207,208,209,210] |
|
|
Fewer capillaries, apical limb width, and capillary width decreased |
[78,211] |
See [44], and for amyloid deposition in skeletal muscle [212] |
|
Mean capillary loop diameter, micro-aneurysm number, avascular areas, and neoangiogenic
capillaries significantly higher
|
[213] |
|
| Gaucher disease |
Various subtypes. Microangiopathy is the most obvious NFC finding |
[214] |
|
| General reviews |
|
[77,94,100,215,216,217] |
|
|
Non-rheumatic diseases |
[218] |
|
|
Vascular disease |
[219] |
|
| Glaucoma |
Huge decrease in capillary blood flow |
[220] |
|
| Heart failure |
Greater abnormalities with preserved ejection fraction |
[221] |
|
| Hepatitis, viral |
Changes in the avascular area, capillary dilatation, capillary tortuosity, and capillary enlargement were observed |
[222] |
|
| Hypertension (general) |
Many differences, including lowered capillary density and other morphological changes |
[223] |
|
| Idiopathic inflammatory myopathy |
Significant differences, including between subtypes |
[224,225,226,227,228] |
|
| Idiopathic macular telangiectasia type 2 |
Increased capillary tortuosity, ‘bizarre’ capillaries, and microhaemorrhage in the patient group compared to the controls |
[229] |
|
| Leprosy |
Capillary dropouts are the most frequent, followed by tortuous, receding, and dilated capillaries |
[230] |
|
| Long COVID |
Compares Long COVID patients without and with systemic sclerosis. Long COVID patients show more microvascular alterations than recovered COVID patients. |
[231] |
[21,24,30,31,32,33,34,35,43,45,125,232] |
| Lupus (systemic lupus erythematosus) |
|
[105,173,233,234,235,236] |
|
| Migraine |
Seemingly little studied recently by nailfold capillaroscopy, but major differences observed vs controls, especially when cold-induced |
[237,238] |
[239] |
| Neutropenia |
Indirect assessment from videocapillaroscopy |
[240,241] |
|
| Obstructive sleep apnoea |
All capillaroscopy findings were significantly higher in the patient group |
[242] |
|
| Parkinson’s disease |
Seemingly not yet studied by nailfold capillaroscopy in any detail. |
|
[12,16,243] |
| Polycythemia vera |
Increase in the diameter of vessels |
[244] |
|
| Polymyositis |
Scleroderma pattern predominated and improved after treatment. |
[104,170,179,245,246] |
|
| Pre-eclampsia |
Change in capillary length and density with pregnancy-induced hypertension, whether pre-eclamptic or not. Some relationship to maternal blood pressure [247]. |
[248] |
|
|
Decreased capillary density in pre-eclamptics |
[249] |
|
|
Review of capillaroscopy in pregnancy |
[250] |
|
| Psoriasis |
|
[251,252,253,254,255,256,257] |
|
Pulmonary
arterial hypertension
|
(Can accompany systemic sclerosis.) Lowered capillary density |
[223,258,259] |
|
| Raynaud’s disease or Raynaud’s phenomenon |
Common accompaniment of systemic sclerosis. NFC especially used in discriminating primary Raynaud’s from secondary Raynaud’s due to systemic sclerosis |
[89,204,260,261,262,263,264,265,266,267,268,269,270,271] |
|
|
Standardisation |
[106] |
|
| Rheumatology, especially rheumatoid arthritis |
Reviews |
[92,251,272,273,274,275,276,277,278,279,280] |
[19,281,282] |
| Sarcoidosis |
Early but promising |
[283,284,285] |
|
| Sarcopenia |
Common in rheumatoid arthritis and systemic sclerosis |
[286,287] |
|
| Sepsis and septic shock |
See Section 2.3 |
[288] |
[38] and see [289] |
|
Decreased capillary density sublingually |
[290] |
|
| Sickle cell disease |
Lower capillary density and more dilated capillaries |
[291] |
|
| Sjögren’s syndrome |
|
[292,293] |
|
| Systemic sclerosis |
It is increasingly seen as a vasculopathy [114]. Reviews on the role of NFC are in the adjacent column. Arguably, the commonest area of study. |
[107,172,294,295,296,297,298,299,300,301,302,303,304,305,306,307,308,309] |
|
|
Use of the NEMO score (the number of microhaemorrhages
plus micro-thromboses)
|
[310,311,312] |
|
|
Patients with primary biliary cholangitis |
[313] |
|
|
Differences when pulmonary arterial hypertension is also present |
[314,315] |
|
The widespread occurrence of alterations in the microcirculation, as judged by nailfold capillaroscopy, shows how extensive this is in multiple syndromes that plausibly share common causes. The important point here is that, where tested, all examples in which fibrinaloid microclots have been measured in plasma also show microcirculation disorders, as one would expect.
One reviewer questioned whether these techniques, that are well accepted for their ability to measure the morphological properties of microcapillaries, are also suitable for measuring blood
flow; clearly individual static images can not do that directly, although it is pretty obvious (given that these methods are routinely used for assessing the
microcirculation) that changes in capillary diameter and tortuosity necessarily have such effects [
107,
143,
144,
217,
273,
315,
316]. Equally clearly, video methods that image capillaries at intervals and with a suitable magnification can precisely detect the flow of blood, as the following illustrative references that demonstrate it explicitly amply show (e.g., [
100,
117,
143,
168,
188,
217,
317,
318,
319,
320,
321,
322,
323,
324,
325,
326]). This does not seem remotely controversial.
2.2. Long COVID as an Example
Following infection with the SARS-CoV-2 virus, a significant fraction of individuals fail to return fully to health, and after three months are said to suffer from post-acute sequelae of COVID-19 (PASC), commonly known as Long COVID [
327]. Long COVID is estimated to affect or have affected over 400 million individuals worldwide, contributing to an annual economic burden of $1 trillion or ~1% of the global economy [
328,
329]. Symptoms vary widely [
330,
331,
332,
333,
334,
335], with fatigue being the most common [
336,
337]. It is a disease in which many studies have shown the presence of fibrinaloid microclots [
21,
24,
30,
31,
32,
33,
34,
35,
43,
45,
125,
232], which provide ready explanations for the various symptoms [
21,
22,
42,
43]. Importantly, Cutolo and colleagues carried out a valuable study [
231] using NFC in patients with Long COVID and matched controls. Specifically, nailfold videocapillaroscopy (NVC) showed significant microvascular damage in long covid (LC) patients compared with matched healthy controls. Dilated capillaries, microhaemorrhages, abnormal shapes, and reduced capillary density were detectable in LC patients even 12 months after acute SARS-CoV-2 infection. Importantly, NVC demonstrated that these observables were normalised in patients who had recovered. It would seem that NVC is a valuable functional diagnostic for individuals with Long COVID, and a potentially valuable complement to the measurement of fibrinaloid microclots.
2.3. Sepsis and Septic Shock
Sepsis and septic shock are of special interest here for a number of reasons. First, they can be highly dangeous. Secondly, they are accompanied by microthrombi [
338] that we suggested are our fibrinaloid microclots [
289], and thirdly, the fibrinaloid microclot burden, as now so measured, is highly predictive of survival in the ICU (odds ratio > 5) [
38]. (The microclots are even more predictive of disseminated intravascular coagulation [
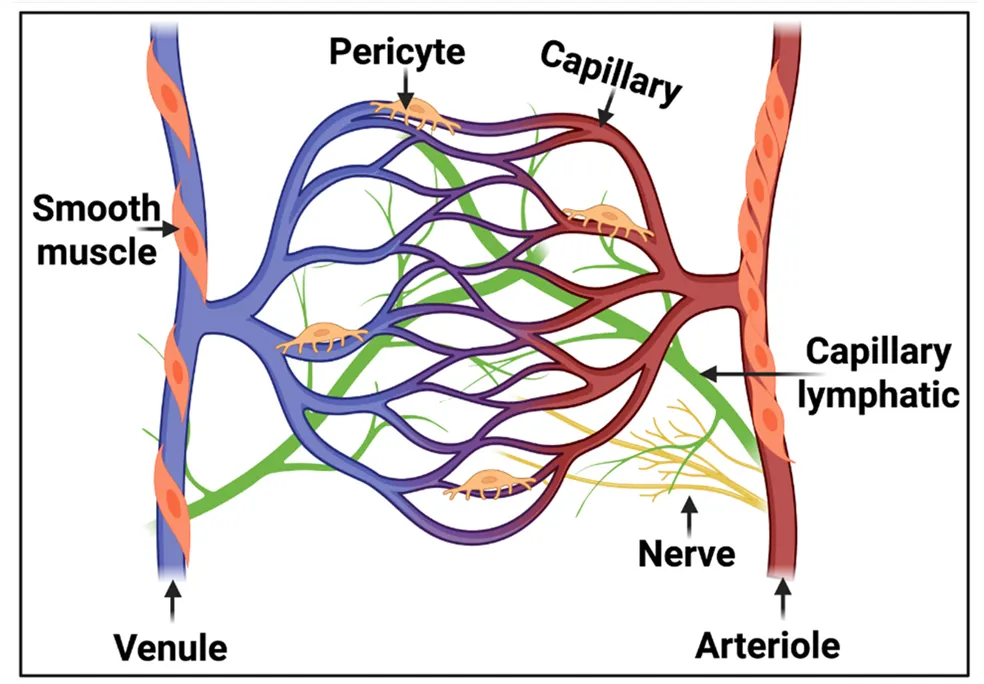
38].) Finally, the microcirculation () is intimately involved in sepsis and septic shock.
. The anatomy of the microcirculation is the largest part of the vascular system and consists of the smallest vessels, referred to as arterioles, capillaries, and venules. The lymphatic capillaries carry the extravascular fluid into the venous system, while the arterioles are surrounded by vascular smooth muscle cells responsible for regulating arteriole tone. Taken and slightly adapted from the CC-BY 4.0 publication [
339].
Specifically, disorders of the endothelium and microcirculation leading to hypoxia are recognised as an intimate part of sepsis and septic shock (e.g., [
288,
340,
341,
342,
343,
344,
345,
346,
347,
348,
349,
350,
351,
352,
353,
354,
355,
356,
357,
358,
359,
360,
361,
362,
363]). However, NFC is said to be not much used as the nailfold vascular bed is sensitive to peripheral vasoconstriction, vasopressor agents, and temperature changes. None of these seems like insurmountable issues [
364], and it would seem that the recognition of the importance of both the microcirculation and fibrinaloid microclots in sepsis mortality warrants a far more detailed analysis, to include a comparison between microclot burden, nailfold capillaroscopic findings, any effects of clotbusters or other treatments, and disease outcomes. Indeed, the generally less common sublingual capillaroscopy is known to be very useful [
365] and even predictive of mortality [
366].
2.4. ‘Blood Stasis’ and Treatments to Improve It
As mentioned above, ‘Blood stasis’, a term used as part of Virchow’s triad [
55,
56,
57,
367,
368], is an extremely important concept in Traditional Chinese Medicine [
58,
369,
370,
371,
372,
373,
374,
375] (known there as Xue Yu (血瘀) [
376]). Exactly equivalent ideas exist in Japanese Kampo medicine (where it is termed Oketsu [
377,
378,
379,
380]) and in Traditional Korean Medicine (where blood stasis is known as ‘Ouhyul’ or ‘Eohyul’) [
61,
381]). We recently summarised the extensive evidence to the effect that ‘blood stasis’ is precisely a manifestation of the presence and effects of fibrinaloid microclots [
62], in that all syndromes known to display fibrinaloid microclots are considered to be diseases of blood stasis. While such traditional medical formalisms also recognise that one should treat the patient as an individual, standard herbal formulas for diseases of blood stasis do exist, in the form of XueFu ZhuYu [
62,
382,
383,
384,
385,
386,
387] and Keishibukuryogan [
377,
388,
389], and are known to improve the microcirculation. Consequently, it would be of considerable interest to assess this via nailfold capillaroscopy.
2.5. Future Directions
Although many of the commercial systems are served by reasonably sophisticated software to assist interpretation [
390], much of the downstream analysis remains in the hands and minds of skilled clinicians, and, especially depending on the image quality [
391], is necessarily subjective [
323,
392,
393,
394]. This said, where it has been studied inter-rater reliability has been found to be good (e.g., [
92,
96,
392,
395,
396]). An easy prediction is that these kinds of tasks will soon be taken over by intelligent systems trained using modern data-driven generative methods of machine learning, commonly referred to as artificial intelligence or ‘AI’. This particular revolution is, of course, already underway [
390,
393,
394,
397,
398,
399,
400,
401,
402,
403,
404,
405]. To date, the lack of availability of labelled datasets has confined most efforts to transfer learning or ‘fine tuning’ of other models [
406]. However, much as with equivalent developments in general image processing [
407,
408], chemistry [
409], and protein science [
410,
411,
412], progress will be greatly assisted [
275] by the availability of a database of tagged images, videos and appropriate metadata taken directly from nailfold capillaroscopy, as well as the ability [
413] to explain the bases (in terms of features extracted) for any such disease classifications.
A further point is that while many diseases have been studied using nailfold capillaroscopy (), there are quite a number more, some with high prevalence, that have not. These would seem to offer considerable opportunities for devising analyses with prognostic value. For instance, myalgic encephalopathy/chronic fatigue syndrome (ME/CFS) shares many of the hallmarks of the other diseases (including Long COVID) listed in [
414,
415,
416], including endothelial dysfunction [
37,
417,
418,
419,
420], fibrinaloid microclots [
23,
37,
421], and a disrupted microcirculation [
422] (as in ), but we know of no attempt to assess its severity using nailfold capillaroscopy, which would provide further evidence beyond that existing (see [
232]) for a deranged microcirculation in this syndrome.
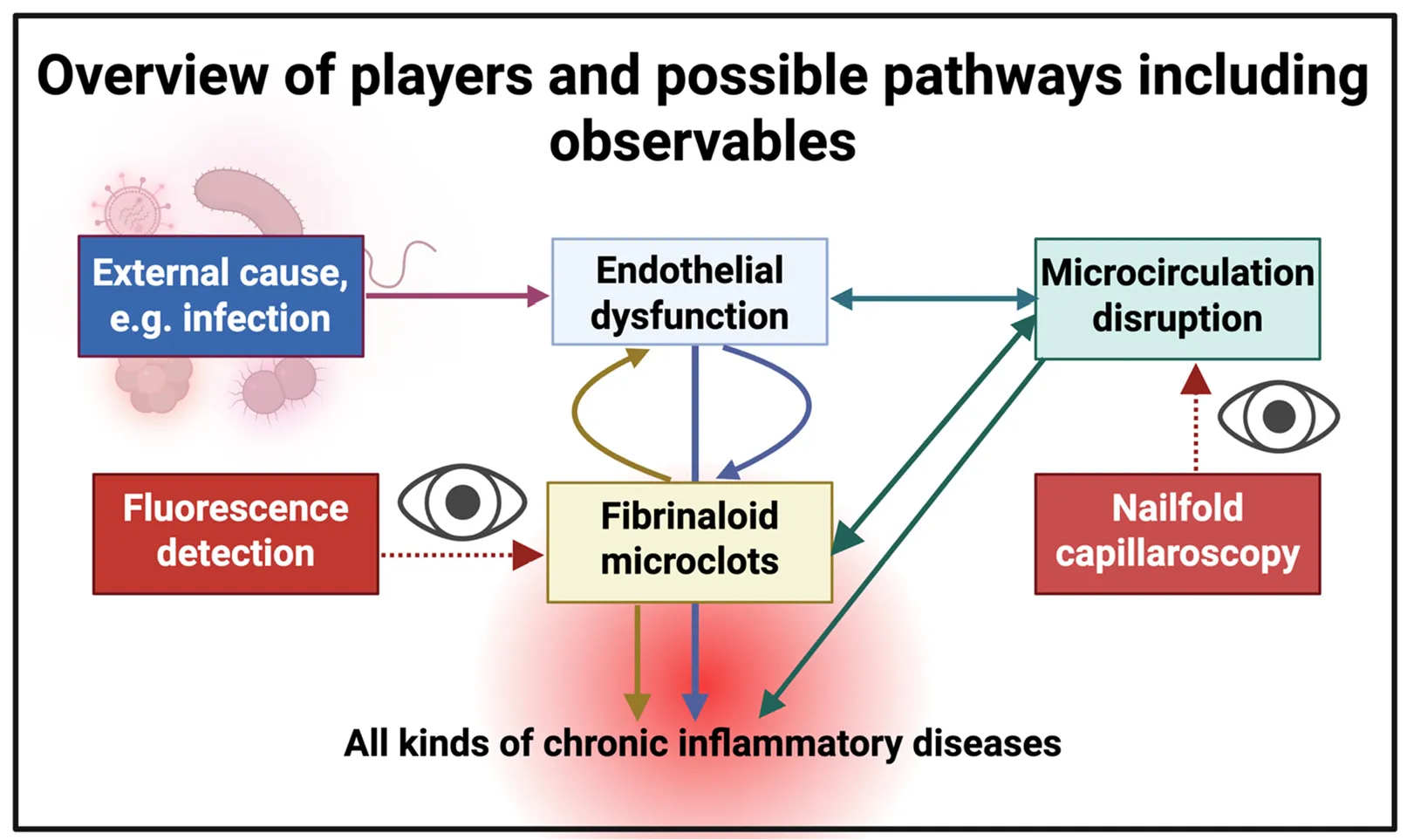
. Cartoon illustrating the systems aspects of the main features of this prospective review. Endothelial dysfunction, the result of a deterministic ‘external’ cause such as (a new or reactivated) infection, trauma, or stress, leads to the disruption of the microcirculation and to fibrinaloid microclots, each of which can potentially exacerbate the others. Our focus here is on nailfold capillaroscopy, though we have rehearsed the methods for microclot detection. Endothelial (dys)function <i>in vivo</i> is commonly assessed via flow-mediated dilatation [
117,
423] or various biomarkers (e.g., [
424,
425,
426,
427]). We anticipate that the combination of all three will be especially powerful in understanding the nature and severity of these kinds of disease, thereby assessing mechanisms and candidate treatments.
This review has purposely confined itself to nailfold capillaroscopy since relatively inexpensive equipment to implement the method is widely available. This said, we recognise that more sophisticated methods will likely provide much more power. 3D optoacoustic imaging (raster scanning optoacoustic mesoscopy) [
428,
429,
430] is one such approach, mirroring (in a certain sense) the developments [
431,
432,
433,
434,
435] in optoacoutstic infrared and Raman spectroscopy and imaging. Another trend towards using smart phones is taking photographs directly to assess digital lesions [
436,
437,
438].
Conceptualization, D.B.K. & E.P.; Formal Analysis, D.B.K. & E.P.; Resources, D.B.K. & E.P.; Writing—Original Draft Preparation, D.B.K.; Writing—Review & Editing, D.B.K. & E.P.; Visualization, D.B.K. & E.P.; Funding Acquisition, D.B.K. & E.P.
DBK thanks the Balvi Foundation (grant 18) and the Novo Nordisk Foundation for funding (grant NNF20CC0035580). EP thanks PolyBio Research Foundation and Kanro Foundation for funding. The content and findings reported and illustrated are the sole deduction, view and responsibility of the researchers and do not reflect the official position and sentiments of the funders. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
EP is a named inventor on a patent disclosing the use of fluorescence microscopy in Long COVID.
 Etheresia Pretorius
1,3,*
Etheresia Pretorius
1,3,*