Post-COVID SARS-CoV-2 Antigen Persistence: A Critical Review of Mass Spectrometry Methodology and the Confound of Vaccine-Derived Antigens

Post-COVID SARS-CoV-2 Antigen Persistence: A Critical Review of Mass Spectrometry Methodology and the Confound of Vaccine-Derived Antigens

Received: 06 May 2026 Revised: 26 May 2026 Accepted: 15 June 2026 Published: 29 June 2026

© 2026 The authors. This is an open access article under the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
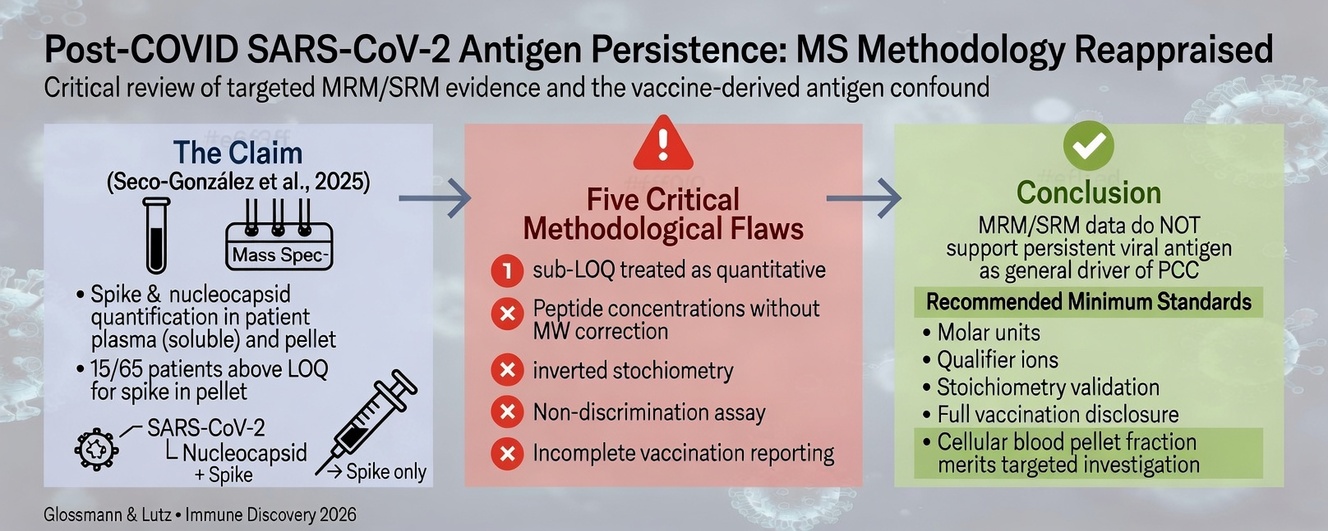
Graphical Abstract
1. Introduction
Post-COVID condition (PCC), or long COVID, affects an estimated 10–20% of individuals following SARS-CoV-2 infection and is characterised by persistent or relapsing symptoms including fatigue, cognitive impairment, dyspnoea, and autonomic dysfunction lasting beyond 12 weeks from acute onset [1,2,3]. Among proposed mechanisms, the persistence of viral antigens—particularly spike proteins—in blood and tissues has attracted considerable attention as a potential driver of ongoing immune activation and inflammation. The hypothesis is biologically plausible: spike protein binds ACE2 receptors, disrupts endothelial function, alters the renin-angiotensin-aldosterone system, and triggers cytokine production, similar to endotoxin. Spike persistence beyond acute infection has been reported by independent platforms, including ELISA, single-molecule array (Simoa), and immunohistochemistry [4,5,6,7], lending biological plausibility to the broader hypothesis even though the MS evidence evaluated here falls short. On the other hand, a persistent spike has been observed in circulating monocytes of patients with similar symptoms (post Vacc), many months after vaccination with no evidence of a previous COVID infection [8]. Clearly, there is an obvious need to identify the culprit (viral or vaccinal origin) unambiguously.
Targeted mass spectrometry—specifically multiple reaction monitoring (MRM) and selected reaction monitoring (SRM)—offers high molecular specificity and has been applied to SARS-CoV-2 antigen quantification in clinical specimens. A comprehensive compilation of prior targeted LC-MS/MS studies identified 16 publications, of which only seven used genuine clinical human specimens (plasma or nasopharyngeal swabs from patients). These seven studies differ importantly in their analytical scope and specimen type. Three groups focused exclusively on NCP in swab matrices using highly sensitive immunocapture workflows: Bezstarosti et al. achieved detection in the mid-attomole range [9], Cardozo et al. validated an automated, high-throughput NCP assay across 985 clinical swabs (attomol–fmol range,) [10], and Rajczewski et al. systematically evaluated peptide target suitability for clinical MS diagnostics [11]. Cazares et al. developed a parallel reaction monitoring (PRM) assay targeting both spike and NCP in clinical specimens (fmol range) [12], while Renuse et al. detected NCP—not spike—in nasopharyngeal swabs using immunoaffinity capture at attomole-level sensitivity, and did not measure antigen in blood [13]. Suddhapas et al. extended the field by evaluating variant-specific spike peptides capable of discriminating SARS-CoV-2 variants of concern from clinical samples [14]. Pierce-Ruiz et al. applied isotope dilution MS to quantify both spike and NCP, but in vaccine and recombinant preparations (LOQ ~10 fmol/µL) rather than patient blood; it is a method and standardisation study, not a measurement of antigen in clinical specimens [15].
Critically, vaccination status was not reported in six of these seven studies (only Pierce-Ruiz et al. provides partial early-2021 context [15]. Most focused on diagnostic detection of acute infection rather than long-term antigen persistence in PCC. None used molar units as their primary output, and none employed the K986P/V987P signature peptide to discriminate vaccine-derived from infection-derived spike. These limitations substantially reduce their utility for evaluating persistent viral antigen in vaccinated post-COVID cohorts, and underscore the need for the methodological standards proposed in Section 5.
2. Methodological Requirements for Valid MRM/SRM-Based Protein Quantification
Valid MRM/SRM quantification requires stable-isotope-labelled (SIL) internal standards, light:heavy ratio-based quantification, qualifier-ion monitoring, strict LOQ compliance, and consistent reporting units [16,17,18]. Qualifier ions are a particularly important requirement: The absence of a qualifier ion, as becomes evident from table 2 on page 4 in the article by Seco-González et al. [19], drastically increases the risk of false-positive identification due to co-eluting isobaric interferences and renders the identification analytically unconvincing for strict quantitative purposes.
A particularly consequential issue is the distinction between peptide mass concentration and protein mass concentration. Calibration curves are constructed with synthetic tryptic peptides; the interpolated value therefore, reflects peptide mass (ng/µL). Conversion to intact protein mass requires the molecular-weight correction factor (MWprotein/MWpeptide). For the two spike peptides used by Seco-González et al. (average MW 1154.075 Da) and the full-length spike monomer (MW 141,178 Da), this gives: 141,178/1154.075 ≈ 122-fold. Reporting peptide concentrations directly as “protein concentrations” without this correction therefore underestimates the true protein level by approximately two orders of magnitude—a fundamental error with direct consequences for interpretation.
Virion stoichiometry provides an independent internal validity check: intact SARS-CoV-2 virions contain approximately 300–500 NCP copies and ~24 spike trimers (~72 spike monomers), as determined by cryo-electron tomography [20,21]. This yields a molar NCP:spike ratio of approximately 4–7:1. Any study quantifying both proteins from the same sample should respect this ratio if the detected material derives from residual intact virions. A marked deviation—especially spike >> NCP—points to non-virion sources such as free soluble antigen or vaccine-derived spike. Theoretically, differential clearance of NCP and spike could skew plasma stoichiometry in favour of spike; however, the scale of inversion observed in Seco-González et al. (spike >>> NCP with near-absence of NCP) is far more likely to indicate a non-virion source of spike rather than differential clearance.
3. The Vaccine Discrimination Problem
mRNA vaccines encode a prefusion-stabilised spike protein carrying the K986P/V987P (“2P”) substitutions. These mutations remove a tryptic cleavage site and produce a detectable mass shift in tryptic peptides spanning residues 980–1000. The two peptides targeted by Seco-González et al. (GIYQTSNFR and GWIFGTTLDSK) lie outside this region and are identical in wild-type and vaccine-encoded spike, rendering the assay completely unable to discriminate the two sources. NCP, which is absent from all approved vaccines, therefore serves as an unambiguous infection-derived control in vaccinated cohorts.
Brogna et al. reported detection of a “PP-spike fragment” consistent with the K986P/V987P substitution signature in blood samples on Guthrie cards from healthy vaccinated individuals [22]. However, several important limitations constrain the interpretation of that study: the cohort comprised exclusively “healthy” vaccinated individuals, with no unvaccinated or infected comparators; the analytical methods were not fully disclosed; and the data were presented only graphically, without descriptive statistics, making independent quantitative evaluation impossible. The study therefore, establishes the detection of a spike-related signal in vaccinated individuals but does not constitute rigorous evidence of the K986P/V987P peptide as a validated diagnostic marker of vaccine-derived spike. Moreover, it should be noted that the proteotypic peptide containing the K986P/V987P mutations is relatively hydrophobic, which may create additional difficulties for chromatographic separation and ionisation in standard MRM methods designed for water-soluble tryptic peptides. This challenge must be taken into account during method development (also, see Box 1). A further limitation applies specifically to spike-based discrimination. The 2P substitutions are present in the mRNA vaccines (Comirnaty, Pfizer-BioNTech; Spikevax, Moderna) and in the Ad26-vectored Janssen vaccine, but not in the chimpanzee-adenovirus vaccine Vaxzevria (ChAdOx1, AstraZeneca), which encodes the full-length wild-type spike [23]. In Spain, where the focal cohort was recruited, Comirnaty (~70%), Spikevax (~12%), and Janssen (~3%) together accounted for ~85% of doses administered by the end of August 2021, while Vaxzevria accounted for ~15% [24]. The K986P/V987P signature peptide, therefore, positively identifies vaccine-derived spike in the great majority of vaccinated patients but is blind to AstraZeneca recipients, whose vaccine spike is indistinguishable from infection-derived spike at this locus. Absence of the 2P peptide cannot, by itself, exclude a vaccine origin, which further reinforces nucleocapsid as the only unambiguous infection-derived marker.
Brogna and Cristoni subsequently described a novel absolute quantification method for peptides and metabolites; that paper presents a methodological framework and does not report measurement of the double-proline peptide in any patient or participant cohort [25]. Neither study, therefore, provides the validated, quantitative, patient-level evidence needed to deploy the 2P-spanning peptide as a routine vaccine-discrimination tool in clinical MRM/SRM workflows—though the approach remains a scientifically sound recommendation for future studies that do report such data.
Box 1. The Cellular Blood Compartment: A Neglected Matrix.
Plasma is the default matrix for almost all clinical proteomics, yet both cited studies reporting blood spike used non-plasma fractions—Seco-González et al., the cellular pellet [19], Brogna et al. dried whole-blood spots [22]. Although we have criticised their quantification, the choice of matrix may be more defensible than it first appears. High whole-blood-to-plasma concentration ratios are familiar in pharmacology—chloroquine is the classic case—but have never been examined for spike. There are mechanistic grounds to expect such partitioning: Bansal et al. detected circulating exosomes bearing spike protein for up to four months after mRNA vaccination [26], immunogenic in mice without added adjuvant. The membrane-bound S2 subunit is a plausible persistent moiety. Such vesicles may aggregate (annexin A1-dependent tethering; [27] but more probably associate with the cellular surface, since injected extracellular vesicles and nanoparticles hitchhike on erythrocytes and platelets in the circulation [28]. This would concentrate vaccine-derived spike in the cellular fraction while leaving little in plasma—coherent with the spike-without-nucleocapsid pattern and orthogonal to the quantification flaws discussed above. Notably, Patterson et al. reported S1, potential S1 mutant peptides and S2 peptides in circulating monocytes months after vaccination [8]. We therefore suggest that the cellular blood component, routinely discarded, warrants direct investigation in the context of spike persistence and PCC.
4. Critical Analysis of the Focal Study by Seco-González
The MRM/SRM component of Seco-González et al. reports “Spike protein” and “Nucleocapsid protein” concentrations (ng/µL) in plasma and pellet fractions from 65 PCC patients and 3 uninfected controls (their table S9) [19]. The authors used two proteotypic peptides for each target protein (GIYQTSNFR and GWIFGTTLDSK for spike; GFYAEGSR and DGIIVVATEGALNTPK for nucleocapsid) together with their corresponding 13C/15N-labelled stable-isotope analogues. Throughout, we use the suffix P to denote the cellular pellet and S the soluble (supernatant) fraction, as established by the antigen distributions in their figure S9; the table S9 caption transposes these labels. Table 1 below summarises the five methodological flaws identified in the following sub-sections.
Table 1. Summary of methodological flaws in the 2025 article by Seco-González et al. and their consequences. Section references are given in parentheses.
|
Flaw |
Evidence |
Consequence |
|---|---|---|
|
Sub-LOQ values treated as quantitative data (4.1) |
The stated LOQ is ~7.9 ng/μL. 100% of soluble (plasma) samples and 77% of pellet samples are Sub-LOQ. Sub-LOQ data are not processed statistically but are presented as quantitative. |
Data are scientifically uninterpretable as protein concentrations |
|
Peptide concentrations reported as protein concentrations (4.2) |
Calibration curves use synthetic tryptic peptides; no MW correction (×122) applied |
Actual spike protein concentrations, if real, would be ~964–>2100 ng/µL—physiologically implausible |
|
Stoichiometric inversion (4.3) |
NCP:spike molar ratio strongly inverted vs. expected virion ratio of ≈4–7:1 [21] |
Signal is incompatible with intact residual virions; consistent with non-virion spike source |
|
Assay blind to vaccine-derived spike (4.4) |
Target peptides (GIYQTSNFR, GWIFGTTLDSK) lie outside the K986P/V987P region; ~77% of cohort vaccinated |
Cannot distinguish infection-derived from vaccine-derived spike signal |
|
Vaccination reporting is incomplete and inconsistent (4.5) |
2024 paper (same cohort) gives no vaccination data; 2025 supplement reports it inconsistently (table S1 vs. figure S9) |
Prevents readers from identifying vaccine-derived spike as a confound |
4.1. Sub-LOQ Measurements Reported as Quantitative Data
The authors state peptide LOQs of ~7.91–7.95 ng/µL (spike) and ~7.96–8.08 ng/µL (NCP) in human plasma matrix. Inspection of table S9 reveals the following:
- ●
-
Pellet spike (SPIKE_P): only 15 patients (23%) have concentrations ≥ 7.9 ng/µL (3 asymptomatic + 12 symptomatic).
- ●
-
Pellet nucleocapsid (NCAP_P): zero patients reach ≥ 7.9 ng/µL (maximum observed = 7.172 ng/µL).
All plasma values and the large majority of pellet values fall far below the stated peptide LOQ. If the numbers represent true “protein” concentrations—as stated in the paper, figures, and conclusions—then every measurement is below the authors’ own validated LOQ and is therefore scientifically uninterpretable as quantitative data.
4.2. Raw Peptide Concentrations Reported as Protein Concentrations
Independent of the peptide-versus-protein interpretation set out below, the reported concentrations are irreconcilable with the entire validated literature on circulating SARS-CoV-2 antigen. Taken at face value and uncorrected, the 15 above-LOQ pellet spike values (≈8–18 ng/µL, i.e., 8000–18,000 ng/mL) exceed every prior measurement of circulating spike by three to five orders of magnitude, and were obtained without any analyte-enrichment step. In fact, no targeted-MS study has quantified free spike protein in human blood at all: the existing MS antigen literature comprises nucleocapsid detection in respiratory specimens (e.g., Renuse et al. [13] and spike/nucleocapsid quantification in vaccine or recombinant preparations (e.g., Pierce-Ruiz et al. [15], not free antigen in plasma or serum. Ultrasensitive single-molecule arrays (Simoa), the most sensitive platform available, detect free spike in the low picogram-per-millilitre range (assay LOD ≈ 5 pg/mL), rising to at most ~1 ng/mL even in severe acute infection [4,29]. Even the most advanced affinity-capture front end yet reported—an engineered pentameric ACE2 receptor coupled to MS [30]—achieved quantitative spike recovery only from saliva spiked with recombinant protein, never from clinical blood. No analytical mechanism is offered for how an unenriched MRM/SRM workflow could detect free antigen at a thousand- to hundred-thousand-fold the demonstrated ceiling of methods purpose-built, with enrichment, for exactly this task; after the molecular-weight correction omitted by the authors (see below), the discrepancy widens further still.
The calibration curves were constructed with synthetic tryptic peptides. The reported ng/µL values therefore represent peptide mass concentrations, not protein mass concentrations. Applying the correct molecular-weight correction (×122; see Section 2) transforms the 15 above-LOQ pellet spike values: the minimum above-LOQ value of ~7.9 ng/µL peptide corresponds to ~964 ng/µL spike protein, and the highest reported values (≈17.8 ng/µL) correspond to >2100 ng/µL. Concentrations in this range would be physiologically implausible for a circulating protein in plasma and are inconsistent with any known biological model of antigen persistence. This arithmetic alone demonstrates that the values cannot represent the intact spike protein.
4.3. Stoichiometric Inconsistency
In the pellet fraction, the NCP: spike molar ratio is strongly inverted (spike >> NCP), opposite to the expected ratio of approximately 4–7:1 that would be expected from intact residual virions. This stoichiometric inversion is incompatible with the hypothesis that the detected material represents residual intact virions, and is exactly what would be predicted if vaccine-derived spike, which is produced independently of any NCP, contributed substantially to the signal while NCP reflected only infection-derived antigen.
4.4. Failure to Discriminate Vaccine-Derived from Infection-Derived Spike
The cohort was predominantly vaccinated: figure S9 (by visual inspection) of Seco-González et al. shows that 50 of 65 patients (77%) had received at least one mRNA vaccine dose at the time of blood collection, with only 15 in the unvaccinated (“None”) subgroup [19]. We note an internal inconsistency in the source: supplementary table S1 records the mirror-image figures—50 unvaccinated and 15 vaccinated—so the supplement contradicts itself on this primary variable (Section 4.5). Notably, the vaccine confound is evident from the authors’ own supplementary data (table S9 and figure S9) without any further analysis: 13 of the 15 above-LOQ pellet-spike values occur in vaccinated patients—an above-LOQ rate twice that of the unvaccinated subgroup (26% vs. 13%), in a cohort that is itself 77% vaccinated—while nucleocapsid is essentially absent and the NCP: spike stoichiometry is inverted relative to intact virions. Because the two assay peptides lie outside the K986P/V987P region (Section 3) and are identical in wild-type and vaccine-encoded spike, the method cannot attribute this signal to infection rather than vaccination. A vaccine-enriched, nucleocapsid-poor, stoichiometrically inverted spike signal, measured by an assay blind to the vaccine signature, points to a substantial vaccine-derived contribution that the study design cannot exclude.
4.5. Transparency and Consistency of Vaccination Reporting
It is noteworthy that in the 2024 publication from the same group [31], vaccination status was not disclosed, even though, according to data from the subsequent 2025 paper [19], it was known to the authors. As a result, readers are unable to recognise vaccine-derived spike as a potential confound. This is not a minor omission: in a cohort where 77% of participants were vaccinated, vaccination status is a primary variable for interpreting any spike signal.
5. Recommendations for Future MRM/SRM Studies of SARS-CoV-2 Antigen Persistence
We propose the following minimum methodological standards for future MRM/SRM studies in this area:
- ●
-
Report in molar units (fmol/µL or pmol/mL) rather than mass concentration, to enable cross-study comparison and stoichiometric verification.
- ●
-
Comply strictly with validated LOQ thresholds; exclude sub-LOQ values from quantitative statistics and clearly label them as below the limit of quantification.
- ●
-
Monitor at least one qualifier ion per peptide in addition to the primary quantifier transition. Without a confirmed qualifier ion ratio, a signal cannot be distinguished from co-eluting isobaric interferents.
- ●
-
Use either a synthetic peptide with an extended sequence (for proteolysis) or, at a minimum, confirm the sequence of the target peptide in the sample using PRM (Parallel Reaction Monitoring) and comparison of spectral similarity (library match score) to a synthetic standard.
- ●
-
Use light: heavy SIL ratios for quantification, not absolute signal intensity.
- ●
-
Include the K986P/V987P signature peptide (spanning residues ~980–1000 of spike, which carries a diagnostic mass shift absent from all wild-type SARS-CoV-2 sequences) for vaccine discrimination in any cohort that includes vaccinated individuals.
- ●
-
Report the measured NCP: spike molar ratio and compare it explicitly against the expected virion ratio (~4–7:1) as an internal stoichiometric validity check.
Disclose vaccination status—including number of doses, vaccine product and platform, and interval since last dose—in all cohort studies reporting spike antigen detection. Vaccine platform is decisive: the 2P-stabilised spike of the mRNA (Comirnaty, Spikevax) and Ad26 (Janssen) vaccines is distinguishable by the K986P/V987P peptide, whereas ChAdOx1/AstraZeneca encodes wild-type spike [23] that is indistinguishable from infection-derived spike at that locus.
6. Conclusions
On the basis of an evaluation of seven MRM/SRM studies using genuine clinical specimens, we conducted an in-depth analysis of the focal paper published by Seco-González et al. [31]. The MRM/SRM data in that paper do not support the claim that persistent viral SARS-CoV-2 antigens are a general pathophysiological driver of PCC. The reported values are either physically impossible if interpreted as intact protein concentrations or, if interpreted as peptide concentrations, would have required a ~122-fold correction (that was not applied). Put differently, consider the exemplary synthetic peptide A with a molecular weight of 1154 Da that calibrates the signal. If the authors report a protein concentration of 10 ng/μL, they have actually measured 10 ng/μL of peptide. To obtain the intact protein concentration (MW 141,178 Da), one must multiply by ~122, yielding 1220 ng/μL—comparable to the total plasma protein concentration. Consequently, the measured value cannot represent an intact protein.
After correction, the implied spike protein concentrations are physiologically implausible. Nucleocapsid is essentially undetectable. Consequently, the measured signal cannot be interpreted as intact viral protein at the reported concentrations; its source (spike, cross-reacting proteins, sample preparation artefact) cannot be determined from the presented data. However, the stoichiometric inversion and the concentration of measurable spike signal among vaccinated individuals point to vaccine-derived rather than infection-derived antigen.
The broader antigen-persistence hypothesis remains biologically plausible and is supported by independent measurement platforms, including ELISA, Simoa, and immunohistochemistry. However, credible MRM/SRM evidence requires molar-unit reporting, strict LOQ compliance, qualifier-ion monitoring, vaccine-discrimination peptides spanning the K986P/V987P region, stoichiometric NCP: spike cross-validation, and transparent disclosure of vaccination status. Adoption of these standards is both necessary and feasible given the existing methodology in the field.
Taken together, the analytical inconsistencies (sub-LOQ values, molecular weight error, violation of stoichiometry) do not allow the presented data to be regarded as reliable evidence for quantitative detection of SARS-CoV-2 antigens. Although a vaccine origin of the signal is the most plausible explanation for the observed picture, a categorical statement to that effect requires separate analytical confirmation.
Statement of the Use of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the authors used Claude (Anthropic) to assist with literature search, reference verification, and manuscript editing. After using this tool, the authors reviewed and edited all content and take full responsibility for the content of the published article.
Author Contributions
Conceptualization, H.H.G.; Methodology, H.H.G. & O.M.D.L.; Formal Analysis, H.H.G. & O.M.D.L.; Investigation, H.H.G. & O.M.D.L.; Data Curation, H.H.G.; Writing—Original Draft Preparation, H.H.G. & O.M.D.L.; Writing—Review & Editing, H.H.G. & O.M.D.L.
Ethics Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Funding
No external funding was received for this work.
Declaration of Competing Interest
The authors declare no conflict of interest.
References
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. DOI:10.1038/s41579-022-00846-2 [Google Scholar]
- Ely EW, Brown LM, Fineberg HV. Long COVID. N. Engl. J. Med. 2024, 390, 2097–2108. DOI: 10.1056/NEJMsb2408466 [Google Scholar]
- Parotto M, Gyöngyösi M, Howe K, Myatra SN, Ranzani O, Shankar-Hari M, et al. Post-Acute Sequelae of COVID-19: Understanding and addressing the burden of multisystem manifestations. Lancet Respir. Med. 2023, 11, 739–754. DOI:10.1016/S2213-2600(23)00239-4 [Google Scholar]
- Swank Z, Senussi Y, Manickas-Hill Z, Yu XG, Li JZ, Alter G, et al. Persistent circulating severe acute respiratory syndrome coronavirus 2 spike is associated with post-acute coronavirus disease 2019 sequelae. Clin. Infect. Dis. 2023, 76, E487–E490. DOI:10.1093/cid/ciac722 [Google Scholar]
- Craddock V, Mahajan A, Spikes L, Krishnamachary B, Ram AK, Kumar A, et al. Persistent circulation of soluble and extracellular vesicle-linked spike protein in individuals with postacute sequelae of COVID-19. J. Med. Virol. 2023, 95, e28568. DOI:10.1002/jmv.28568 [Google Scholar]
- Peluso MJ, Swank ZN, Goldberg SA, Lu S, Dalhuisen T, Borberg E, et al. Plasma-based antigen persistence in the post-acute phase of COVID-19. Lancet Infect. Dis. 2024, 24, E345–E347. DOI:10.1016/S1473-3099(24)00211-1 [Google Scholar]
- Arostegui D, Castro K, Schwarz S, Vaidy K, Rabinowitz S, Wallach T. Persistent SARS-CoV-2 nucleocapsid protein presence in the intestinal epithelium of a pediatric patient 3 months after acute infection. JPGN Rep. 2022, 3, e152. DOI:10.1097/pg9.0000000000000152 [Google Scholar]
- Patterson BK, Yogendra R, Francisco EB, Guevara-Coto J, Long E, Pise A, et al. Detection of S1 spike protein in CD16+ monocytes up to 245 days in SARS-CoV-2-negative post-COVID-19 vaccine syndrome (PCVS) individuals. Hum. Vaccines Immunother. 2025, 21, 2494934. DOI:10.1080/21645515.2025.2494934 [Google Scholar]
- Bezstarosti K, Lamers MM, Doff WAS, Wever PC, Thai KTD, van Kampen JJA, et al. Targeted proteomics as a tool to detect SARS-CoV-2 proteins in clinical specimens. PLoS ONE 2021, 16, e0259165. DOI:10.1371/journal.pone.0259165 [Google Scholar]
- Cardozo KHM, Lebkuchen A, Okai GG, Schuch RA, Viana LG, Olive AN, et al. Establishing a mass spectrometry-based system for rapid detection of SARS-CoV-2 in large clinical sample cohorts. Nat. Commun. 2020, 11, 6201. DOI:10.1038/s41467-020-19925-0 [Google Scholar]
- Rajczewski AT, Mehta S, Nguyen DDA, Grüning B, Johnson JE, McGowan T, et al. A rigorous evaluation of optimal peptide targets for MS-based clinical diagnostics of Coronavirus Disease 2019 (COVID-19). Clin. Proteom. 2021, 18, 15. DOI:10.1186/s12014-021-09321-1 [Google Scholar]
- Cazares LH, Chaerkady R, Samuel Weng SH, Boo CC, Cimbro R, Hsu HE, et al. Development of a Parallel Reaction Monitoring Mass Spectrometry Assay for the Detection of SARS-CoV-2 Spike Glycoprotein and Nucleoprotein. Anal. Chem. 2020, 92, 13813–13821. DOI:10.1021/acs.analchem.0c02288 [Google Scholar]
- Renuse S, Vanderboom PM, Maus AD, Kemp JV, Gurtner KM, Madugundu AK, et al. A Mass Spectrometry-Based Targeted Assay for Detection of SARS-CoV-2 Antigen from Clinical Specimens. EBioMedicine 2021, 69, 103465. DOI:10.1016/j.ebiom.2021.103465 [Google Scholar]
- Suddhapas K, Choi MH, Shortreed MR, Timperman A. Evaluation of Variant-Specific Peptides for Detection of SARS-CoV-2 Variants of Concern. J. Proteome Res. 2022, 21, 2443–2452. DOI:10.1021/acs.jproteome.2c00325 [Google Scholar]
- Pierce-Ruiz C, Santana WI, Sutton WJH, Fischler DA, Cooper HC, Marc LR, et al. Quantification of SARS-CoV-2 spike and nucleocapsid proteins using isotope dilution tandem mass spectrometry. Vaccine 2021, 39, 5106–5115. DOI:10.1016/j.vaccine.2021.07.066 [Google Scholar]
- Gallien S, Duriez E, Domon B. Selected reaction monitoring applied to proteomics. J. Mass Spectrom. 2011, 46, 298–312. DOI:10.1002/jms.1895 [Google Scholar]
- Carr SA, Abbatiello SE, Ackermann BL, Borchers C, Domon B, Deutsch EW, et al. Targeted peptide measurements in biology and medicine: best practices for mass spectrometry-based assay development using a fit-for-purpose approach. Mol. Cell Proteom. 2014, 13, 907–917. DOI:10.1074/mcp.M113.036095 [Google Scholar]
- van den Broek I, Mastali M, Mouapi K, Bystrom C, Bairey Merz CN, Van Eyk JE. Quality control and outlier detection of targeted mass spectrometry data from multiplex protein panels. J. Proteome Res. 2020, 19, 2278–2293. DOI:10.1021/acs.jproteome.9b00854 [Google Scholar]
- Seco-Gonzalez A, Antelo-Riveiro P, Bravo SB, Domínguez-Santalla MJ, Rodríguez-Ruiz E, Piñeiro Á, et al. Comprehensive molecular characterization of post-COVID condition: Immunoglobulin suppression and persistent SARS-CoV-2 antigens as key pathophysiological drivers. J. Infect. Public Health 2025, 18, 102870. DOI:10.1016/j.jiph.2025.102870 [Google Scholar]
- Wrapp D, Wang N, Corbett KS, Goldsmith JA, Hsieh CL, Abiona O, et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. DOI:10.1126/science.abb2507 [Google Scholar]
- Ke Z, Oton J, Qu K, Cortese M, Zila V, McKeane L, et al. Structures and distributions of SARS-CoV-2 spike proteins on intact virions. Nature 2020, 588, 498–502. DOI:10.1038/s41586-020-2665-2 [Google Scholar]
- Brogna C, Cristoni S, Marino G, Montano L, Viduto V, Fabrowski M, et al. Detection of recombinant spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms. Proteom. Clin. Appl. 2023, 17, e2300048. DOI:10.1002/prca.202300048 [Google Scholar]
- Heinz FX, Stiasny K. Distinguishing features of current COVID-19 vaccines: knowns and unknowns of antigen presentation and modes of action. NPJ Vaccines 2021, 6, 104. DOI:10.1038/s41541-021-00369-6 [Google Scholar]
- Giesen C, Saa-Requejo C, Lopez-Carrillo I, Ortega-Torres A, García-Fernández C. Risks of adverse outcomes in COVID-19 patients and vaccination status in a secondary hospital in Spain. Vacunas 2022, 23, S32–S35. DOI:10.1016/j.vacune.2022.10.013 [Google Scholar]
- Brogna C, Cristoni S. A new absolute quantitative method for peptide and metabolite detection. J. Mass Spectrom. 2024, 59, e4991. DOI:10.1002/jms.4991 [Google Scholar]
- Bansal S, Perincheri S, Fleming T, Poulson C, Tiffany B, Bremner RM, et al. Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer-BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines. J Immunol. 2021, 207, 2405–2410. DOI:10.4049/jimmunol.2100637 [Google Scholar]
- Rogers MA, Buffolo F, Schlotter F, Atkins SK, Lee LH, Halu A, et al. Annexin A1–dependent tethering promotes extracellular vesicle aggregation revealed with single–extracellular vesicle analysis. Sci. Adv. 2020, 6, eabb1244. DOI:10.1126/sciadv.abb1244 [Google Scholar]
- Pavlova S, Mamand DR, Hagey DW, Liang X, Estupiñán HY, Zheng W, et al. Injected extracellular vesicles and other nanoparticles hitchhike on erythrocytes and platelets from circulation towards organ clearance. Extracell. Vesicle 2026, 7, 100103. DOI:10.1016/j.vesic.2025.100103 [Google Scholar]
- Ogata AF, Maley AM, Wu C, Gilboa T, Norman M, Lazarovits R, et al. Ultra-sensitive serial profiling of SARS-CoV-2 antigens and antibodies in plasma to understand disease progression in COVID-19 patients with severe disease. Clin. Chem. 2020, 66, 1562–1572. DOI:10.1093/clinchem/hvaa213 [Google Scholar]
- Bate N, Lane D, Evans SE, Salim F, Allcock NS, Haigh R, et al. Engineered Receptor Capture Combined with Mass Spectrometry Enables High-Throughput Detection and Quantitation of SARS-CoV-2 Spike Protein. JACS Au 2025, 5, 747–755. DOI:10.1021/jacsau.4c00980 [Google Scholar]
- Seco-González A, Antelo-Riveiro P, Bravo SB, Garrido PF, Domínguez-Santalla MJ, Rodríguez-Ruiz E, et al. Proteomic analysis of post-COVID condition: Insights from plasma and pellet blood fractions. J. Infect. Public Health 2024, 17, 102571. DOI:10.1016/j.jiph.2024.102571 [Google Scholar]