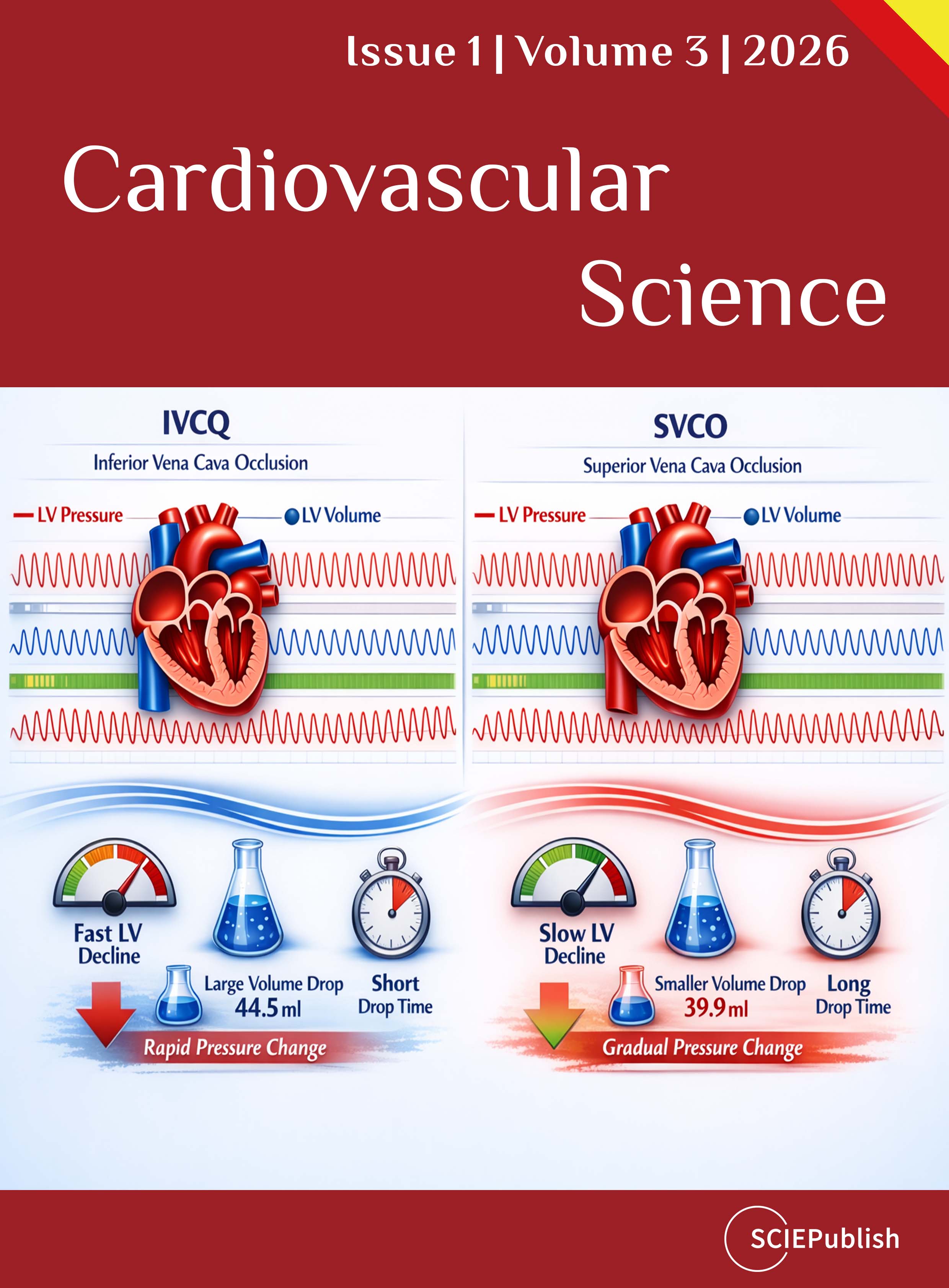
Heart failure (HF) is marked by impaired ventricular function, neurohormonal activation, and volume overload. While therapies target remodeling and neurohormonal pathways, preload management remains pivotal for symptom relief and preventing decompensation. Pressure–volume (PV) loop analysis enables precise characterization of cardiac performance during acute loading changes. To define the differential hemodynamic impact of transient inferior vena cava occlusion (IVCO) versus superior vena cava occlusion (SVCO) using PV loop analysis in a large-animal model. Controlled IVCO and SVCO were performed in healthy animals to reduce preload. PV-derived indices included stroke volume (SV), cardiac output (CO), end-systolic elastance (Ees), volume-axis intercept (V₀), and preload recruitable stroke work (PRSW). IVCO, removing ~70% of venous return, produced a marked leftward PV loop shift, decreased SV and CO, and a near-zero V₀, consistent with near-complete ventricular unloading. The end-systolic pressure–volume relationship steepened, suggesting an acute compensatory inotropic response, though Ees remained unchanged, indicating preserved intrinsic contractility. In contrast, SVCO (~30% venous return) caused only modest PV loop shifts, with preserved end-diastolic volume and stable or slightly rightward V₀. Across both interventions, preload, not intrinsic contractility, accounted for changes in mechanical work and PRSW. IVCO and SVCO elicit distinct preload-dependent hemodynamic profiles. Interpretation of PV loop–derived metrics must account for dynamic loading conditions. These findings provide mechanistic insight into acute volume regulation and warrant validation in HF-specific models to inform decongestive management strategies.

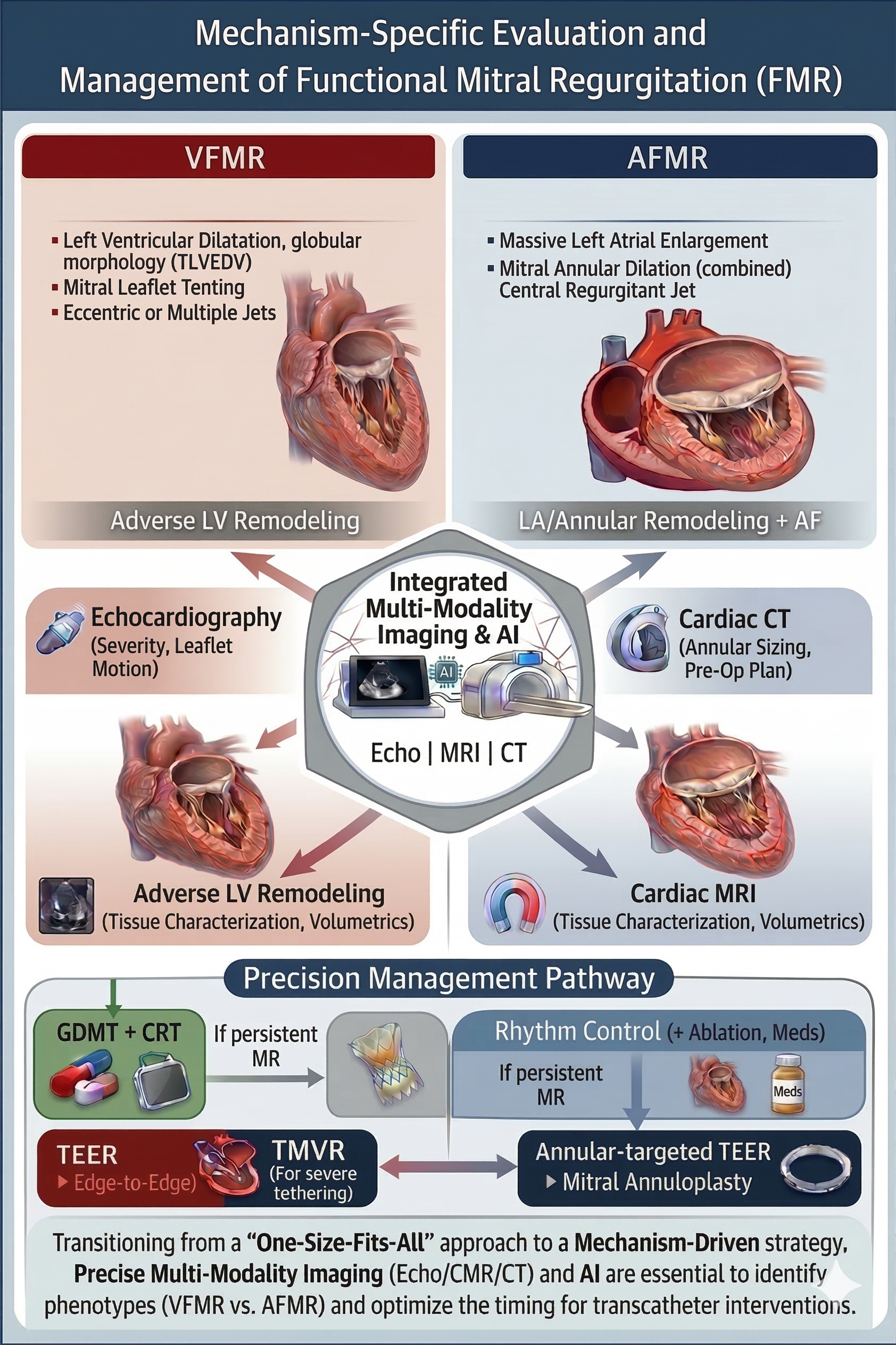
Functional mitral regurgitation (FMR) is a prevalent valvular disorder driven by adverse remodeling of the left ventricle and/or left atrium. This review synthesizes the contemporary evidence on multimodality imaging and its role in mechanism-specific evaluation and management of FMR, with particular emphasis on distinguishing ventricular FMR (VFMR) from atrial FMR (AFMR). FMR is mechanistically heterogeneous, requiring precise phenotyping to guide therapy. A mechanism-based framework differentiating VFMR, driven by left ventricular dilation and leaflet tethering, from AFMR, driven by left atrial and annular enlargement with preserved ventricular function, is central to contemporary management. Echocardiography remains the cornerstone for real-time assessment of MR severity, hemodynamics, and valve–ventricle interactions. Cardiac magnetic resonance (CMR) provides the gold standard for volumetric quantification and myocardial tissue characterization, enabling improved risk stratification by assessing ventricular remodeling and fibrosis. Computed tomography (CT) offers high-resolution anatomic phenotyping and is essential for procedural planning, particularly for transcatheter edge-to-edge repair (TEER) and transcatheter mitral valve replacement (TMVR). Integration of multimodality imaging supports individualized selection between guideline-directed medical therapy alone, TEER, surgical intervention, or TMVR, based on the dominant mechanism and myocardial substrate. The discordant outcomes of landmark trials such as MITRA-FR and COAPT have underscored the importance of precision in patient selection, highlighting the controversial but clinically relevant proportionate/disproportionate FMR framework and the extent of myocardial fibrosis as key modifiers of treatment response. Emerging advances in advanced imaging and artificial intelligence hold promise for automated phenotyping, improved reproducibility, and earlier identification of patients most likely to benefit from intervention, ultimately enabling a more personalized, mechanism-driven approach to improving outcomes in FMR.