2.1. VAERS Retrospective Analysis
This study identified candidate autoimmune AEs by ad hoc matching lists of autoimmune disease names with corresponding names used with the VAERS database; only a subset (20) of autoimmune AEs were examined. The VAERS database [
26] was retrospectively examined for the AEs designated by the following Medical Dictionary for Regulatory Activities (MedDRA) codes [
27]: Arthritis, Autoimmune thyroiditis, Chronic fatigue, Complex regional pain syndrome (CRPS), Diabetes mellitus, Eczema, Encephalitis autoimmune, Guillain barre (Guillain–Barré Syndrome), Henoch Schonlein purpura (Henoch-Schönlein purpura), Immune thrombocytopenia, Narcolepsy, Neutropenia, Polymyalgia rheumatica, Postural orthostatic tachycardia syndrome (POTS), Psoriasis, Raynaud’s phenomenon, Restless legs syndrome, Rheumatoid arthritis, Systemic lupus erythematosus, and Vasculitis. MedDRA
®, the Medical Dictionary for Regulatory Activities terminology, is the international medical terminology developed under the auspices of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). The downloaded VAERS data includes all AEs reported from 1990 to 27 December 2024.
The Ruby program vaers_slice4.rb [
28,
29] (https://github.com/doricke/VAERS-Tools, accessed on 4 January 2025) was used for retrospective analysis of the VAERS data files VAERSDATA, VAERSSYMPTOMS, and VAERSVAX for the years 1990 to 2024 and NonDomestic. The vaers_slice4.rb program combination report tallies vaccine AEs and generates multiple summary reports. This study focused on AEs by vaccine combination and age. The vaers_slice4.rb program calculates the frequencies of reported AEs normalized to 100,000 VAERS reports [
30]: AE normalized frequency = (observed AEs/all vaccine AEs)∗100,000. These normalized frequencies do not represent true incidence rates (asymptomatic individuals not included) but estimated rates of reported AEs. To avoid duplicate data, data is tabulated by unique “vaers_id” identifier. The tool vaers_slice4.rb uses “Unknown” when no gender is specified, −1 when no day of onset is specified, and −1 when no age is provided in VAERS. Vaccine combinations are defined when two or more vaccines a documented for a vaers_id; VAERS data is tallied by vaccine(s) in the combinations report (Supplemental Data tables). The vaers_slice4.rb program inputs a list of one or more MedDRA names (used by VAERS). Microsoft Excel was used to prepare figures and calculate Pearson correlation coefficient. Normalized frequencies were filtered for a minimum of 200 per 100,000 VAERS reports and a minimum of five AEs for vaccine or vaccine combination. Vaccines and vaccine combinations including the text “no brand name”, “foreign”, “unknown”, and “vaccine not specified” were excluded to avoid possible reporting biases (possibility of underrepresentation of less severe AEs resulting in increased normalized frequency estimates).
2.2. Adverse Events Following Immunization
Adverse events (
X) following immunization can be represented as the sum of immunization associated AEs (if any) and background (
B) (if any) occurrences of adverse events. A background AE is considered an event that occurs independent of immunization in the population being examined (sampled) during the time period examined; background AEs are not considered associated with immunizations. The reported AEs diminish due to reporting bias as the time since immunization increases (as time increases, fewer AEs are reported). Vaccine associated AEs can be modeled by the risks related to specific vaccine components (
C), excipients (
E) (if any), manufacturing contaminants (
M) (if any), and population background (
B) events in
Equation (1).
Coadministered vaccine AEs can be modeled by
Equation (2).
If
AE(
V|X) = 0 for multiple vaccines for adverse event
X, then each of the components
Ci, Ej, and
Mk, are all approximately zero for these vaccines and
B is approximately zero for all vaccines. If
AE(
V|X) = 0 for multiple vaccines and
AE(
V|X) >> 0 for other vaccines (second vaccine set), then there are vaccine associated AEs for the second set of vaccines.
For each autoimmune AEs examined, an upper limit for background (B
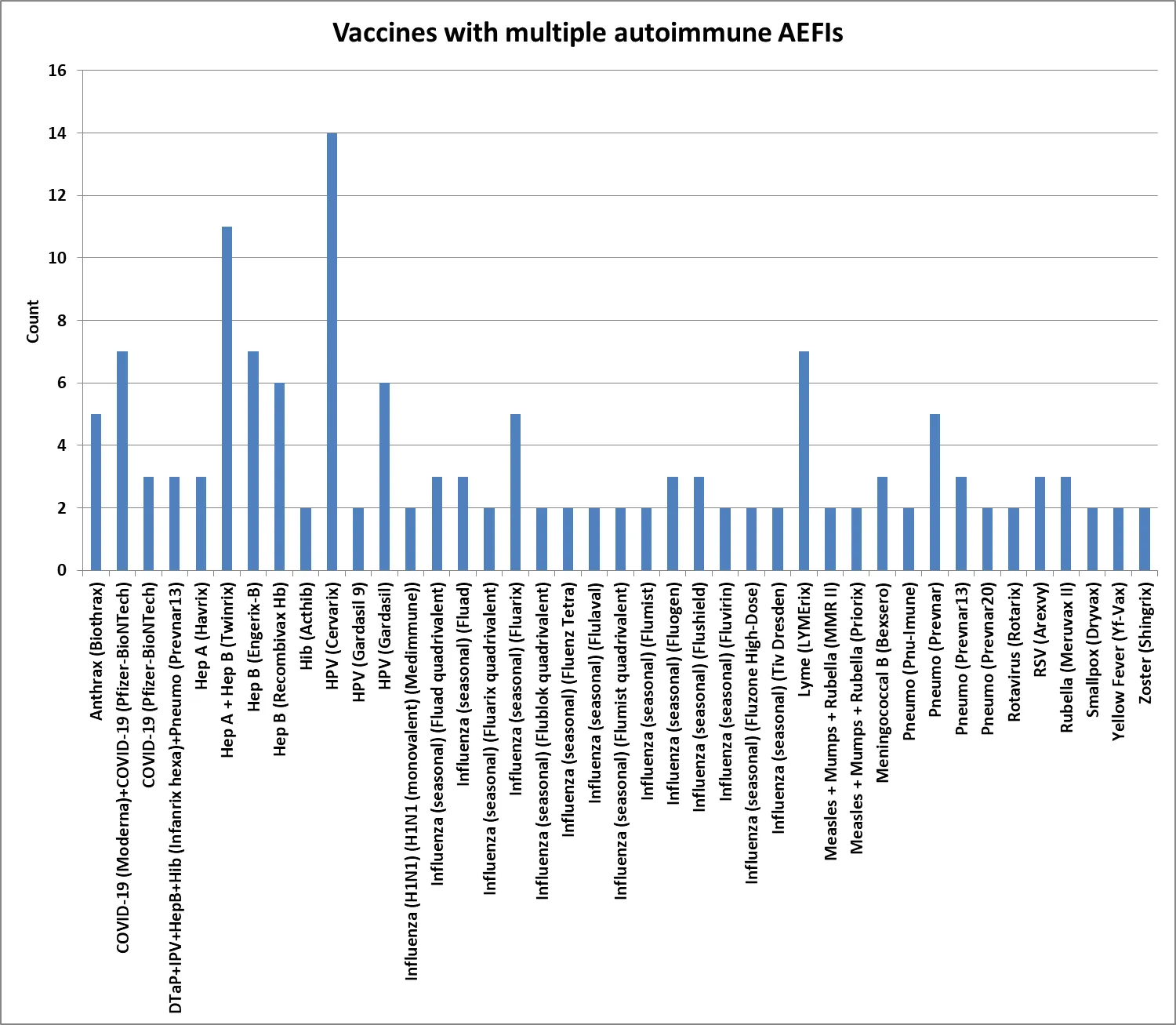
X) < 50 per 100,000 VAERS reports can be estimated from . The normalized frequencies for multiple autoimmune AEs from VAERS are summarized in and , , , , and . The normalized frequencies vary by vaccine for each AE, with multiple vaccines observed for two or more autoimmune AEs with normalized frequencies greater than or equal to 200 per 100,000 VAERS reports. An adverse event following immunization (AEFI) refers to any unfavorable or unintended medical occurrence after a person receives a vaccination. Vaccines with multiple AEFIs are summarized in . Vaccines with at least 2000 autoimmune AEs per 100,000 VAERS reports and at least 500 VAERS reports are summarized in .
.
Example normalized frequencies for estimating the upper limit of background (BX) adverse events, less than 50 per 100,000 VAERS reports for all adverse events.
| Adverse Event |
Vaccine(s) |
Normalized Frequency |
| Arthritis |
Smallpox + Monkeypox (Jynneos) |
47.4 |
| Arthritis |
Influenza (seasonal) (Fluvirin) + Pneumo (Pneumovax) |
39.4 |
| Arthritis |
Typhoid live Oral Ty21A (Vivotif) |
38.8 |
| Arthritis |
Varicella (Varivax) |
29.1 |
| Arthritis |
Meningococcal conjugate (Menveo) |
19.9 |
| Autoimmune thyroiditis |
Tdap (Adacel) |
7.6 |
| Autoimmune thyroiditis |
Varicella (Varivax) |
7.3 |
| Autoimmune thyroiditis |
Zoster (Shingrix) |
4.3 |
| Autoimmune thyroiditis |
Zoster live (Zostavax) |
2.6 |
| Autoimmune thyroiditis |
Pneumo (Pneumovax) |
2.3 |
| Chronic fatigue syndrome |
Influenza (seasonal) (Fluarix) |
20.5 |
| Chronic fatigue syndrome |
COVID-19 (Moderna bivalent) |
17.7 |
| Chronic fatigue syndrome |
Zoster live (Zostavax) |
10.3 |
| Chronic fatigue syndrome |
Zoster (Shingrix) |
8.6 |
| Chronic fatigue syndrome |
Pneumo (Pneumovax) |
2.3 |
| Complex regional pain syndrome |
COVID-19 (Moderna) |
6.9 |
| Complex regional pain syndrome |
Pneumo (Pneumovax) |
6.9 |
| Complex regional pain syndrome |
Zoster (Shingrix) |
5.8 |
| Complex regional pain syndrome |
Zoster live (Zostavax) |
5.1 |
| Complex regional pain syndrome |
COVID-19 (Pfizer-BioNTech bivalent) |
4.5 |
| Diabetes mellitus |
HPV (Gardasil 9) |
23.9 |
| Diabetes mellitus |
Influenza (seasonal) (Fluzone high-dose) |
23.9 |
| Diabetes mellitus |
Measles + Mumps + Rubella (MMR II)+Varicella (Varivax) |
18.5 |
| Diabetes mellitus |
Influenza (seasonal) (Fluzone quadrivalent) |
17.5 |
| Diabetes mellitus |
Zoster live (Zostavax) |
12.8 |
| Eczema |
Influenza (seasonal) (Flumist quadrivalent) |
30.8 |
| Eczema |
Influenza (seasonal) (Fluzone quadrivalent) |
26.2 |
| Eczema |
Pneumo (Pneumovax) |
25.2 |
| Eczema |
Influenza (H1N1 monovalent) (Sanofi) |
24.2 |
| Eczema |
Hep A (Vaqta) |
13.3 |
| Encephalitis autoimmune |
Influenza (seasonal) (Fluvirin) |
7 |
| Encephalitis autoimmune |
Pneumo (Prevnar13) |
6.7 |
| Encephalitis autoimmune |
COVID-19 (Janssen) |
6.1 |
| Encephalitis autoimmune |
Zoster (Shingrix) |
2.9 |
| Encephalitis autoimmune |
Pneumo (Pneumovax) |
2.3 |
| Guillain–Barré Syndrome |
Hib (Acthib) |
43.9 |
| Guillain–Barré Syndrome |
DTaP + IPV + Hib (Pentacel) |
42 |
| Guillain–Barré Syndrome |
COVID-19 (Moderna bivalent) |
41.2 |
| Guillain–Barré Syndrome |
Measles + Mumps + Rubella + Varicella (Proquad) |
9 |
| Henoch-Schönlein purpura |
Influenza (seasonal) (Fluzone high-dose) |
8 |
| Henoch-Schönlein purpura |
Zoster live (Zostavax) |
7.7 |
| Henoch-Schönlein purpura |
Influenza (seasonal) (Fluvirin) |
7 |
| Henoch-Schönlein purpura |
COVID-19 (Moderna bivalent) |
5.9 |
| Henoch-Schönlein purpura |
Zoster (Shingrix) |
5.8 |
| Immune thrombocytopenia |
Influenza (seasonal) (Fluzone quadrivalent) |
8.7 |
| Immune thrombocytopenia |
Hep B (Engerix-B) |
8.6 |
| Immune thrombocytopenia |
Varicella (Varivax) |
4.8 |
| Immune thrombocytopenia |
Influenza (seasonal) (Fluzone) |
4.1 |
| Immune thrombocytopenia |
Zoster live (Zostavax) |
2.6 |
| Narcolepsy |
Influenza (seasonal) (Fluzone quadrivalent) |
8.7 |
| Narcolepsy |
COVID-19 (Janssen) |
8.2 |
| Narcolepsy |
COVID-19 (Moderna) |
7.5 |
| Narcolepsy |
Pneumo (Prevnar13) |
6.7 |
| Narcolepsy |
COVID-19 (Pfizer-BioNTech bivalent) |
4.5 |
| Neutropenia |
COVID-19 (Moderna) |
17.1 |
| Neutropenia |
Pneumo (Pneumovax) |
16 |
| Neutropenia |
HPV (Gardasil 9) |
11.9 |
| Neutropenia |
Zoster live (Zostavax) |
10.3 |
| Neutropenia |
Zoster (Shingrix) |
5.8 |
| Polymyalgia rheumatica |
Influenza (H1N1 monovalent) (Sanofi) |
24.2 |
| Polymyalgia rheumatica |
Pneumo (Prevnar) |
22.8 |
| Polymyalgia rheumatica |
Tdap (Adacel) |
7.6 |
| Polymyalgia rheumatica |
HPV (Gardasil) |
2.7 |
| Polymyalgia rheumatica |
Varicella (Varivax) |
2.4 |
| Postural orthostatic tachycardia syndrome |
Influenza (seasonal) (Fluzone) |
12.2 |
| Postural orthostatic tachycardia syndrome |
Influenza (seasonal) (Fluarix quadrivalent) |
11.7 |
| Postural orthostatic tachycardia syndrome |
Hep B (Recombivax Hb) |
5.7 |
| Postural orthostatic tachycardia syndrome |
Zoster (Shingrix) |
2.9 |
| Postural orthostatic tachycardia syndrome |
Pneumo (Pneumovax) |
2.3 |
| Psoriasis |
Influenza (seasonal) (Flucelvax quadrivalent) |
16.7 |
| Psoriasis |
Hep A (Vaqta) |
13.3 |
| Psoriasis |
Varicella (Varivax) |
12.1 |
| Psoriasis |
Pneumo (Pneumovax) |
11.5 |
| Psoriasis |
Influenza (seasonal) (Fluzone) |
4.1 |
| Raynaud’s phenomenon |
Zoster (Shingrix) |
7.2 |
| Raynaud’s phenomenon |
Pneumo (Pneumovax) |
6.9 |
| Raynaud’s phenomenon |
Pneumo (Prevnar13) |
6.7 |
| Raynaud’s phenomenon |
Influenza (seasonal) (Fluzone) |
4.1 |
| Raynaud’s phenomenon |
Varicella (Varivax) |
2.4 |
| Restless legs syndrome |
Influenza (seasonal) (Fluzone) |
16.2 |
| Restless legs syndrome |
Zoster live (Zostavax) |
10.3 |
| Restless legs syndrome |
Pneumo (Prevnar13) |
6.7 |
| Restless legs syndrome |
Hep B (Recombivax Hb) |
5.7 |
| Restless legs syndrome |
Pneumo (Pneumovax) |
2.3 |
| Rheumatoid arthritis |
Smallpox (Dryvax) |
39.3 |
| Rheumatoid arthritis |
Influenza (seasonal) (Fluzone high-dose) |
31.8 |
| Rheumatoid arthritis |
Varicella (Varivax) |
19.4 |
| Rheumatoid arthritis |
Influenza (seasonal) (Fluzone high-dose quadrivalent) |
18 |
| Rheumatoid arthritis |
Influenza (seasonal) (Flucelvax quadrivalent) |
16.7 |
| Systemic lupus erythematosus |
COVID-19 (Pfizer-BioNTech bivalent) |
22.3 |
| Systemic lupus erythematosus |
Pneumo (Pneumovax) |
20.6 |
| Systemic lupus erythematosus |
Varicella (Varivax) |
9.7 |
| Systemic lupus erythematosus |
Influenza (seasonal) (Fluzone quadrivalent) |
8.7 |
| Systemic lupus erythematosus |
Influenza (seasonal) (Fluzone high-dose) |
8 |
| Vasculitis |
Tdap (Adacel) |
30.6 |
| Vasculitis |
Meningococcal conjugate (Menactra) |
21.8 |
| Vasculitis |
Influenza (seasonal) (Flumist) |
18.9 |
| Vasculitis |
Measles + Mumps + Rubella + Varicella (Proquad) |
18.1 |
| Vasculitis |
Influenza (seasonal) (Flucelvax quadrivalent) |
16.7 |
.
Normalized frequencies for multiple autoimmune AEs (excluding Arthritis, Rheumatoid arthritis, Eczema, Guillain–Barré Syndrome, Henoch-Schönlein purpura, and Vasculitis).
| Adverse Event |
Vaccines |
Normalized Frequency |
Chi-Square 2 × 2 p-Value |
| Autoimmune thyroiditis |
COVID-19 (Moderna) + COVID-19 (Pfizer-BioNTech) |
258 |
<0.00001 |
| Autoimmune thyroiditis |
Hep A + Hep B (Twinrix) |
434 |
<0.00001 |
| Autoimmune thyroiditis |
HPV (Cervarix) |
212 |
<0.00001 |
| Chronic fatigue |
Anthrax (Biothrax) |
243 |
<0.00001 |
| Chronic fatigue |
COVID-19 (Moderna) + COVID-19 (Pfizer-BioNTech) |
335 |
<0.00001 |
| Chronic fatigue |
Hep A + Hep B (Twinrix) |
241 |
<0.00001 |
| Chronic fatigue |
HPV (Cervarix) |
1569 |
<0.00001 |
| Chronic fatigue |
HPV (Gardasil) |
397 |
<0.00001 |
| Complex regional pain syndrome (CRPS) |
HPV (Cervarix) |
1060 |
<0.00001 |
| Diabetes mellitus |
Anthrax (Biothrax) |
486 |
<0.00001 |
| Diabetes mellitus |
Hep A + Hep B (Twinrix) |
289 |
<0.00001 |
| Diabetes mellitus |
Hep B (Engerix-B) |
385 |
<0.00001 |
| Diabetes mellitus |
Lyme disease (LYMErix) |
457 |
<0.00001 |
| Diabetes mellitus |
Pneumo (Prevnar) |
228 |
<0.00001 |
| Encephalitis autoimmune |
HPV (Cervarix) |
233 |
<0.00001 |
| Encephalitis autoimmune |
Yellow Fever (Yf-Vax) |
322 |
<0.00001 |
| Immune thrombocytopenia |
Pneumo (Prevnar13) + Rotavirus (RotaTeq) |
5769 |
<0.00001 |
| Narcolepsy |
HPV (Cervarix) |
615 |
<0.00001 |
| Narcolepsy |
Influenza (H1N1 monovalent) (GSK)) |
11,539 |
<0.00001 |
| Narcolepsy |
Influenza (seasonal) (Fluenz Tetra) |
2100 |
<0.00001 |
| Narcolepsy |
Influenza (seasonal) (Flumist quadrivalent) |
370 |
<0.00001 |
| Neutropenia |
DTaP + IPV + HepB + Hib (Infanrix Hexa)+Pneumo (Prevnar) |
1139 |
<0.00001 |
| Neutropenia |
DTaP + IPV + HepB + Hib (Infanrix Hexa)+Pneumo (Prevnar13) |
712 |
<0.00001 |
| Neutropenia |
Meningococcal B (Bexsero) |
278 |
<0.00001 |
| Neutropenia |
Pneumo (Prevnar) |
274 |
<0.00001 |
| Neutropenia |
Rotavirus (Rotarix) |
249 |
<0.00001 |
| Polymyalgia rheumatica |
COVID-19 (Moderna) + COVID-19 (Pfizer-BioNTech) |
206 |
<0.00001 |
| Polymyalgia rheumatica |
Influenza (seasonal) (Fluad quadrivalent) |
252 |
<0.00001 |
| Polymyalgia rheumatica |
Influenza (seasonal) (Fluad) |
383 |
<0.00001 |
| Polymyalgia rheumatica |
Influenza (seasonal) (Fluarix) |
287 |
<0.00001 |
| Polymyalgia rheumatica |
Lyme disease (LYMErix) |
411 |
<0.00001 |
| POTS |
HPV (Cervarix) |
1229 |
<0.00001 |
| POTS |
HPV (Gardasil 9) |
472 |
<0.00001 |
| POTS |
HPV (Gardasil 9) + HPV (Gardasil) |
2703 |
<0.00001 |
| POTS |
HPV (Gardasil) |
1223 |
<0.00001 |
| Psoriasis |
COVID-19 (Moderna) + COVID-19 (Pfizer-BioNTech) |
464 |
<0.00001 |
| Psoriasis |
Hep A + Hep B (Twinrix) |
217 |
<0.00001 |
| Raynaud’s phenomenon |
Lyme disease (LYMErix) |
548 |
<0.00001 |
| Restless legs syndrome |
HPV (Cervarix) |
254 |
<0.00001 |
| Systemic lupus erythematosus |
Hep A + Hep B (Twinrix) |
362 |
<0.00001 |
| Systemic lupus erythematosus |
Hep B (Engerix-B) |
492 |
<0.00001 |
| Systemic lupus erythematosus |
Hep B (Recombivax Hb) |
321 |
<0.00001 |
| Systemic lupus erythematosus |
HPV (Cervarix) |
911 |
<0.00001 |
| Systemic lupus erythematosus |
HPV (Gardasil) |
419 |
<0.00001 |
| Systemic lupus erythematosus |
Lyme disease (LYMErix) |
503 |
<0.00001 |
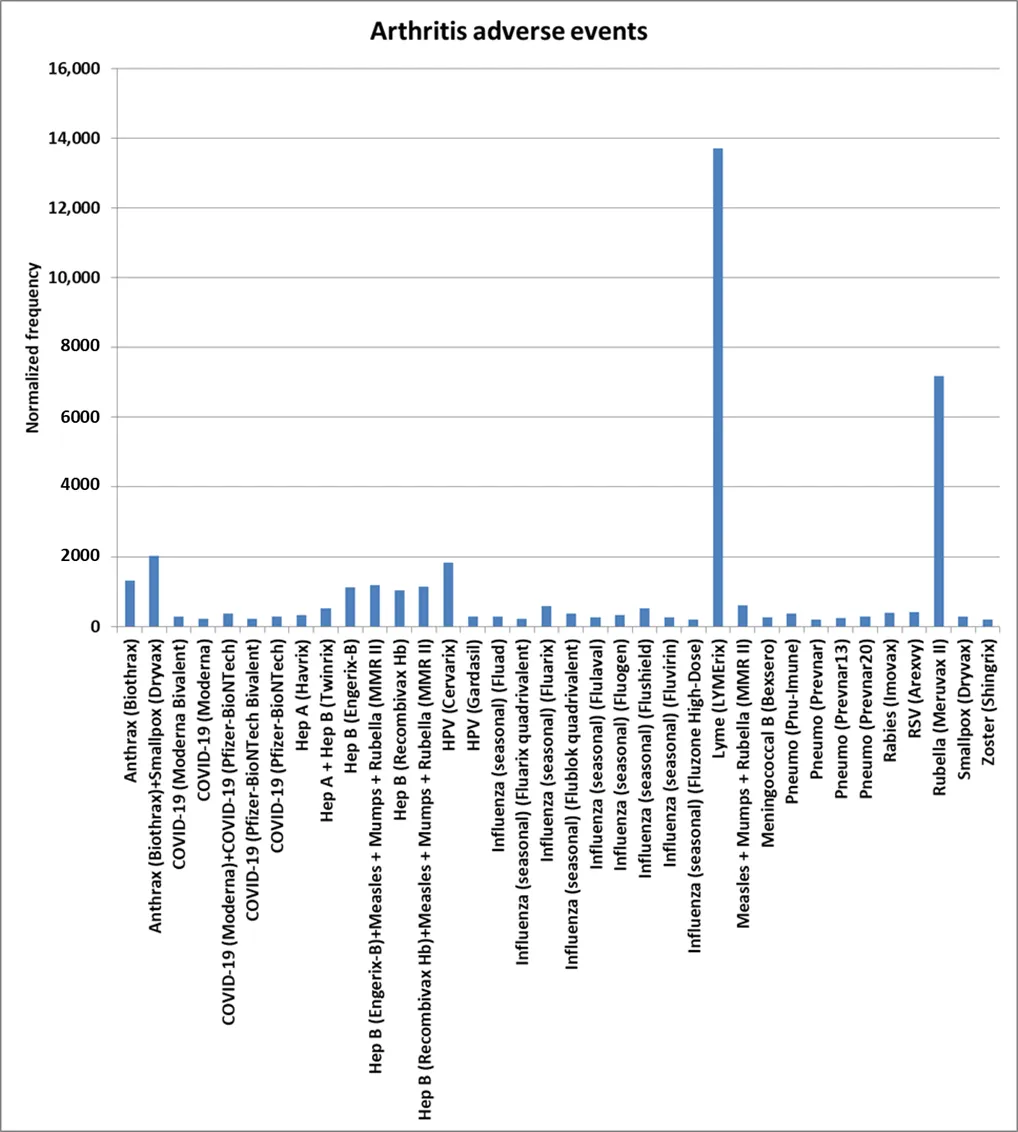
. Arthritis AEs normalized frequencies.
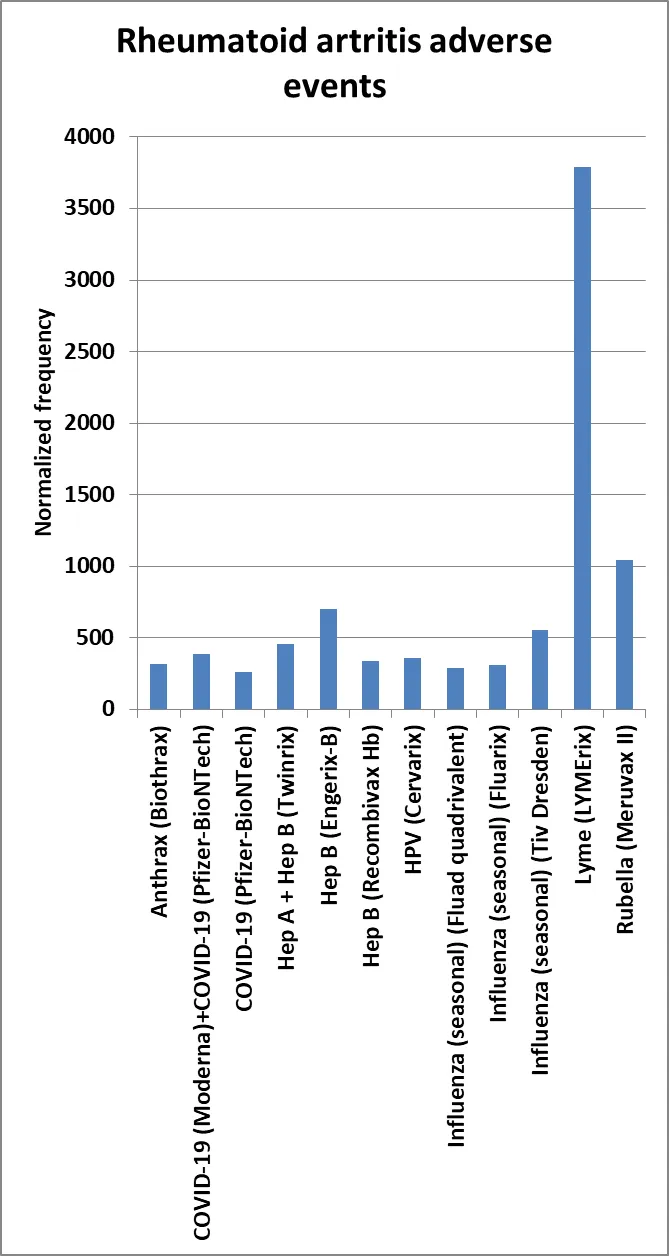
. Rheumatoid arthritis (RA) AEs normalized frequencies.
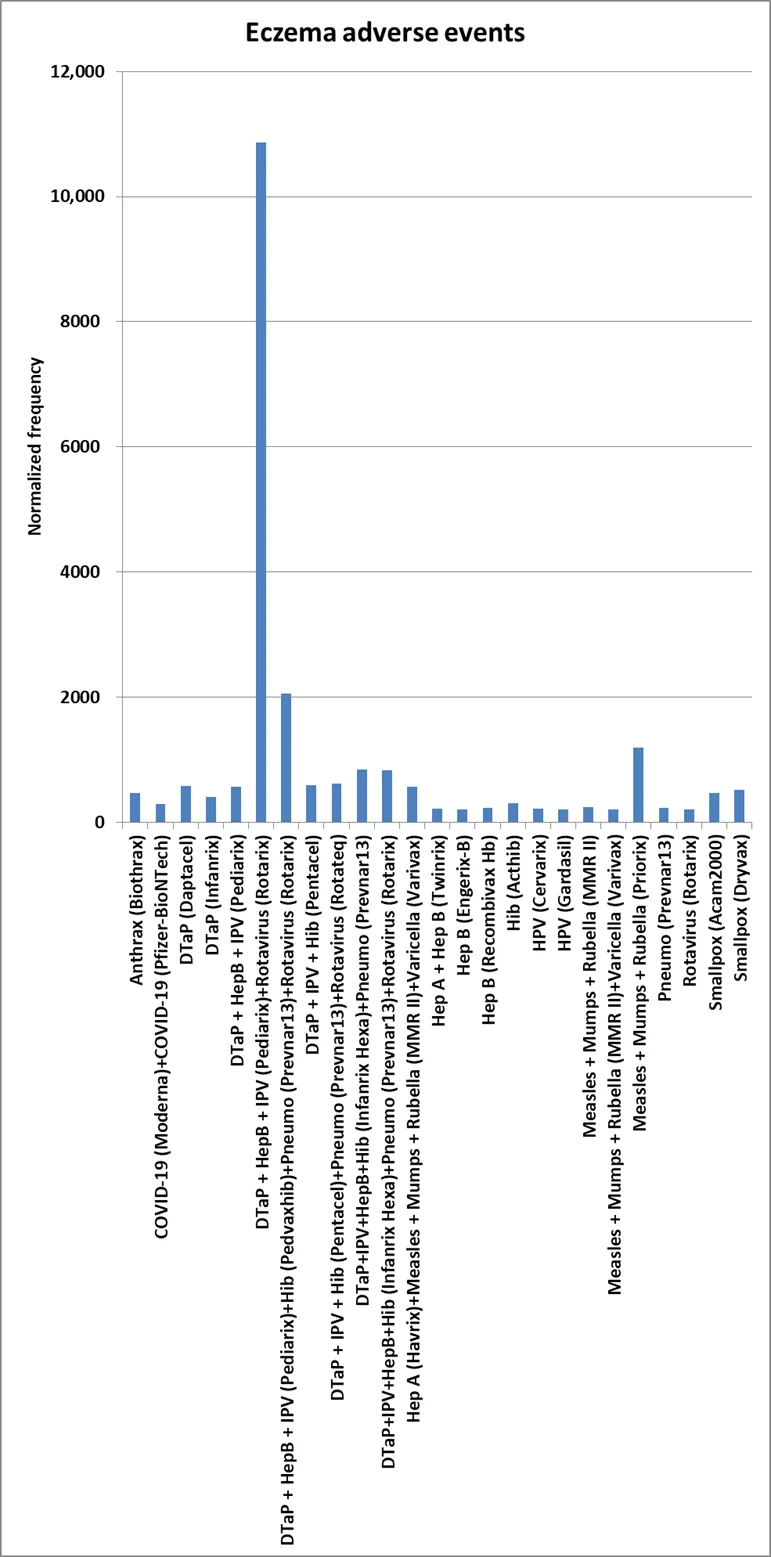
. Eczema AEs normalized frequencies.
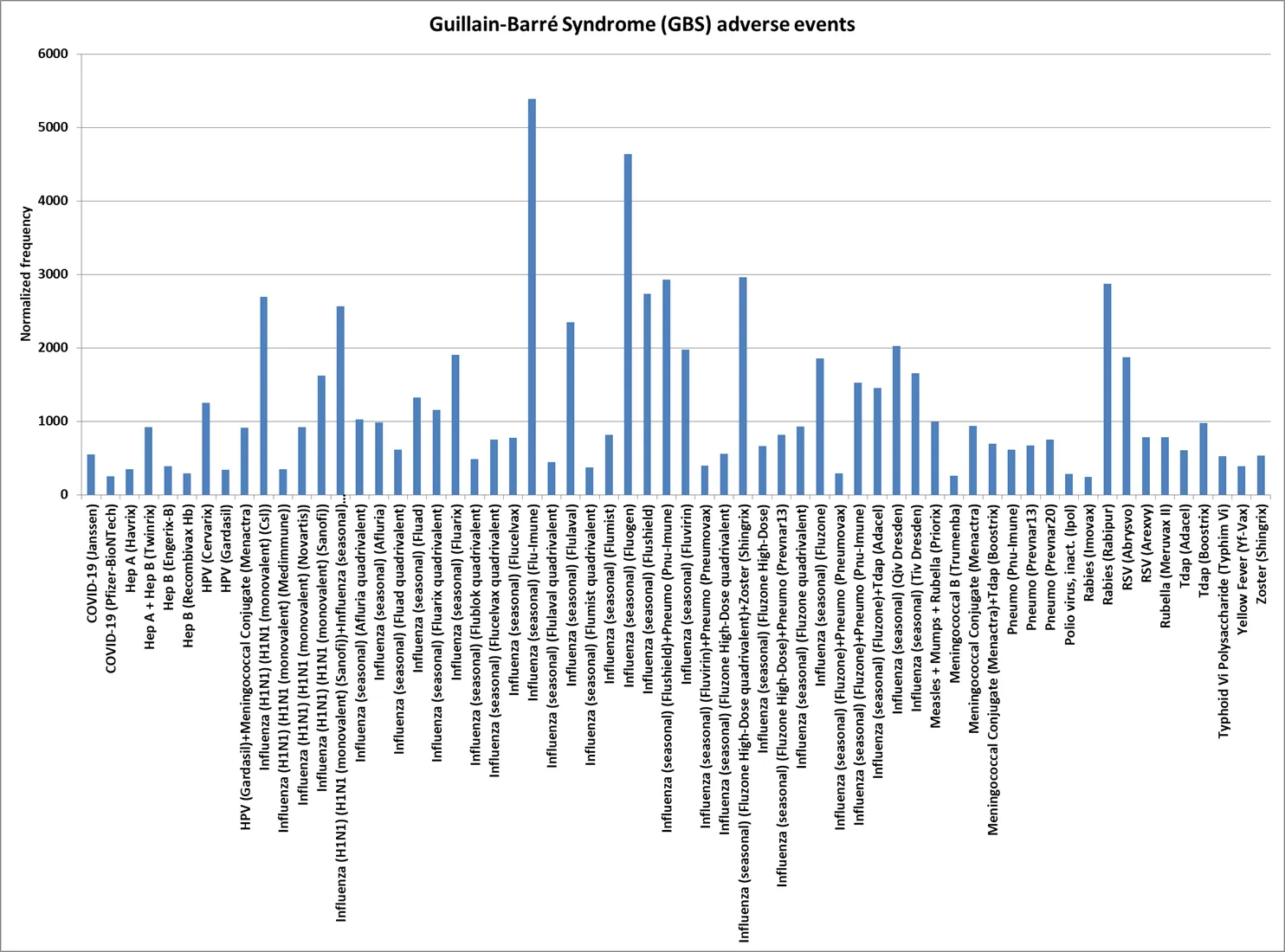
. Guillain–Barré Syndrome (GBS) AEs normalized frequencies.
. Henoch-Schönlein purpura (HSP) AEs normalized frequencies.
. Vasculitis AEs normalized frequencies.
. Vaccines with multiple AEFIs.
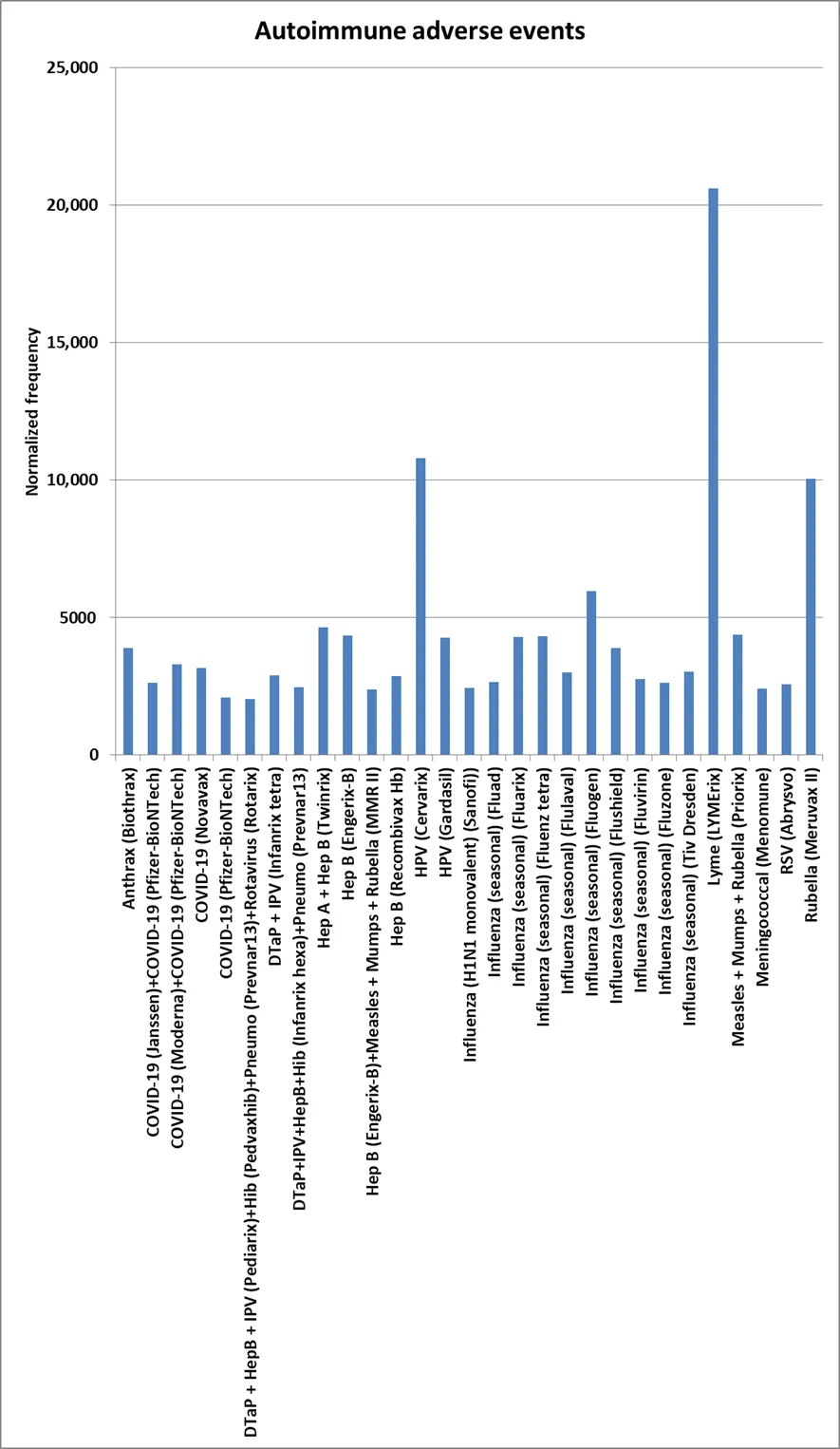
. Autoimmune adverse events with normalized frequency of at least 2000 per 100,000 VAERS reports for one or more autoimmune adverse events and a minimum of 500 VAERS reports.
Inflammation or swelling of one or more joints, surrounding tissues, or other connective tissues is arthritis. RA is an autoimmune disease causing joint inflammation, swelling, pain, and stiffness. Normalized frequencies for Arthritis AEs include Lyme disease (LYMErix) at 13,711 per 100,000 (1 in 7) (chi-square 2 × 2
p < 0.00001) (gender neutral), Rubella (Meruvax II) at 7171 (1 in 14) (
p < 0.00001) (27:1 female bias), Anthrax (Biothrax) + Smallpox (Dryvax) at 2027 (
p < 0.00001), HPV (Cervarix) at 1823 (
p < 0.00001) (females), Anthrax (Biothrax) at 1313 (
p < 0.00001) (7.7× male), Hep B (Engerix-B) at 1113 (
p < 0.00001) (2.6× female), and Hep B (Recombivax Hb) at 1038 (
p < 0.00001) (2.5× female) all per 100,000 VAERS reports (
). Normalized frequencies for Rheumatoid arthritis AEs parallel Arthritis AEs with Lyme disease (LYMErix) at 3793 (1 in 26) (
p < 0.00001) (gender neutral), Rubella (Meruvax II) at 1043 (
p < 0.00001) (all female), and Hep B (Engerix-B) at 702 (
p < 0.00001) (2.8× female) all per 100,000 VAERS reports (
). The RA AEs (
) have a Pearson correlation coefficient r = 0.95 with the matching normalized frequencies for arthritis AEs (
). While clinical trials detected no associations, arthritis and autoimmune arthritis have been reported following Lyme disease vaccination [
31,
32]. The LYMErix and Meruvax II vaccines may have specific vaccine components, $$C_{i}^{X}$$, contributing to both of the AEs.
3.2. Eczema Adverse Events
Eczema (aka, atopic dermatitis) is characterized by dry, itchy, and inflamed skin. Normalized frequencies for Eczema AEs include DTaP + HepB + IPV (Pediarix) + Rotavirus (Rotarix) at 10,870 for 5 out of 46 reports (
p < 0.00001), DTaP + HepB + IPV (Pediarix) + Hib (Pedvaxhib) + Pneumo (Prevnar13) + Rotavirus (Rotarix) at 2048 (
p < 0.00001), and Measles + Mumps + Rubella (Priorix) at 1191 (
p < 0.00001) (infants) all per 100,000 VAERS reports (
). Note that the normalized frequency estimate for DTaP + HepB + IPV (Pediarix) + Rotavirus (Rotarix) is likely overestimated due to the small number (46) of all VAERS reports for this vaccine combination.
3.3. Guillain–Barré Syndrome (GBS) Adverse Events
GBS is a neurological disease where the immune system attacks peripheral nervous system, leading to muscle weakness and sometimes paralysis. Normalized frequencies for GBS include 19 Influenza vaccines or combinations including an Influenza vaccine with normalized frequencies between 1022 (
p < 0.00001) (Afluria quadrivalent) and 5385 (
p < 0.00001) (Flu-Imune), Rabies (Rabipur) at 2869 (
p < 0.00001), RSV (Abrysvo) at 1868 (
p < 0.00001), and HPV (Cervarix) at 1251 (
p < 0.00001) (females) all per 100,000 VAERS reports (
). An additional 16 Influenza vaccines or combinations including Influenza have normalized frequencies between 200 and 1000 per 100,000 VAERS Reports (
). GBS has been linked to influenza vaccination [
9,
10,
11]. It is plausible to suspect an antigen in influenza vaccine components contributing to GBS.
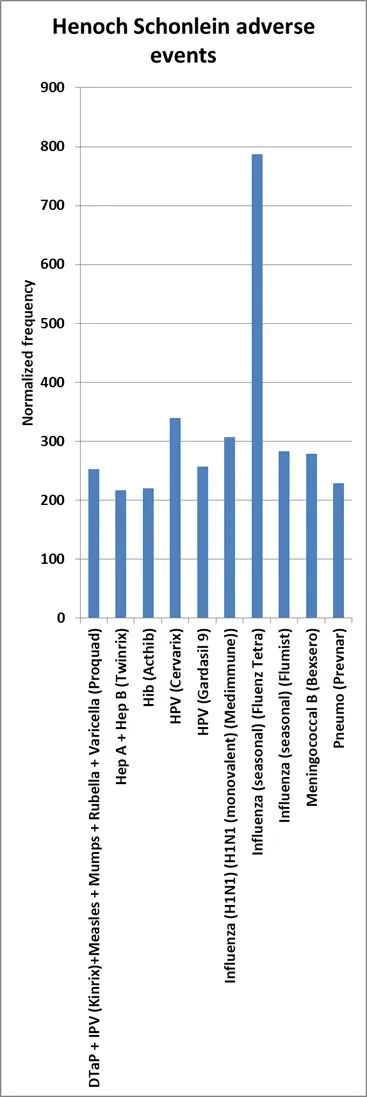
3.4. Henoch-Schönlein Purpura (HSP) Adverse Events
HSP (aka, IgA vasculitis) is inflammation in small blood vessels, often leading to rash, joint pain, and abdominal pain. The highest normalized frequencies for Henoch-Schönlein purpura AEs include Influenza (seasonal) (Fluenz tetra) at 787 (
p < 0.00001), and HPV (Cervarix) at 339 (
p < 0.00001), all per 100,000 VAERS reports (
). A case of HSP following rabies immunization has been reported [
33]. A potential false signal for Polio virus, inact. (Poliovax) was excluded from the results.
3.5. Immune Thrombocytopenia (ITP) Adverse Events
ITP occurs when the immune system attacks and destroys platelets, leading to a low platelet count. coadministered vaccines Pneumo (Prevnar13) + Rotavirus (RotaTeq) have an immune thrombocytopenia normalized frequency of 5769 (
p < 0.00001) based on 9 reports for 156 VAERS reports (
). Immune thrombocytopenia has been reported post COVID-19 immunization [
34]. Normalized frequencies for immune thrombocytopenia for COVID-19 Pfizer-BioNTech were 123, and for COVID-19 Janssen were 114 (below the threshold for inclusion in this study). Unusual thrombotic events and thrombocytopenia with autoantibodies targeting platelet factor 4 (PF4) have been advanced in association with the AstraZeneca (AZD1222) ChAdOx1 SARS-CoV-2 vaccine with the suggested name of vaccine induced prothrombotic immune thrombocytopenia (VIPIT) [
35,
36,
37].
3.6. Narcolepsy Adverse Events
Narcolepsy is a neurological disorder characterized by excessive daytime sleepiness despite adequate sleep at night. Narcolepsy occurs when the immune system attacks brain cells that produce hypocretin (aka, orexin). Hypocretin is important in regulating sleep and wakefulness. Influenza (H1N1 monovalent) GSK has a normalized frequency of 11,539 (
p < 0.00001) for 12 of 104 VAERS reports and Influenza (seasonal) (Fluenz tetra) of 2100 (
p < 0.00001) (
). Narcolepsy has been linked to the 2009 influenza H1N1 vaccine [
8]. Antibodies to influenza 2009 A(H1N1) nucleoprotein were found to be cross-reacting with human hypocretin receptor 2 [
37].
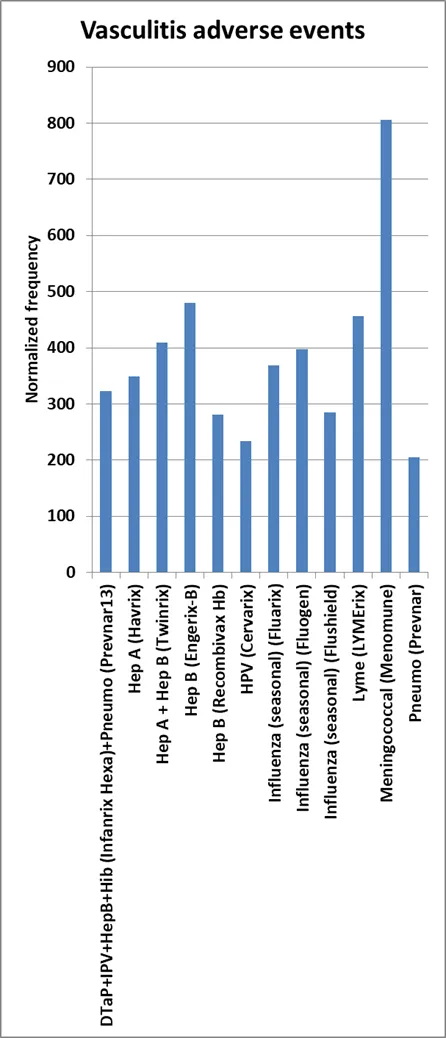
3.7. Vasculitis Adverse Events
Vasculitis is characterized by inflamed blood vessels. The highest normalized frequencies for Vasculitis AEs include Meningococcal (Menomune) at 807 (
p < 0.00001) (3x male), Hep B (Engerix-B) at 479 (
p < 0.00001) (1.5x female), Lyme disease (LYMErix) at 457 (
p < 0.00001) (1.5x female), and Hep A + Hep B (Twinrix) at 410 (
p < 0.00001) (gender neutral) all per 100,000 VAERS reports (
). A case of urticarial vasculitis was reported following meningococcal serogroup B vaccination [
38]. A case of urticarial vasculitis has been reported following meningococcal serogroup B immunization [
38].
3.8. Anthrax Vaccine Adverse Events
Anthrax (Biothrax) AEs normalized frequencies include Arthritis (1313 per 100,000 VAERS reports,
p < 0.00001), Chronic fatigue (243,
p < 0.00001), Diabetes mellitus (486,
p < 0.00001), Eczema (462,
p < 0.00001) and Rheumatoid arthritis (316,
p < 0.00001). Anthrax (Biothrax) + Smallpox (Dryvax) had a higher Arthritis normalized frequency of 2027 per 100,000 VAERS reports (
p < 0.00001). Cases of RA [
39] and eczema [
40] have been reported following anthrax vaccination [
39].
3.9. COVID-19 Vaccine Adverse Events
Normalized frequencies for COVID-19 vaccines include Arthritis AEs for Moderna (222 per 100,000 VAERS reports,
p < 0.00001), Moderna + Pfizer-BioNTech (361,
p < 0.00001), Pfizer-BioNTech bivalent (219,
p < 0.00001), and Pfizer-BioNTech (293,
p < 0.00001), Autoimmune thyroiditis AEs for Moderna + Pfizer-BioNTech (258,
p < 0.00001), Chronic fatigue AEs for Moderna+Pfizer-BioNTech (335,
p < 0.00001), Eczema AEs for Moderna + Pfizer-BioNTech (284,
p < 0.00001), GBS AEs for Janssen (553,
p < 0.00001) and Pfizer-BioNTech (248,
p < 0.00001), Polymyalgia rheumatic for Moderna+Pfizer-BioNTech (206,
p < 0.00001), and Rheumatoid arthritis for Pfizer-BioNTech (261,
p < 0.00001) and Moderna+Pfizer-BioNTech (387,
p < 0.00001). Coadministration of COVID-19 Moderna and COVID-19 Pfizer-BioNTech (note: likely vaccine administration errors) was observed with seven autoimmune AEs safety signals. Examining Autoimmune thyroiditis, Chronic fatigue syndrome, Eczema, Polymyalgia rheumatica, Psoriasis, and Rheumatoid arthritis, Coadministration of COVID-19 (Moderna) with COVID-19 (Pfizer-BioNTech) has a normalized frequency of 1933 per 100,000 VAERS reports (
p < 0.00001) while individual administration has lower normalized frequencies of COVID-19 (Janssen) at 339, (
p = 0.0090) COVID-19 (Moderna) at 494 (
p = 0.00034), COVID-19 Pfizer-BioNTech at 918 (
p < 0.00001), COVID-19 Novavax at 998 (
p < 0.00001). Coadministration of COVID-19 Pfizer-BioNTech with Influenza (seasonal) (Fluzone quadrivalent) has a normalized frequency of 1235 (
p < 0.00001). Examining all of the autoimmune AEs in this study together, COVID-19 Moderna + COVID-19 Pfizer-BioNTech has a normalized frequency of 3299 (
p < 0.00001) for any of the autoimmune AEs (1 in 30 VAERS reports for these coadministered vaccines), COVID-19 Janssen + COVID-19 Pfizer-BioNTech normalized frequency of 2637 (
p < 0.00001), COVID-19 Novavax normalized frequency of 3161 (
p < 0.00001), and COVID-19 Pfizer-BioNTech normalized frequency of 2096 (
p < 0.00001) (
). Multiple autoimmune diseases have been reported following COVID-19 vaccination [
15,
16,
17,
18,
19,
20,
21,
22,
23,
24]. The timing of COVID-19 mRNA vaccine doses has also been linked with autoimmune AEs [
7].
3.10. Hepatitis Vaccines Autoimmune Adverse Events
Safety signals for Hepatitis A (Hep A) and/or Hepatitis B (Hep B) vaccines are observed for Arthritis AEs (6 times), Autoimmune thyroiditis (Twinrix), Chronic fatigue (Twinrix), Diabetes mellitus (twice), Eczema (4 times), GBS (4 times), Henoch-Schönlein purpura (Twinrix), Psoriasis (Twinrix), Rheumatoid arthritis (3 times), Systemic lupus erythematous (3 times), and Vasculitis (4 times). GBS has been reported after Hepatitis A vaccination [
41]. Systemic lupus erythematous has been reported after Hepatitis B vaccination [
42,
43].
3.11. Human Papillomavirus (HPV) Vaccines Adverse Events
Safety signals for HPV (Cervarix) were observed with fourteen autoimmune AEs (
): Arthritis (1823,
p < 0.00001), Autoimmune thyroiditis (212,
p < 0.00001), Chronic fatigue syndrome (1569,
p < 0.00001), Complex regional pain syndrome (CRPS) (1060,
p < 0.00001), Eczema (212,
p < 0.00001), Encephalitis autoimmune (233,
p < 0.00001), GBS (1251,
p < 0.00001), Henoch-Schönlein purpura (339,
p < 0.00001), Narcolepsy(615,
p < 0.00001), POTS (1229,
p < 0.00001), Restless legs syndrome (254,
p < 0.00001), Rheumatoid arthritis (360,
p < 0.00001), Systemic lupus erythematosus (911,
p < 0.00001), and Vasculitis (233,
p < 0.00001). Safety signals for HPV (Gardasil) were observed with six autoimmune AEs: Arthritis (290 per 100,000 VAERS reports), Chronic fatigue (397,
p < 0.00001), Eczema (201,
p < 0.00001), GBS (338,
p < 0.00001), POTS (1223,
p < 0.00001), and Systemic lupus erythematosus (419,
p < 0.00001). Safety signals for HPV (Gardasil 9) were observed for Henoch-Schönlein purpura (257,
p < 0.00001) and POTS (472,
p < 0.00001). A safety signal for coadministering HPV (Gardasil) with Meningococcal conjugate (Menactra) was observed for GBS (912,
p < 0.00001). The HPV AEs may be inflated by reporting bias [
44]; this would cause inflated normalized frequencies estimates and also artificially decrease calculated
p-values. A teenager developed POTS and chronic fatigue syndrome after Gardasil vaccination [
45]. HPV Cervarix and Gardasil use different manufacturing processes, common vaccine components, $$C_{i}^{X}$$, are likely candidates for these autoimmune diseases. Alternatively, HPV Cervarix and HPV Gardasil both contained (possibly overlapping) manufacturing contaminants ($$M_{k}^{X}$$) with some reduction for HPV Gardasil 9. The ASO4 adjuvant in HPV Cervarix together with the causative vaccine component(s) may contribute to the higher number of autoimmune AEs for HPV Cervarix compared to HPV Gardasil.
3.12. Influenza Vaccines Adverse Events
Safety signals for Influenza vaccines were observed with nine Arthritis AEs (207,
p < 0.00001, to 574,
p < 0.00001, per 100,000 VAERS reports), 35 GBS AEs (with 19 greater than 1000 per 100,000 VAERS reports), Henoch-Schönlein purpura (3 times), Narcolepsy (3 times), Polymyalgia rheumatic (3 times), Rheumatoid arthritis (3 times), and Vasculitis (3 times). The normalized frequency for Narcolepsy of 12 of 104 reports (
p < 0.00001) is likely overestimated due to the small number (104) of reports but Influenza (seasonal) (Fluenza Tetra) also had a normalized frequency of 2100 per 100,000 VAERS reports (
p < 0.00001).
3.13. Lyme Disease Vaccine AEs (8)
Safety signals for the Lyme disease (LYMErix) vaccine were observed with seven autoimmune AEs: Arthritis (13,711 per 100,000 VAERS reports,
p < 0.00001), Diabetes mellitus (457,
p < 0.00001), Polymyalgia rheumatica (457,
p < 0.00001), Raynaud’s phenomenon (548,
p < 0.00001), Rheumatoid arthritis (3793,
p < 0.00001), Systemic lupus erythematosus (503,
p < 0.00001), and Vasculitis (457,
p < 0.00001). The number of adverse events in VAERS for LYMErix may be increased due to reporting bias [
46]; this would also incorrectly decreased the calculated
p-values. The LYMErix vaccine may have specific vaccine components, $$C_{i}^{X}$$, contributing to these AEs. Four cases of arthritis following Lyme disease vaccination have been reported [
31].
3.14. Pneumococcal Vaccines Adverse Events
Safety signals for Pneumococcal vaccines AEs were observed for multiple autoimmune AEs, Pnu-immune: Arthritis (370 per 100,000 VAERS reports,
p < 0.00001) and GBS (616,
p < 0.00001), Prevnar: Arthritis (205,
p < 0.00001), Diabetes mellitus (228,
p < 0.00001), Henoch-Schönlein purpura (228,
p < 0.00001), Neutropenia (274,
p < 0.00001), and Vasculitis (205,
p < 0.00001), Prevnar13: Arthritis (236,
p < 0.00001), Eczema (223,
p < 0.00001), and GBS (668,
p < 0.00001), Prevnar20: Arthritis (277,
p < 0.00001) and GBS (753,
p < 0.00001), and Prevnar13 + Rotavirus (RotaTeq): Immune thrombocytopenia (5769 from 9 out of 156 reports,
p < 0.00001) (normalized frequency is likely overestimated). These autoimmune AEs may be the result of stimulations of immune responses.
4.1. Arthritis and Rheumatoid Arthritis Adverse (RA) Events
The three vaccines with the highest arthritis AE normalized frequencies are no longer distributed in the United States. The Lyme disease (LYMErix) vaccine was discontinued in 2002. The Rubella (Meruvax II) vaccine is a live attenuated (weakened) vaccine of the rubella virus for preventing rubella infection (German measles); it was discontinued in 2011. Also, the HPV (Cervarix) vaccine is no longer available in the United States. For arthritis, Anthrax (Biothrax) concomitantly administered with Smallpox (Dryvax) with normalized frequency of 2000 per 100,000 VAERS reports (
p < 0.00001) is somewhat higher than the individual vaccines Anthrax at 1313 (
p < 0.00001) and Smallpox at 275 (
p < 0.00001). The two Hep B vaccines (Engerix-B and Recombivax Hb) also have high normalized frequencies of 1112 (
p < 0.00001) and 1038 (
p < 0.00001), respectively. The very high Pearson correlation coefficient of 0.95 between the RA and arthritis AEs strongly indicates shared autoimmune etiologies between these two AEs.
4.2. Eczema Adverse Events
The higher eczema AEs normalized frequencies are DTaP + HepB + IPV (Pediarix) + Hib (Pedvaxhib) + Pneumo (Prevnar13) + Rotavirus (Rotarix) at 2048 (
p < 0.00001) per 100,000 VAERS reports based on 586 reports and Measles + Mumps + Rubella (Priorix) at 1191 (
p < 0.00001) based on 504 reports. Note that these are children’s vaccines. These normalized frequency estimates may decrease with additional VAERS reports for these vaccine combinations.
4.3. Guillain–Barré Syndrome (GBS) Adverse Events
Safety signals for GBS were observed with 62 vaccines or combinations of 35, including influenza vaccines.
Hypothesis 1 (H1). A component of the Influenza vaccines, VCInfluenza, may be associated with Guillain–Barré Syndrome; causative shared epitope(s) or peptide fragment(s) shared across these Influenza vaccines may be the source of these GBS associations.
Additional GBS associations include Hep A + Hep B (Twinrix) at 916 (
p < 0.00001), HPV (Cervarix) at 1251 (
p < 0.00001), Measles + Mumps + Rubella (Priorix) at 992 (
p < 0.00001), Rabies (Rabipur) at 2869 (
p < 0.00001), RSV (Arexvy) at 1868 (
p < 0.00001), and Tdap (Boostrix) at 976 (
p < 0.00001); these and other GBS vaccine associations may share the etiology related to non-specific immune responses.
4.4. COVID-19 Vaccines
Safety signals for concomitant administration of COVID-19 Moderna with Pfizer-BioNTech were observed with multiple autoimmune AEs: Arthritis (361 per 100,000 VAERS reports,
p < 0.00001), Autoimmune thyroiditis (258,
p < 0.00001), Chronic fatigue (335,
p < 0.00001), Eczema (284,
p < 0.00001), Polymyalgia rheumatica (206,
p < 0.00001), Psoriasis (464,
p < 0.00001), and Rheumatoid arthritis (387,
p < 0.00001). The normalized frequency of these 6 autoimmune AEs for these two shots combined is 1933 per 100,000 (1 in 52) VAERS reports. While individually, safety signals for COVID-19 Moderna were observed for Arthritis (222,
p < 0.00001) and COVID-19 Pfizer-BioNTech with Arthritis (293,
p < 0.00001), GBS (248,
p < 0.00001), and Rheumatoid arthritis (261,
p < 0.00001); for both GBS and Rheumatoid arthritis, corresponding estimated normalized frequencies for COVID-19 Pfizer-BioNTech bivalent were below the inclusion threshold of 200 for this study. Follow up studies to detect possible unknown manufacturing contaminants $$\left(M_{k}^{X} \right)$$ may be warranted.
4.5. Hepatitis A and B Vaccines
Safety signals for Hep A (Havrix) were observed for 3 autoimmune AEs, Hep B (Engerix-B) with 7 autoimmune AEs, Hep B (Recombivax Hb) with 6 autoimmune AEs, and Hep A + Hep B (Twinrix) with 11 autoimmune AEs. Combining both Hep A and Hep B into one vaccine may result in increased non-specific induction of autoimmune AEFIs.
4.6. Human Papillomavirus (HPV) Vaccines
Safety signals for HPV (Cervarix) were observed for 14 autoimmune AEs including Arthritis at 1823 (
p < 0.00001), Chronic fatigue at 1569 (
p < 0.00001), GBS at 1251 (
p < 0.00001), POTS at 1229 (
p < 0.00001), CRPS at 1060 (
p < 0.00001), and Systemic lupus erythematosus at 911 (
p < 0.00001) all per 100,000 VAERS reports. Safety signals for HPV (Gardasil) were observed for 6 autoimmune AEs, including POTS at 1223 (
p < 0.00001). Safety signals for HPV (Gardasil 9) were observed for 2 autoimmune AEs: Henoch-Schönlein purpura (257,
p < 0.00001) and POTS (472,
p < 0.00001). HPV (Cervarix) uses a baculovirus expression system, and HPV (Gardasil) and HPV (Gardasil 9) do not; the only common components are HPV type 16 L1 capsid protein and HPV type 18 L1 capsid protein, aluminum, and sodium chloride. The most likely causative component(s) include the HPV type 16 L1 and type 18 L1 proteins, and/or unknown manufacturing contaminants $$\left( M_{k}^{X} \right)$$. HPV (Cervarix) includes ASO4 adjuvant (Toll-like receptor 4, TLR4, agonist 3-O-desacyl-4′-monophosphoryl lipid A (MPL) with aluminum salt) but HPV (Gardasil) and HPV (Gardasil 9) do not; it is possible that the inclusion of the ASO4 adjuvant in HPV (Cervarix) contributes to the increased number of autoimmune AE associations detected (
).
4.7. Study Limitations
This is an exploratory study examining possible autoimmune AEs safety signals following immunization. AEFIs can represent background AEs plus possible vaccine associated AEs. The evidence herein identifies candidate safety signals and does not establish causality for possible vaccine associated AEs. Based on the observed patterns of safety signals across all vaccines, possible follow-up areas for confirmation and future studies are suggested. Data and results from VAERS can identify new safety signals but do not confirm diagnoses or establish biological plausibility.
This retrospective study identifies multiple autoimmune AE safety signals linked to specific vaccines and coadministered vaccines. For detected non-specific associations, decreasing the level of immune stimulation may reduce these autoimmune AEs while still stimulating desired immune responses. Follow-up studies examining possible manufacturing contaminants linked to a subset of the identified autoimmune safety signals are warranted. For specific autoimmune AE safety signals detected, removal/substituting causative peptides, antigens, or causative component(s) will likely reduce the autoimmune AE safety signals with minimal impact on vaccine efficacy.
D.O.R.: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. The author has read and approved the submitted version.
Not applicable.
Not applicable.
Data available at Ricke, Darrell, 2025, “Autoimmune Adverse Events Following Immunization”, https://doi.org/10.7910/DVN/RE23RJ, Harvard Dataverse, V2.
This research received no external funding.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.