A Medical Review of Human Injuries from Unidentified Aerial Phenomena

A Medical Review of Human Injuries from Unidentified Aerial Phenomena
Guodong Qin
1
Pengfei Zhao
2,*

Received: 24 January 2026 Revised: 09 March 2026 Accepted: 25 March 2026 Published: 07 April 2026

© 2026 The authors. This is an open access article under the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
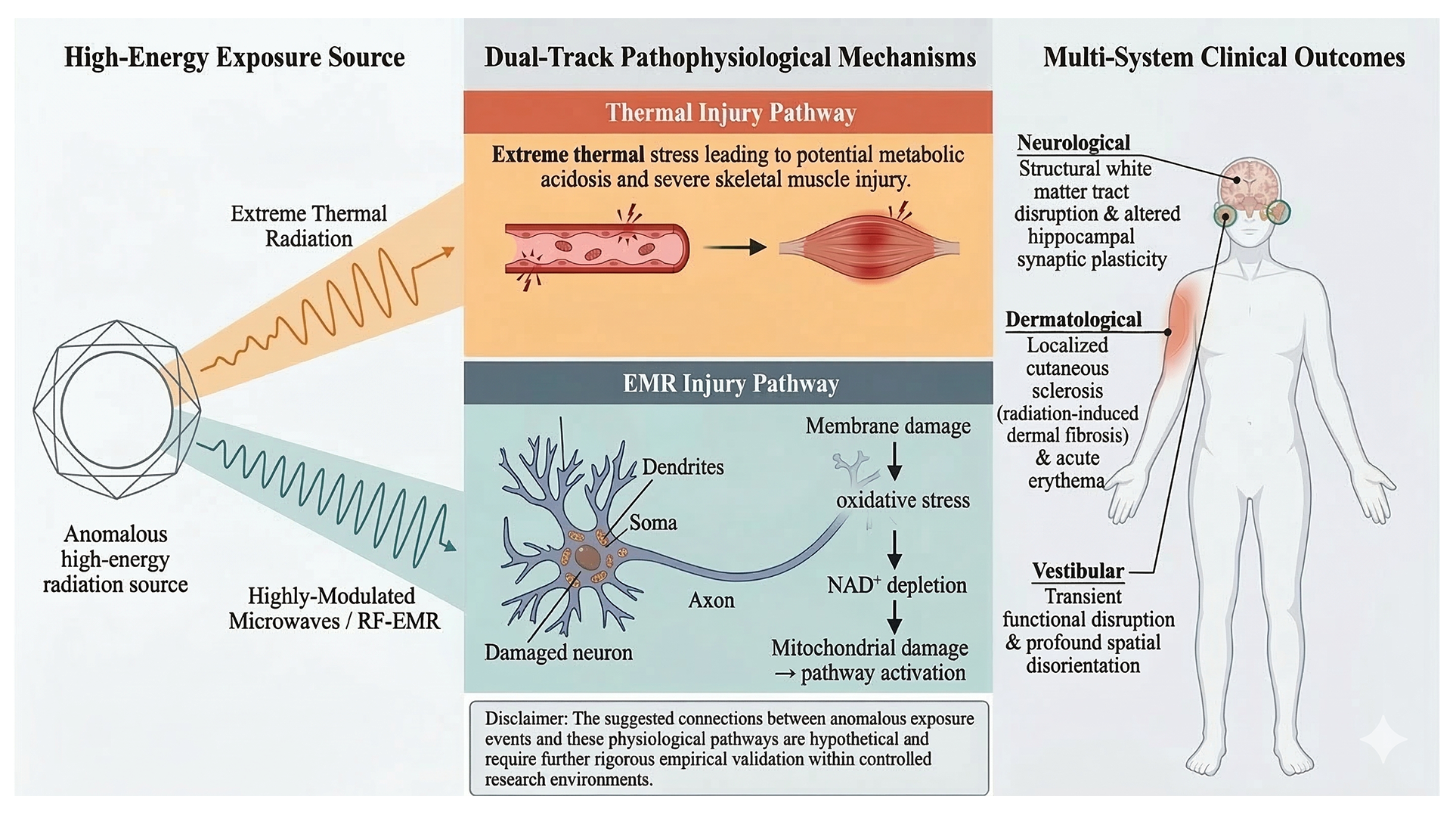
Graphical Abstract
1. Introduction
The term Unidentified Aerial Phenomena (UAP) encompasses airborne objects or events that defy immediate identification by current sensor technologies or conventional meteorological explanations. This term was formally adopted by the U.S. military in recent years, gradually replacing the traditional concept of “Unidentified Flying Objects” (UFOs) [1]. With growing attention from governments worldwide, research has shifted from mere sighting reports to multidisciplinary scientific studies, with the impact of UAPs on human health becoming an increasingly critical focus.
The establishment of the Unidentified Aerial Phenomena Task Force (UAPTF) in 2020 and its successor, the All-domain Anomaly Resolution Office (AARO) in 2022, alongside comprehensive reports from the Office of the Director of National Intelligence (ODNI), has provided a more reliable data foundation for UAP research [2,3]. From a medical perspective, investigating these impacts holds significant practical importance [4]. Military personnel and aviation professionals face occupational health issues directly related to national security, while health concerns arising among the general public require scientific explanation and intervention.
This article systematically reviews the existing medical evidence regarding UAP-related injuries. By integrating declassified documents, medical evaluations, and analogous radiobiology studies [5], this article seeks to provide a comprehensive academic reference for medical researchers, highlight current limitations, and propose future research directions to advance the scientific standardization of this emerging field.
2. Clinical Case Reports of UAP-Induced Human Injuries
2.1. Case Selection Criteria and Traceability
To ensure scientific validity and address the sporadic nature of available data, specific objective criteria were established for this review. As applied to representative historical cases (such as the Cash-Landrum, Rendlesham Forest, and Lonnie Zamora incidents), cases were strictly included based on the following parameters: (1) close-proximity encounters, typically defined as occurring within 150 m; (2) the presence of multiple witnesses exhibiting similar acute clinical symptoms simultaneously, which crucially helps rule out individual psychological or psychosomatic factors; (3) the availability of corroborating physical or environmental trace evidence, such as elevated radiation levels or anomalous damaged vegetation; and (4) a clear temporal correlation between the encounter and the onset of medical symptoms. This review prioritized cases documented in official declassified reports, such as those from the U.S. Defense Intelligence Agency (DIA), and clinical evaluations conducted by recognized medical experts [5].
To address potential selection bias and ensure absolute transparency regarding the clinical origins of the data discussed in this review, we have established a definitive traceability matrix. Table 1 maps the core clinical cases to their primary medical symptoms and, crucially, their original declassified intelligence or official government sources.
Table 1. Core Clinical Cases and Their Original Declassified Intelligence Traceability Mapping.
|
Case Designation (Year) |
Primary Exposed Cohort |
Core Medical Symptoms & Physical Traces |
Declassified Intelligence/Official Source Traceability |
Refs. |
|---|---|---|---|---|
|
Unnamed Military Cohorts (Various) |
Military pilots, Intelligence, & Aerospace personnel |
Structural white matter damage, localized cutaneous sclerosis (erythema/burns), acute neuropsychiatric anomalies. |
U.S. Defense Intelligence Agency (DIA) 2010 Report/Dr. Christopher Green’s clinical evaluations. |
|
|
Cash-Landrum Incident (1980) |
Civilian (Betty Cash, Vickie Landrum, Colby Landrum) |
Acute radiation-like symptoms, severe erythema, blistering, severe hair loss, and potential oncogenesis. |
Verified medical records (Dr. Brian McClellan); cited in DIA 2010 medical pathology assessments. |
|
|
Rendlesham Forest Incident (1980) |
U.S. Military Personnel (USAF) |
Neurological impacts, radiation exposure, and physical trace evidence (elevated localized radiation). |
UK Ministry of Defence (MoD) declassified files; cited within DIA 2010 framework. |
|
|
Lonnie Zamora/Socorro Incident (1964) |
Law Enforcement Personnel |
Thermal effects, physiological shock, verified burned vegetation, and landing traces. |
U.S. Air Force Project Blue Book archives; historical medical evaluations. |
2.2. Health Issues in Military Personnel Encountering UAP Events
Military personnel represent a high-risk cohort for UAP exposure. According to a 2010 research report commissioned by forensic neuroimaging expert Dr. Christopher Green—whose extensive clinical evaluations involved hundreds of patients, primarily including personnel from the CIA, the Department of Defense, special forces, and the aerospace industry—military and intelligence personnel revealed a severe spectrum of acute and subacute field effects [5].
These documented health issues primarily included localized cutaneous sclerosis (radiation-induced dermal fibrosis), severe structural brain injuries (including white matter tract disruption, localized neuroinflammation, and altered blood-brain barrier permeability), and deep tissue thermal injuries. Dr. Green hypothesized that some of these injuries resulted from close-proximity exposure to “subtle, high-power, highly-modulated microwaves”, suggesting that personnel were affected by intense radiofrequency emissions associated with these anomalous objects [5]. Alarmingly, the patient statistics from these evaluations revealed a severe spectrum of acute and subacute field effects, raising significant occupational mortality and morbidity concerns among medical researchers regarding these highly exposed cohorts [5]. To systematically categorize these findings, Table 2 summarizes the major clinical symptoms, underlying UAP-specific pathologies, and epidemiological data observed within these highly exposed military cohorts.
Table 2. Major Clinical Symptoms and UAP-Specific Pathologies in Military Personnel.
|
Symptom Category |
Specific Clinical Manifestations |
UAP-Related Mechanisms & Epidemiological Data |
|---|---|---|
|
Dermatological & Thermal |
Non-ionizing radiation burns, acute erythema, localized cutaneous sclerosis (radiation-induced dermal fibrosis). |
Close-proximity exposure to subtle, high-power, highly-modulated microwaves or RF-EMR associated with the anomalous object. |
|
Neurological |
Close-proximity exposure to subtle, high-power, highly-modulated microwaves or RF-EMR associated with the anomalous object. |
EMR-induced alteration of neuronal membrane potentials and mitochondrial dysfunction. |
|
Systemic & Mortality |
Multisystem inflammatory response, extreme autonomic nervous dysfunction. |
Elevated occupational mortality and severe systemic morbidity concerns post-encounter. |
Note: All clinical manifestations and epidemiological statistics summarized in this table are derived from the evaluations of military personnel conducted by Green [5].
2.3. Detailed Analysis of a Typical UAP Contact Incident
Among numerous UAP contact cases, the incident involving Betty Cash, Vickie Landrum, and 7-year-old Colby Landrum on 29 December 1980, stands out as one of the most representative medical cases. The three individuals encountered a massive diamond-shaped flying object while driving on a highway in Texas. The object hovered in the air, periodically emitting explosive blue flames from its underside, accompanied by intense hot air currents [7]. During the incident, the witnesses were exposed to the object at an estimated close proximity of 40 to 60 m for a sustained duration of approximately 15 to 20 min [7]. Following the exposure, all three individuals began to experience similar acute phase symptoms, including severe nausea, vomiting, diarrhea, fatigue, and redness in their skin and eyes, along with a strong burning sensation.
Betty’s condition progressed to include significant hair loss, tissue fluid exudation (blisters), and severe systemic fatigue [8]. Dr. Brian McClellan, her attending physician, clinically evaluated her symptoms and diagnosed that her condition was highly consistent with environmental radiation exposure [7,8]. Betty was subsequently diagnosed with breast cancer in 1982. While this oncological diagnosis is temporally sequential to the anomalous incident, establishing a definitive causal link to the UAP-associated radiation exposure remains epidemiologically challenging without a larger controlled cohort, highlighting the urgent need for longitudinal follow-up in such anomalous cases [7].
The scientific value of this case lies in the simultaneous onset of identical pathophysiological symptoms among multiple witnesses, strictly correlated with the physical exposure timeline, thereby minimizing the likelihood of isolated psychosomatic origins. Similarly, the 1980 Rendlesham Forest incident and the 1964 Lonnie Zamora case involved military and law enforcement personnel, respectively. During the Zamora incident, the officer chased an unidentified object in his car, leaving behind verifiable physical evidence such as burned vegetation and elevated radiation levels at the site [9,10,11,12].
The common characteristics of these highly credible typical cases are rigorously defined as follows: close-proximity encounters (usually less than 150 m), multiple witnesses exhibiting symptoms simultaneously, the presence of corroborating physical trace evidence, and a clear temporal connection between the symptoms and the UAP encounter. These features provide a reliable clinical foundation for studying the severe health impacts of UAPs on humans.
2.4. Acute and Subacute Clinical Manifestations After UAP Contact
The clinical manifestations of human injury following UAP contact generally present in distinct acute and subacute phases [5]. Acute manifestations typically appear immediately after contact and last for several hours to days, while subacute symptoms emerge days to weeks later. As outlined in Table 3, the acute phase is primarily characterized by immediate thermal damage, cardiovascular stress, and transient neuropsychiatric anomalies. Conversely, Table 4 details the subsequent subacute pathophysiological changes, highlighting the delayed onset of structural neurological damage and severe systemic sequelae.
Table 3. Acute Phase Clinical Manifestations and Physiological Markers Following UAP Exposure.
|
Clinical Manifestation |
Specific UAP-Related Symptoms & Biomarkers |
Defined Mechanism of Occurrence |
Refs. |
|---|---|---|---|
|
Skin/Thermal Damage |
Acute erythema, localized superficial burns, and intense burning sensations; severe cases accompanied by blistering. |
Close-proximity exposure to high-intensity thermal radiation or highly modulated non-ionizing microwaves. |
|
|
Cardiovascular/Systemic |
Compensatory tachycardia, abnormal blood pressure fluctuations, and potential metabolic stress states. |
Sudden surges in metabolic rate induced by extreme thermal stress; acute autonomic nervous dysfunction. |
[16] |
|
Neurological & Neuropsychiatric |
Spatial disorientation, transient confusion; some cases report intense abnormal emotional fluctuations (e.g., acute euphoria). |
Transient abnormal stimulation of the limbic system by extreme electromagnetic pulses. |
[5] |
|
Ophthalmological |
Acute photosensitivity (photophobia), conjunctival hyperemia, and transient blurred vision. |
Direct physical and thermal stimulation of the cornea by intense light sources or RF radiation. |
Table 4. Subacute Phase Pathophysiological Changes Following UAP Exposure.
|
Pathophysiological Domain |
Specific Clinical and Cellular Manifestations |
Underlying UAP-Induced Mechanisms |
Refs. |
|---|---|---|---|
|
Neurological |
Decline in learning/memory abilities persists up to 28 days post-exposure; structural white matter damage. |
Neuronal apoptosis and altered synaptic plasticity in the hippocampus due to EMP radiation. |
|
|
Systemic/Oncological |
Severe hair loss, body swelling, prolonged systemic sequelae, and localized tissue necrosis. |
Long-term high-dose exposure causes severe microcirculatory disorders and deep tissue damage. |
[7] |
Beyond these physical markers, the 2010 report by the U.S. Defense Intelligence Agency documented several unusual subacute phase effects, including severe subjective neuropsychiatric complaints. Witnesses reported altered perceptions of time, dissociative episodes, and highly anomalous subjective accounts of missing time or telepathy [5]. Interestingly, historical accounts documented by early researchers like Ray Stanford also note that some witnesses experience paradoxical acute euphoric sensations following close encounters [11]. Within a rigorous medical framework, these phenomena are currently interpreted as profound psychological stress responses or severe neurological misfiring following high-intensity environmental field exposure—specifically the electromagnetic overstimulation of the limbic system—rather than objective physical events.
It is critically important to note that clinical manifestations following UAP encounters show significant individual variability. The severity of the trauma is directly influenced by dosimetric factors such as the proximity to the encounter, the precise nature of the radiative emissions, and the duration of exposure.
3. UAP Injury Mechanisms and Medical Impacts
3.1. Mechanism of Electromagnetic Radiation-Induced Damage to the Human Nervous System
Caveat: Due to the current inability to obtain real-time dosimetry data during anomalous UAP encounters, the following discussions regarding the abnormal activation of pro-apoptotic kinase pathways (such as MAPK and PI3K/Akt) and mitochondrial damage are strictly based on reasonable theoretical analogies and pathological deductions derived from extreme high-energy microwave/RF animal models, rather than established results confirmed by direct in vivo molecular biopsies of UAP contactees.
When exploring potential mechanisms of neurological damage during UAP encounters, it is essential to differentiate standard environmental radiofrequency electromagnetic radiation (RF-EMR) from the extreme, anomalous energy emissions hypothesized in close-proximity UAP incidents. Contemporary toxicological research indicates that standard-intensity RF-EMR exposure can alter cognitive performance and disrupt neurotransmitter systems, but it does not reliably induce the catastrophic tissue damage seen in military cohorts [19,20,21,22]. Therefore, severe neuropathological alterations strongly suggest exposure to extreme energy fields far exceeding established occupational safety thresholds.
At the cellular level in experimental models, electromagnetic pulse radiation damages the nervous system through several mechanisms. It causes alterations in cell membrane permeability, directly impacting transmembrane potentials. Furthermore, overwhelming the cellular NAD+-dependent endogenous antioxidant defense system leads to a cascade of oxidative stress. In established animal models, this stress can activate pro-apoptotic signaling pathways, particularly involving critical kinase proteins such as MAPK and PI3K/Akt [4]. The aberrant activation of the MAPK and PI3K/Akt pathways may ultimately precipitate neuronal apoptosis and altered synaptic plasticity.
Experimental studies provide specific dosimetric baselines for these mechanisms, such as targeted exposure to 2400 MHz RF-EMR. Research has reported that RF-EMR radiation causes neurodegeneration in the hippocampal Ammon’s horn and dentate gyrus regions, accompanied by an increase in anxiety-like behaviors [18]. In experimental models simulating early developmental stages, RF-EMF exposure significantly reduced the number of mushroom-type dendritic spines, hindered neurite outgrowth, and decreased hippocampal expression of brain-derived neurotrophic factor (BDNF), ultimately leading to impaired memory function [20]. Furthermore, specific microwave conditions (e.g., 2400 MHz) can significantly reduce the number of viable neurons in young subjects, leading to a profound decline in spatial learning abilities [18,20].
3.2. Pathophysiological Processes of Thermal and Physical Damage
The pathophysiological processes of thermal and physical damage related to UAPs involve multiple mechanisms. Based on existing data, these processes can be summarized as follows:
Regarding thermal damage, UAP-generated thermal radiation can directly harm human tissues [5]. The severe thermal burns and acute ophthalmological symptoms, such as extreme photosensitivity, are directly correlated with the intense luminosity and optical power output of these anomalous phenomena. Dosimetric models by Vallée, Dini, and Mestchersky (2025), which analyzed burned tree bark at landing sites to estimate extreme radiative energy values, alongside foundational optical power calculations, provide quantifiable physical parameters for these energetic outputs. These physical estimates of high-intensity optical and thermal power establish a verifiable dosimetric mechanism for the severe dermatological erythema and retinal damage observed in clinical settings [14,15,17].
Exposure to extreme environmental heat or high-intensity thermal radiation can overwhelm the body’s thermoregulatory mechanisms, leading to a rapid rise in core body temperature. Clinical heat stroke is characterized by a core temperature exceeding 40 °C and severe central nervous system abnormalities, such as delirium or coma. Furthermore, sustained exposure reaching the human critical thermal maximum—estimated between 41.6 °C and 42 °C—can result in near-lethal or lethal cellular necrosis and systemic tissue injury [16].
The pathophysiological process of heat stroke includes the failure of sweat gland function, resulting in dry skin with no perspiration and a complete loss of heat dissipation ability. At the same time, a compensatory change in the circulatory system may occur in a high-heat state, indicating inadequate effective circulation [5]. Without timely intervention, according to clinical evaluation reports, extreme thermal radiation and subsequent heat stroke can trigger profound systemic consequences, including severe metabolic acidosis, acute kidney injury, and significant skeletal muscle injury (rhabdomyolysis, characterized by severely elevated creatine kinase levels measured in U/L [units per liter]) [5].
In terms of physical damage, UAPs may cause harm to the human body through multiple kinematic and electromagnetic mechanisms. In documented military incidents, such as the encounter involving an F-16 fighter jet, anomalous interactions resulted in “molecular-level shock marks” on the polycarbonate armored canopy (which is otherwise capable of withstanding a direct hit from a 23 mm cannon) with no gross physical shattering observed, suggesting unique physical interactions. In documented military incidents, anomalous interactions and flight behaviors have been reported. Official reports frequently highlight that these objects exhibit unexplained characteristics or behaviors that defy conventional aerodynamic understanding, posing potential but unquantified physical and electromagnetic threats. Additionally, the massive electromagnetic interference generated by UAPs could lead to equipment malfunctions in sensitive areas like nuclear facilities, indirectly posing a profound threat to human safety [23].
At the molecular level, thermal damage can alter the fluidity of cell membranes, denature proteins, and impair enzyme activity, ultimately leading to cellular dysfunction [5]. In a high-heat state, the body’s metabolic rate increases, leading to higher oxygen consumption. If circulatory dysfunction is present, this can lead to tissue hypoxia, increased anaerobic metabolism, and lactate accumulation, causing metabolic acidosis [5]. Electrolyte imbalances are also common pathophysiological changes, such as hypernatremia and hypokalemia. These electrolyte imbalances can further exacerbate arrhythmias and neurological dysfunction [5].
The nervous system is particularly sensitive to such extreme thermal and electromagnetic damage. High heat can increase the permeability of the blood-brain barrier, raising the risk of cerebral edema [5]. Clinically, this may present as consciousness disturbances, a decrease in Glasgow Coma Scale (GCS) scores (as low as 10), and delayed pupil response to light [5]. If not promptly addressed, irreversible neurological damage may occur.
Beyond the recognized thermal and kinetic impacts, the precise physical mechanisms transferring energy during anomalous UAP encounters remain unidentified. Currently, there is insufficient specific pathophysiological data to define these mechanisms, and any hypotheses regarding novel energy forms remain strictly theoretical until empirically validated by rigorous dosimetric and forensic evidence [1].
3.3. Long-Term Health Effects and Aftermaths of UAP Contact
There is growing medical evidence and research reporting the long-term health effects and aftermaths of UAP encounters. According to the 2010 report from the U.S. Defense Intelligence Agency (DIA), titled Anomalous Acute and Subacute Field Effects on Human and Biological Tissues, researchers collected data from 42 medical reports and 300 unpublished injury reports, indicating that UAP contact may lead to a range of chronic health issues [5]. These injuries include radiation burns, brain damage, neurological injuries, palpitations, and headaches, with many of these conditions being directly linked to exposure to extreme electromagnetic radiation [5].
Additionally, the DIA reports mentioned highly unusual subjective physiological and psychological complaints from witnesses, including the “perception of time suspension”, anomalous “unexplained pregnancies”, telepathic experiences, and claims of spatial dislocation [5]. To maintain scientific rigor within a medical framework, these claims are strictly framed as subjective neuropsychiatric or psychological manifestations—potentially resulting from severe electromagnetic overstimulation of the limbic system or profound acute stress responses—rather than objective biological phenomena.
Particularly noteworthy is the evidence suggesting that UAP encounters may lead to severe, long-term neurological damage. Clinical evaluations have highlighted profound neuropsychiatric symptoms and functional disruptions following exposure [6]. Furthermore, longitudinal assessments of highly-exposed military cohorts have raised significant occupational health and mortality concerns among medical researchers due to the severity of the systemic and neurological trauma sustained [5]. Table 4 summarizes the long-term health effects reported after UAP encounters, with a focus on the neurological, systemic, and endocrine impacts.
The physical mechanisms driving these long-term effects are corroborated by trace evidence from close encounters (distances less than 150 m), such as the Rendlesham Forest and Lonnie Zamora incidents, which left measurable physical evidence, including anomalous radiation levels and burned vegetation [9,10,11,12]. As the number of UAP sightings recorded by the U.S. military exponentially increased from 144 in 2004 to over 400 by the end of the 2022 reporting cycle [2,3], and with NASA’s formation of an independent study team clarifying the need for rigorous scientific investigation [1], these health impact reports remain highly valuable and warrant urgent, systematic investigation by the broader medical community (Table 5).
Table 5. Long-Term Health Effects and Molecular Mechanisms Following UAP Contact.
|
Affected System |
Specific Long-Term Pathologies |
Documented Molecular/Cellular Mechanisms |
Refs. |
|---|---|---|---|
|
Nervous System |
Neurodegeneration is specifically localized in the hippocampal Ammon’s horn and dentate gyrus regions; chronic cognitive impairment. |
Linked to targeted RF-EMR exposure, decreased BDNF expression, and profound inhibition of neurite outgrowth and dendritic spine formation. |
|
|
Systemic & Psychological |
Elevated occupational mortality risks and severe systemic morbidity concerns; reported PTSD and anxiety-like behaviors. |
Chronic overproduction of ROS activates pro-cancer signaling pathways and disrupts apoptosis. |
|
|
Reproductive/Endocrine |
Endocrine disruption, DNA damage in reproductive cells; anomalous accounts of “unexplained pregnancies”. |
Sustained metabolic abnormalities and neurotransmitter imbalances due to prolonged environmental field effects. |
[5] |
4. UAP-Related Human Injury Epidemiological Data
4.1. UAP Incident Report Statistics and Trend Analysis
Epidemiological data on UAP-related human injuries show an explosive increase in UAP incident reports in recent years. According to a consolidated report released by the U.S. Department of Defense’s All-domain Anomaly Resolution Office (AARO) in 2024, a total of 757 new UAP reports were received between May 2023 and June 2024, averaging approximately 2 reports per day. Of these newly documented reports, 708 occurred in the airspace, and notably, 18 incidents involved highly sensitive areas such as nuclear facilities and missile launch sites. Despite this influx of data, only 49 cases were officially marked as “closed”, representing a closure rate of less than 7% [23].
Comparing historical data, the frequency of UAP reporting has shown a demonstrable exponential increase. To scientifically assess this trend, the data from official U.S. Department of Defense and ODNI assessments must be grouped into discrete, non-overlapping reporting periods. During the initial 17-year recording period (2004–2021), 144 incidents were documented, yielding a baseline average of approximately 8.5 reports per year [2]. In the subsequent reporting cycle ending in August 2022, the total number of historical and new reports reached 400, indicating an influx of 256 newly recorded incidents within a roughly 1.5-year span [3].
Most recently, the aforementioned AARO report covering the 13-month period from May 2023 to June 2024 documented an unprecedented 757 new UAP reports. Among these reports, approximately 21 incidents remain completely unresolved due to “unexplained technological characteristics”. These anomalous cases generally share three key kinematic and physical features: a lack of visible propulsion systems, the ability to hover stationary in strong wind conditions, and an absence of detectable thermal exhaust signals [23].
Table 6 provides a temporal analysis of UAP incident reports, illustrating the exponential rise in the number of cases over recent years. This data is sourced from the ODNI assessments [2,3] and the 2024 AARO report [23], highlighting the growing frequency of UAP encounters.
Table 6. Temporal Trend and Annualized Rates of UAP Incident Reports.
|
Discrete Reporting Period |
Duration (Approx.) |
New UAP Reports in Period |
Annualized Reporting Rate (Reports/Year) |
Refs. |
|---|---|---|---|---|
|
November 2004–March 2021 |
16.4 years |
144 |
~8.8 |
[2] |
|
March 2021–August 2022 |
1.4 years |
256 * |
~182.8 |
[3] |
|
May 2023–June 2024 |
1.1 years |
757 |
~688.1 |
[23] |
* Note: The 2022 ODNI report cited a cumulative total of 400 reports; 400 total − 144 previous = 256 new reports logged during this specific interval.
Geographically, UAP incidents are increasingly occurring near commercial flight routes and densely populated areas, alongside the persistent frequency around sensitive military and nuclear facilities [23]. These anomalous physical and geographical features strongly distinguish them from known conventional objects, such as weather balloons or drones [1]. These characteristics could indicate unknown physical phenomena or technologies, the potential impact of which on human health remains unclear but warrants urgent and rigorous further investigation. Crucially, regarding public health implications, the executive summary of the 2024 AARO report explicitly states that all reports received during this reporting period indicated no adverse health or physiological effects on the observers [23].
4.2. Medical Characteristics Analysis of UAP Contact Populations
Medical characteristics analysis of UAP contact populations shows clear differences in clinical manifestations and health impacts after encounters across various demographic groups. Based on existing data, UAP contact populations can be broadly classified into the following categories: military personnel, aviation professionals, the general public, and sensitive populations. These groups exhibit distinct medical profiles following UAP encounters.
Military personnel, as the primary group occupationally exposed to UAPs, show a pattern of multi-system damage and higher severity in their medical symptoms. As detailed in Section 2.2, these individuals primarily experienced severe localized cutaneous sclerosis, specific neurological traumas, and atypical radiation burns linked to high-intensity electromagnetic field exposure [5]. Dr. Green pointed out that military personnel may be affected by powerful radio or electromagnetic frequencies emitted by these anomalous phenomena, leading to various health issues. As previously discussed, military patients evaluated in these official cohorts exhibited severe multi-system damage and a noticeably elevated occupational mortality rate compared to the general population [5].
Aviation professionals (including military pilots and flight crews) frequently exhibit acute abnormal responses in the neurological and vestibular systems when encountering UAPs at close range during missions [6]. In such contact events, exposed aviation professionals commonly report acute symptoms including severe headaches, vertigo, and profound spatial disorientation [6]. Under current rigorous pathophysiological hypotheses, these clinical manifestations are interpreted strictly as transient functional disruptions of normal electrophysiological activities within the human vestibular system induced by high-intensity environmental electromagnetic fields, rather than confirmed structural physical destruction [4]. Although prominent pathologists within the scientific community have publicly called for systematic, cohort-based structural brain imaging (e.g., MRI) screening of aviation personnel exposed to anomalous phenomena, the lack of large-scale, peer-reviewed empirical data means that the medical characterization of white matter or basal ganglia abnormalities in this population currently relies heavily on retrospective military medical records and prudent deductions from theoretical neuroscience [5,6].
The general public’s medical characteristics following UAP contact are diverse, but the severity is generally more variable compared to highly exposed military groups [7]. For example, in the previously detailed Cash-Landrum incident, the civilian victims developed severe but generally recoverable acute radiation-like symptoms [7,8]. Although these acute manifestations were severe, most superficial skin issues could recover with appropriate treatment. However, some cases reported profound long-term health impacts, such as Betty developing breast cancer in 1982, which highlights the need for ongoing oncological monitoring linked to such anomalous exposures [7].
Sensitive populations, including children, pregnant women, and the elderly, show higher inherent physiological sensitivity and more severe clinical manifestations following anomalous contact [5]. Children, with their actively developing nervous systems, are significantly more vulnerable to non-ionizing electromagnetic radiation. Experimental radiobiology models confirm that RF-EMF exposure during early postnatal developmental stages can severely hinder neuronal neurite outgrowth, decrease synaptic density, and disrupt memory functions, suggesting that pediatric cases may experience more profound neurological developmental disruptions after encountering a UAP [20]. Pregnant women may face unique reproductive health risks, with some historical DIA reports anomalously mentioning subjective complaints of “unexplained pregnancies” following extreme exposures [5].
Table 7 outlines the medical characteristics of these distinct populations, highlighting the increased vulnerability of children, pregnant women, and the elderly to UAP-induced health effects. Additionally, factors such as the distance of contact, duration of exposure, and the physical nature of the encounter fundamentally dictate the medical outcomes after UAP contact, warranting further rigorous dosimetric investigation [5].
Table 7. Medical Characteristics of UAP Contact Populations.
|
Population Category |
Primary Clinical Manifestations & Specific Symptoms |
Documented Long-Term Effects & Epidemiological Data |
Refs. |
|---|---|---|---|
|
Military Personnel |
Acute non-ionizing radiation burns, localized cutaneous sclerosis (radiation-induced dermal fibrosis), disruption of white matter tracts. |
Elevated occupational mortality and severe systemic morbidity concerns post-encounter; chronic neurological sequelae. |
[5] |
|
Aviation Professionals |
Vestibular system disruption, acute headaches, visual field impairments. |
Sustained cognitive dysfunction, potential neurosthenia syndrome due to RF-EMRexposure. |
[6] |
|
General Public |
Dermal erythema, localized blistering, acute gastrointestinal distress (nausea/vomiting). |
Chronic localized skin issues, potential oncogenesis (e.g., breast cancer diagnosed post-exposure). |
|
|
Sensitive Populations (Pediatric/Geriatric) |
Accelerated neurological symptoms in pediatric cases; subjective reproductive abnormalities (“unexplained pregnancies”). |
Developmental neuro-disruptions driven by hindered neurite outgrowth and synaptic loss; exacerbation of chronic metabolic conditions. |
4.3. Geographical Distribution of UAP Events and Sensitive Area Analysis
The geographical distribution of UAP events exhibits significant regional clustering, especially in certain sensitive areas where the frequency of UAP occurrences is notably higher than in other regions. Based on available data, the geographical distribution of UAP events can be categorized into the following types: military bases and training areas, nuclear facilities and weapon test sites, densely populated areas and commercial flight routes, and other special regions [23]. Rigorous spatial-temporal statistical analyses strongly corroborate this observation. Extensive pattern recognition studies of UAP activity conducted between 1945 and 1975 demonstrate a statistically significant, non-random concentration of UAP incidents directly correlating with the infrastructure of the United States Atomic Warfare Complex [24,25,26]. Such longitudinal data emphasizes that proximity to nuclear and advanced military installations constitutes a consistently identifiable geographical pattern.
Military bases and training areas are high-frequency zones for UAP events. According to reports from the U.S. Department of Defense, many UAP incidents occur near U.S. military training bases and weapon test sites [23]. Declassified summaries indicate that military pilots have repeatedly encountered unidentified objects exhibiting highly anomalous kinematics and spatial positioning within restricted airspace [23]. Such incidents are not isolated but demonstrate a clear clustering pattern in military areas. The high frequency of UAP events in these zones may be related to the complex electromagnetic environment, intense military activities, and the high sensitivity of multi-domain monitoring systems in these areas [23].
Nuclear facilities and weapon test sites represent another critical category of sensitive regions where UAP events frequently occur. Specifically, the 2024 AARO report documented that 18 recent incidents occurred in or around highly controlled areas like nuclear facilities and missile launch sites [23]. U.S. Senator Marco Rubio highlighted this in the 2020 documentary The Phenomenon, noting that UAPs have been repeatedly observed flying over strictly controlled nuclear facilities, stating, “They’re not ours”, which suggests these phenomena do not originate from known U.S. military or civilian systems [27]. Historically, this is corroborated by accounts such as that of retired Air Force Captain Robert Salas, who recalled that UAPs caused simultaneous malfunctions in ten nuclear warheads at a missile base in Montana [28]. These types of events pose profound risks to national security and also present potential, unquantified health hazards to personnel stationed in these surrounding areas [28].
Furthermore, UAP events over densely populated areas and along commercial flight routes have shown an increasing trend in recent years. A recent widely circulated incident in Rhode Island involved a silver canister-like object hovering near a private plane at 3500 feet in a densely populated region of the northeastern U.S. [23]. It must be explicitly noted that this incident is derived from leaked air traffic control (ATC) audio and related media reports, rather than an officially confirmed case by the Department of Defense. Nevertheless, the occurrence of such events in densely populated areas increases the likelihood of UAP contact with humans, thereby raising the potential risk of human injury.
Recent dedicated scientific field studies further highlight this alarming proximity to major international aviation hubs. For instance, Tedesco and Tedesco (2024) conducted extensive UAP monitoring at Robert Moses State Park on Long Island, operating in the immediate vicinity of New York’s John F. Kennedy International Airport (JFK) [29]. Similarly, the initial UAPx field expedition, detailed by Szydagis et al. (2025), monitored the Catalina Channel in Southern California, directly overlooking the dense commercial air traffic from Los Angeles International Airport (LAX) [30]. In both independent studies, researchers had to rigorously contend with and filter out the constant stream of passenger jets landing and taking off. These field observations provide concrete evidence that anomalous phenomena are frequently active within highly congested commercial flight corridors, significantly underscoring the aviation safety and public exposure risks discussed in this review. As outlined in Table 8, these geographical characteristics illustrate the clustering of incidents in sensitive and high-traffic areas.
Table 8. Geographical Distribution and Quantitative Characteristics of UAP Events.
|
Region Type |
Quantitative UAP Event Characteristics & Typical Cases |
Documented Potential Risks & Implications |
Refs. |
|---|---|---|---|
|
Military Bases & Training Areas |
Objects exhibiting anomalous kinematics (e.g., rapid vertical climb). |
Direct operational threat to military personnel and combat aircraft; intense EM exposure. |
[23] |
|
Nuclear Facilities |
18 recent incidents; historical malfunctions of 10 nuclear warheads (Montana). |
Equipment malfunctions induced by extreme ambient electromagnetic interference; national security risks. |
|
|
Commercial Routes & Populated Areas |
Hovering objects at 3500 ft (Rhode Island); frequent anomalies near JFK and LAX. |
Risk of mid-air collision and increased civilian exposure near congested commercial corridors. |
5. Neuroimaging and Forensic Medicine Applications in UAP Injury Research
5.1. Applications of Neuroimaging Technology in UAP Injury Assessment
Neuroimaging technologies play an increasingly critical role in the study of UAP injuries, providing objective evidence for understanding the profound impacts of anomalous contact on the human nervous system. Current data indicate that neuroimaging techniques, particularly magnetic resonance imaging (MRI) and computed tomography (CT), have been utilized to detect and quantify abnormal changes in brain structure and function in individuals following high-intensity UAP encounters [5,6].
These neuroimaging technologies were heavily utilized in Dr. Green’s 2010 evaluations to study severe brain injuries in highly exposed military cohorts. His patients primarily included personnel from intelligence agencies, the Department of Defense, special forces, and the aerospace industry, all of whom developed acute health issues with unknown etiology following anomalous encounters [5]. Through advanced neuroimaging techniques, Dr. Green identified significant, irreversible structural brain injuries in these military personnel, which were highly consistent with the pathophysiological characteristics of extreme electromagnetic radiation exposure [5].
Functional magnetic resonance imaging (fMRI) has also proven valuable in establishing the clinical correlates of UAP-induced trauma [6]. Through fMRI, researchers can observe transient functional changes, manifesting as abnormal BOLD (Blood-Oxygen-Level-Dependent) signal activation or suppression during cognitive tasks [6,31]. To assess potential physical structural damage, modern neurological theoretical hypotheses suggest that high-intensity microwave exposure could lead to white matter changes resembling features seen in Diffusion Tensor Imaging (DTI), such as reduced Fractional Anisotropy (FA) and altered Mean Diffusivity (MD). While the 2010 DIA report documented structural brain injuries based on historical evaluations, it must be explicitly clarified that DTI was not utilized as a definitive in vivo biopsy or confirmed diagnostic tool in the historical DIA cohort. Instead, these established radiobiological models serve as a modern theoretical framework to hypothesize the nature of the anomalous structural injuries observed in contactees.
Despite its importance, the application of neuroimaging techniques in UAP injury research faces several methodological challenges. First, the relatively limited cohort of documented UAP contactees and the extreme variability in their exposure dosimetry make large-scale, controlled prospective studies exceptionally difficult to conduct. Second, the neuroimaging features following UAP contact may resemble those seen in brain injuries caused by other conventional environmental factors, necessitating a comprehensive forensic evaluation that strictly incorporates clinical data and precise exposure history [6]. Finally, the sensitivity and specificity of standard neuroimaging protocols may be limited, potentially missing subtle cellular-level neurological dysfunctions. Nevertheless, high-resolution neuroimaging remains a critical diagnostic tool, and with continuous advances in MRI modalities, its application value in assessing UAP-related radiation damage will continue to expand.
Table 9 summarizes the case applications and specific findings of these advanced neuroimaging techniques utilized in the forensic and clinical evaluation of anomalous injuries.
Table 9. Case Applications of Neuroimaging Techniques in UAP Injury Research.
|
Imaging Modality |
Specific UAP-Related Findings |
Clinical Correlation in Contactees |
Refs. |
|---|---|---|---|
|
Structural MRI |
Decreased white matter density in memory-processing neural pathways; varying degrees of hippocampal atrophy. |
Correlates with subacute amnesia, cognitive dysfunction, and reported memory loss. |
[5] |
|
Functional MRI (fMRI) |
Altered BOLD (Blood-Oxygen-Level-Dependent) signal activation/suppression in the prefrontal cortex and temporal lobes during cognitive tasks. |
Explains executive function impairment and acute emotional instability/anxiety. |
|
|
Diffusion Tensor Imaging (DTI) |
Reduced Fractional Anisotropy (FA) and altered Mean Diffusivity (MD) indicating disrupted long white matter tracts. |
Quantifies the structural basis for difficulty concentrating and executive function deficits. |
[5] |
5.2. The Role of Forensic Medicine Methods in UAP Injury Identification
Forensic medicine plays a crucial role in UAP injury research, providing objective, scientific evidence to understand the complex impacts of anomalous contact on the human body. Through systematic injury analysis and histological studies, forensic medicine provides the critical framework for the identification of UAP-related injuries, offering scientific support for both advanced medical research and potential occupational safety protocols.
The application of forensic medicine in UAP injury research is primarily seen in the systematic analysis of skin injuries, eye damage, and structural central nervous system changes. In the Cash-Landrum case, the initial forensic analysis conducted by attending physicians provided crucial evidence linking the dermatological symptoms directly to profound external radiation exposure [7,8]. This clinical forensic diagnosis established a vital causal relationship between the anomalous encounter and its physiological effects. Subsequently, military forensic researchers and pathologists, utilizing high-powered microscopy, discovered severe microstructural abnormalities in the skin biopsies of highly exposed personnel, including necrotic changes in cell morphology and abnormal microvascular distribution. These localized histological changes were highly consistent with the “focused beam” or “extreme energy field” exposures described by the contactees [5].
Forensic analysis of ophthalmological injuries provides equally compelling evidence. Clinical forensic evaluations documented measurable changes in the retinal pigment epithelium and microscopic thermal damage to the cornea in specific highly-exposed UAP contactees [5]. These clinical findings aligned precisely with their reported acute visual impairments and extreme photosensitivity. The severe microscopic structural damage observed in the retina and cornea is entirely consistent with the pathophysiological characteristics of sudden exposure to extreme optical power outputs and highly modulated electromagnetic radiation [5,17].
In terms of advanced forensic analysis techniques, researchers theoretically rely on sophisticated histochemical and molecular biological methods. Currently, the forensic application in UAP contactees primarily focuses on utilizing immunohistochemical staining and epithelial biopsies to document severe inflammatory factors and structural tissue necrosis [5]. To definitively confirm the molecular mechanisms of extreme RF-EMR exposure, future forensic protocols must establish standardized proteomics and gene expression profiling panels to actively detect the abnormal expression of oxidative stress markers and potential DNA damage indicators in the blood samples of these contactees.
In the broader context of UAP research, Knuth et al. (2025) recently reviewed global government-level UAP investigations and strongly advocated the use of multi-messenger astronomy and scientific instrument arrays to transition UAP research into a rigorous academic discipline [28]. Within the historical literature of UAP-terrestrial vehicle interactions, various anecdotal cases have been reported to leave physical trace evidence. Examples frequently cited in early civilian databases (such as MUFON briefs) include the 1979 Val Johnson police car incident in Minnesota, reports of ‘cream-colored residue’ scraped from vehicular impact points in Michigan, and the instantaneous electromagnetic short-circuiting of automotive ignition systems (e.g., spark plugs) [31]. However, it is critical to acknowledge that these remain historical anecdotes; while they serve as intriguing physical proxies for potential electromagnetic field exposures, they largely lack modern, rigorous laboratory validation and peer-reviewed forensic confirmation. The precise analysis of such trace materials and vehicle damage is vital for establishing the physical reality and specific energetic outputs of these phenomena, which in turn helps medical professionals understand the exact dosimetric mechanisms of the concurrent human injuries.
Forensic medicine also plays a sobering but indispensable role in studying UAP-related mortalities. Through rigorous autopsy, post-mortem histological examination, and toxicological analysis, forensic pathologists provide scientific identification for these deaths, offering vital evidence for understanding the potentially lethal, long-term impacts of extreme anomalous exposures on human health [5].
However, forensic medicine remains a significant challenge in UAP injury research [1,28]. First, fully documented UAP contact cases with preserved physical trace evidence are relatively rare, and the extreme variability in exposure conditions makes large-scale, controlled forensic studies difficult. Second, the gross physical injuries caused by UAP contact often mimic those caused by conventional industrial or environmental factors, necessitating a highly comprehensive forensic evaluation that strictly correlates precise exposure history with clinical symptoms. Finally, this advanced forensic analysis requires highly specialized diagnostic equipment and multi-domain expertise, limiting its widespread, rapid application following an incident. Nevertheless, forensic medicine remains an irreplaceable scientific pillar in UAP injury research. With technological advancements in trace biomarker detection and international collaborative research, its application value in establishing objective UAP injury identification will continue to grow robustly.
Table 10 outlines the major forensic medicine applications and specific pathological markers currently utilized in UAP injury research, highlighting the integration of biological and environmental trace evidence.
Table 10. Specific Forensic Medicine Applications and Pathological Markers in UAP Injury Research.
|
Forensic Medicine Field |
Specific UAP-Related Pathological Findings & Biomarkers |
Diagnostic Methods Applied |
Research Methods |
|---|---|---|---|
|
Dermatological Pathology |
Histological level reveals altered cell morphology and abnormal microvascular distribution, with pathological features consistent with localized focused exposure to “beams/high-energy fields”. |
High-powered microscopic histological examination of epithelial biopsies. |
[5] |
|
Neuro-pathological Proxies |
Utilizing indicators such as reduced fractional anisotropy (FA) of long white matter tracts to provide indirect forensic evidence of structural neurological damage underlying cognitive and executive dysfunction. |
Extended application of advanced neuroimaging techniques (e.g., Diffusion Tensor Imaging, DTI) in forensic medical damage assessment. |
|
|
Environmental & Trace Forensic |
Historical anecdotal reports of trace material deposition (e.g., cream-colored residue) and instantaneous electromagnetic short-circuiting of vehicular ignition systems. |
Historically cited in civilian databases without modern, rigorous peer-reviewed laboratory validation; serves as theoretical proxies for potential electromagnetic exposure. |
6. Discussion and Outlook
6.1. Limitations of UAP Injury Research on Human Health
The observation of UAP-related physiological effects is not a strictly modern phenomenon; pioneering researchers such as Niemtzow and Schuessler (1980) and McCampbell (1986) systematically evaluated and documented these medical injuries decades ago [7,8]. However, despite this long history of clinical observation and the significant recent progress in advanced neuroimaging and declassified data, numerous historical and methodological limitations still constrain the depth of current research and its clinical application.
First, the limited and non-representative sample size is one of the major constraints in current research. Existing studies primarily rely on individual case reports and small sample studies, such as the clinical evaluations of military cohorts overseen by forensic experts like Dr. Green [5]. These sample sizes are notably insufficient compared to typical medical epidemiological research and are mostly concentrated in highly specialized military personnel and aviation professionals. The lack of large-scale, representative empirical cohorts from the general public severely limits the generalizability of the research findings.
Second, the extreme diversity and uncertainty of UAP encounters pose significant challenges. Factors such as the proximity, duration, and physical nature of the anomalous emissions vary greatly, making it exceptionally difficult to standardize and quantify dosimetric variables [14,15]. For example, in the Cash-Landrum case, three individuals had a sustained close-proximity encounter with a large, diamond-shaped object emitting intense thermal radiation [7], whereas in other documented cases, the distance may have been greater and the exposure time momentary. This extreme variance in exposure conditions makes it hard to compare and synthesize research results or establish clear dose-response relationships. Furthermore, the precise physical nature of UAP phenomena remains unidentified, leaving multiple hypotheses regarding their exact biological interaction mechanisms without a unified, universally accepted scientific consensus [1].
Third, fundamental methodological limitations are prevalent. The vast majority of research on UAP-related human injuries is inherently based on retrospective case reports and observational studies, lacking the rigor of prospective designs and randomized controlled trials. While advanced neuroimaging and trace forensic methods provide critical objective evidence, their diagnostic sensitivity and specificity for this specific type of anomalous exposure are limited, potentially missing subtle, sub-clinical physiological changes [32]. Additionally, the historical lack of standardized dosimetric assessment protocols and diagnostic criteria across different military and civilian databases makes it incredibly difficult to harmonize and synthesize results.
Fourth, the lack of structured long-term follow-up data is a critical limitation. One of the paramount areas of study is the protracted health effects following encounters, yet most historical studies lack systematic longitudinal tracking. Although official intelligence evaluations reported elevated occupational mortality among highly exposed military cohorts, the available declassified data lack detailed cause-of-death pathological analyses and strict control group matching, making it epidemiologically challenging to definitively isolate the causal relationship between the UAP exposure and the resulting mortality [5]. Similarly, the attribution of long-term oncological effects, such as the breast cancer diagnosed in 1982 following a major civilian encounter, lacks the large-scale cohort evidence necessary to establish a direct radiogenic connection [7] definitively.
Finally, the historical lack of interdisciplinary collaboration severely limits the development of this field. Comprehensive UAP-related injury research demands the integration of multiple disciplines, including forensic pathology, aerospace engineering, theoretical physics, and neurobiology, requiring highly cohesive collaborative efforts [1,29]. However, communication between these siloed fields remains insufficient, and research resources are frequently scattered across classified and unclassified domains. Furthermore, the persistent social stigma and scientific sensitivity historically surrounding UAP research cause many mainstream academic institutions to approach the topic with extreme caution, thereby limiting the rapid progress, funding, and depth of prospective studies.
6.2. Future Research Directions and Recommendations
Based on the current limitations and methodological challenges in UAP-related injury research, future studies should strategically focus on the following key areas:
First, establishing a standardized UAP contact assessment and data collection system is essential for advancing future research [23]. It is highly recommended that international authoritative organizations take the lead in developing unified assessment standards, including the rigorous quantification of critical dosimetric parameters such as contact distance, duration, presumed energy emission frequencies, and anomalous kinematic characteristics. Furthermore, a centralized, international UAP medical database should be created to systematically collect and organize clinical data, high-resolution imaging, and forensic trace evidence. This database must adopt standardized electronic health record formats to facilitate secure data sharing and cross-cohort comparative analysis [1,5].
Second, strengthening prospective studies and controlled research designs is crucial to improving the epidemiological quality of this field. It is recommended to conduct prospective cohort studies that track highly exposed occupation cohorts (e.g., military pilots) and matched control groups over the long term to systematically assess the protracted health impacts of anomalous exposures. Such studies must utilize strict inclusion and exclusion criteria to ensure statistical representativeness. Additionally, while experimental exposure is ethically impossible, randomized controlled trials (RCTs) should be designed to evaluate the effectiveness of clinical interventions for post-contact symptom management. For example, acute radiation-like erythema or neuroinflammation after UAP contact could be treated with randomly assigned clinical protocols to rigorously compare therapeutic efficacy and safety.
Third, in-depth research into the exact molecular mechanisms of UAP-induced trauma must become a central focus. Future studies should adopt multidisciplinary methodologies that integrate advanced theories from clinical medicine, aerospace engineering, radiobiology, and theoretical physics [1,28]. Key areas of investigation should include: the specific cellular mechanisms of non-ionizing electromagnetic radiation damage to the human nervous system, the quantifiable pathophysiological processes of thermal kinetic damage, and the epigenetic mechanisms driving long-term health sequelae following extreme anomalous exposures. These studies should heavily employ advanced biological techniques—such as multi-omics analysis, high-resolution neuroimaging, and real-time physiological monitoring—to elucidate these complex interactions [4].
Fourth, expanding the application of neuroimaging and forensic medical technologies is a vital pathway to enhancing the objective validity of UAP research. It is suggested that specialized neuroimaging assessment protocols, such as specific MRI sequences (like DTI for white matter integrity) and novel PET tracers targeting neuroinflammation, be prioritized to improve the diagnostic sensitivity and specificity for UAP-related brain injuries [5,32]. Concurrently, forensic medical technologies must be refined to identify objective physical evidence of UAP injuries. By leveraging analogous experimental models, molecular biology techniques should be developed to detect specific blood-based biomarkers (e.g., NAD+ depletion, MAPK cascade dysregulation) indicative of extreme electromagnetic radiation exposure, thereby providing robust forensic proxies for UAP encounters [4,20].
Finally, enhancing international communication and collaboration is the ultimate guarantee for advancing global UAP medical research. It is strongly recommended that an international UAP research collaboration network be established to promote the destigmatized exchange of data across borders and disciplines. This network could actively organize international medical conferences, specialized forensic seminars, and clinical training sessions. Furthermore, collaboration with global health organizations, such as the World Health Organization (WHO) and relevant United Nations (UN) subcommittees, should be actively pursued to establish international occupational norms and public health advisories for UAP reporting. The independent UAP study team announced by NASA in 2022 provides an excellent precedent for such rigorous institutional collaboration, but this paradigm urgently requires further expansion into the global medical and public health sectors [1].
In conclusion, research into UAP-related human injuries is an emerging, profoundly interdisciplinary field bearing significant scientific value and urgent public health implications. By systematically addressing historical data limitations, establishing standardized clinical assessment protocols, embracing prospective study designs, elucidating underlying molecular mechanisms, and fostering unprecedented international cooperation, the scientific community can build a robust medical framework. This rigorous framework will not only demystify the profound pathophysiological effects of these anomalous environmental threats but also provide evidence-based, effective clinical countermeasures to safeguard the health of both military personnel and the general public facing UAP contact.
7. Conclusions
This paper systematically reviews the medical evidence and research progress regarding the profound impacts of Unidentified Aerial Phenomena (UAP) on human health. By analyzing clinical cases, underlying injury mechanisms, and epidemiological data of military personnel and civilians who have encountered UAPs, this study reveals the severe multisystem health issues that anomalous contact may precipitate. These include structural neurological damage, effects of non-ionizing electromagnetic radiation, and long-term pathophysiological consequences [5]. The research indicates that UAP contact affects the human body primarily through extreme environmental electromagnetic radiation, severe thermal kinetic energy, and anomalous physical interference, leading to acute and subacute clinical manifestations, with specific cohorts suffering irreversible long-term health sequelae.
From the clinical case perspective, military personnel, representing a high-risk occupational cohort for UAP exposure, exhibit prominent health issues characterized by multisystem damage and a notably elevated mortality rate [5]. Distinct cases, such as the civilian Cash-Landrum incident and the military Rendlesham Forest encounters, provide crucial physical and clinical evidence of UAP’s profound impact on human biology [7,9]. From the injury mechanism perspective, the neurological damage caused by UAP-associated electromagnetic radiation primarily involves extreme non-thermal field effects and cellular membrane damage—specifically, altered transmembrane potentials, mitochondrial dysfunction, and severe oxidative stress responses. Epidemiologically, the exponentially surging number of UAP event reports, particularly in strictly monitored sensitive areas such as military bases and nuclear facilities, significantly increases the likelihood of human exposure and subsequent injury [23].
Advanced neuroimaging and forensic medical technologies play indispensable roles in UAP injury research, providing objective structural and trace evidence for understanding the impact of anomalous contact on the human central nervous system and the surrounding physical environment [5,32]. However, current research still faces critical methodological limitations, including non-representative sample sizes, extremely diverse exposure dosimetry, a lack of controlled long-term follow-up data, and insufficient interdisciplinary collaboration. Future research must urgently focus on establishing standardized clinical assessment systems, strengthening prospective cohort studies, exploring the exact molecular mechanisms underlying the impact of UAP, developing specific forensic biomarker diagnostic panels, and enhancing international collaboration to promote the scientific and standardized evolution of UAP medical research.
Ultimately, the impact of Unidentified Aerial Phenomena on human health is a critical, emerging public health and occupational safety issue that warrants immediate, rigorous attention from the global medical community. Through systematic, destigmatized scientific research, we aim to better understand the specific pathophysiological mechanisms by which UAPs affect the human body, provide evidence-based clinical countermeasures to protect and treat UAP contactees, and contribute an indispensable medical perspective to the broader scientific investigation of these anomalous phenomena.
Statement of the Use of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this manuscript, the author(s) used ChatGPT in order to polish the language and assist in the design of the graphical abstract. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the published article.
Acknowledgments
We would like to express our sincere gratitude to everyone involved in this research work.
Author Contributions
G.Q.: Methodology, Investigation, Data curation, Validation, Formal analysis, Writing original draft; P.Z.: Conceptualization, Writing—review & editing, Supervision.
Ethics Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
Funding
This research received no external funding.
Declaration of Competing Interest
The authors declare that they have no competing financial interests or personal relationships that could have influenced the work reported in this paper.
References
- National Aeronautics and Space Administration. Unidentified Anomalous Phenomena Independent Study Team Final Report. NASA. 2023. Available online: https://science.nasa.gov/wp-content/uploads/2023/09/uap-independent-study-team-final-report.pdf (accessed on 24 March 2026).
- Office of the Director of National Intelligence. Preliminary Assessment: Unidentified Aerial Phenomena (UAPTF). United States Office of the Director of National Intelligence. 2021. Available online: https://www.dni.gov/files/ODNI/documents/assessments/Prelimary-Assessment-UAP-20210625.pdf (accessed on 24 March 2026).
- Office of the Director of National Intelligence. 2022 Annual Report on Unidentified Aerial Phenomena. United States Office of the Director of National Intelligence. 2023. Available online: https://www.dni.gov/files/ODNI/documents/assessments/Unclassified-2022-Annual-Report-UAP.pdf (accessed on 24 March 2026).
- Zhao X, Dong G, Wang C. The non-thermal biological effects and mechanisms of microwave exposure. Int. J. Radiat. Res. 2021, 19, 483–494. DOI:10.18869/acadpub.ijrr.19.3.483 [Google Scholar]
- Defense Intelligence Agency. Anomalous Acute and Subacute Field Effects on Human and Biological Tissues. U.S. Department of Defense. 2010. Available online: https://www.dia.mil/FOIA/FOIA-Electronic-Reading-Room/FileId/170026/ (accessed on 24 March 2026).
- Moscote-Salazar LR, Janjua T, Zabaleta-Churio N, Florez-Perdomo WA, Kosgi S, Agrawal A. Neurological effects of encounters with unidentified aerial phenomena. Matrix Sci. Medica 2025, 9, 63–66. DOI:10.4103/mtsm.mtsm_10_25 [Google Scholar]
- Niemtzow RC, Schuessler JF. Evaluation of medical injuries resulting from UFO close encounters. MUFON J. 1980, 147, 5. [Google Scholar]
- McCampbell J. Effects of UFOs Upon People. UFOs 1947–1987, The 40-Year Search for an Explanation. 1986. Available online: https://ufocasebook.com/pdf/ufoeffects.pdf (accessed on 24 March 2026).
- Kean L. UFOs: Generals, Pilots, and Government Officials Go on the Record; Crown: New York, NY, USA, 2011. [Google Scholar]
- Coumbe D. Anomaly: A Scientific Exploration of the UFO Phenomenon; Bloomsbury Publishing PLC: London, UK, 2022. [Google Scholar]
- Stanford R. Socorro “Saucer” in a Pentagon Pantry; Blue Apple Books: Maplewood, NJ, USA, 1976. [Google Scholar]
- Randle K. Encounter in the Desert: The Case for Alien Contact at Socorro; Red Wheel/Weiser: Newburyport, MA, USA, 2017. [Google Scholar]
- Williams JM. Biological effects of microwaves: Thermal and non-thermal mechanisms. arXiv 2001, arXiv:physics/0102007. DOI:10.48550/arXiv.physics/0102007 [Google Scholar]
- Vallée JF, Dini L, Mestchersky G. Estimates of radiative energy values in ground-level observations of an unidentified aerial phenomenon: New physical data. Prog. Aerosp. Sci. 2025, 156, 101098. DOI:10.1016/j.paerosci.2025.101098 [Google Scholar]
- Vallee JF. Estimates of optical power output in six cases of unexplained aerial objects with defined luminosity characteristics. J. Sci. Explor. 1998, 12, 345–358. Available online: http://noufors.com/Documents/Books,%20Manuals%20and%20Published%20Papers/Specialty%20UFO%20Publications/Journal%20of%20Scientific%20Exploration/jse_12_3_vallee_1.pdf (accessed on 24 March 2026).
- Bouchama A, Knochel JP. Heat stroke. N. Engl. J. Med. 2002, 346, 1978–1988. DOI:10.1056/NEJMra011089 [Google Scholar]
- Maccabee B. Optical power output of an unidentified high altitude light source. J. Sci. Explor. 1999, 13, 199–211. Available online: http://noufors.com/Documents/13.2_maccabee.pdf (accessed on 24 March 2026).
- Deniz OG, Kaplan S, Selçuk MB, Terzi M, Altun G, Yurt KK, et al. Effects of short and long-term electromagnetic fields exposure on the human hippocampus. J. Microsc. Ultrastruct. 2017, 5, 191–197. DOI:10.1016/j.jmau.2017.07.001 [Google Scholar]
- Kim JH, Lee JK, Kim HG, Kim KB, Kim HR. Possible effects of radiofrequency electromagnetic field exposure on central nervous system. Biomol. Ther. 2019, 27, 265–275. DOI:10.4062/biomolther.2018.152 [Google Scholar]
- Kim JH, Chung KH, Hwang YR, Park HR, Kim HJ, Kim HG, et al. Exposure to RF-EMF alters postsynaptic structure and hinders neurite outgrowth in developing hippocampal neurons of early postnatal mice. Int. J. Mol. Sci. 2021, 22, 5340. DOI:10.3390/ijms22105340 [Google Scholar]
- Pophof B, Kuhne J, Schmid G, Weiser E, Dorn H, Henschenmacher B, et al. The effect of exposure to radiofrequency electromagnetic fields on cognitive performance in human experimental studies: Systematic review and meta-analyses. Environ. Int. 2024, 191, 108899. DOI:10.1016/j.envint.2024.108899 [Google Scholar]
- Hu C, Zuo H, Li Y. Effects of radiofrequency electromagnetic radiation on neurotransmitters in the brain. Front. Public Health 2021, 9, 691880. DOI:10.3389/fpubh.2021.691880 [Google Scholar]
- United States Department of Defense, All-Domain Anomaly Resolution Office. Fiscal Year 2024 Consolidated Annual Report on Unidentified Anomalous Phenomena. Office of the Director of National Intelligence. 2024. Available online: https://www.dni.gov/files/ODNI/documents/assessments/DOD-AARO-Consolidated-Annual-Report-on-UAP-Nov2024.pdf (accessed on 24 March 2026).
- Hancock LJ, Porritt I, Grosvenor S, Cates L. UAP Activity Pattern Study 1945–1975 Military and Public Activities. Zenodo 2024. DOI:10.5281/zenodo.8213330 [Google Scholar]
- Hancock LJ, Porritt I, Grosvenor S. UAP Pattern Recognition Study 1945–1975 US Military Atomic Warfare Complex. Zenodo 2023. DOI:10.5281/zenodo.7295958 [Google Scholar]
- Grosvenor S, Hancock L, Porritt I. UAP Indications Analysis 1945–1975 United States Atomic Warfare Complex. Limina-J. UAP Stud. 2025, 2, 109–128. Available online: https://limina.scholasticahq.com/article/131854.pdf (accessed on 24 March 2026).
- Fox J. The Phenomenon [Documentary Film]; 1091 Pictures: New York, NY, USA, 2020. Available online: https://thephenomenonfilm.com/ (accessed on 24 March 2026).
- Knuth KH, Ailleris P, Agrama HA, Ansbro E, Budinger PA, Cai T, et al. The new science of Unidentified Aerospace-Undersea Phenomena (UAP). Prog. Aerosp. Sci. 2025, 156, 101097. DOI:10.1016/j.paerosci.2025.101097 [Google Scholar]
- Tedesco JJ, Tedesco GT. Eye on the sky: A UAP research and field study off New York’s Long Island coast. Open J. Appl. Sci. 2024, 14, 2267–2295. DOI:10.4236/ojapps.2024.148152 [Google Scholar]
- Szydagis M, Knuth KH, Kugielsky B, Levy C. Initial results from the first field expedition of UAPx to study unidentified anomalous phenomena. Prog. Aerosp. Sci. 2025, 156, 101099. DOI:10.1016/j.paerosci.2025.101099 [Google Scholar]
- McCampbell JM. UFO interference with vehicles and self-starting engines. In Proceedings of the MUFON 1983 UFO Symposium Proceedings, Pasadena, CA, USA, 1–3 July 1983; pp. 45–59. [Google Scholar]
- Heuser G, Heuser SA. Functional brain MRI in patients complaining of electrohypersensitivity after long-term exposure to electromagnetic fields. Rev. Environ. Health 2017, 32, 291–299. DOI:10.1515/reveh-2017-0014 [Google Scholar]