Attitudes to Aging and Emotional Well-Being Among Middle-Aged and Older Adults During the COVID-19 Pandemic in China: The Mediating Role of Emotion Regulation

Attitudes to Aging and Emotional Well-Being Among Middle-Aged and Older Adults During the COVID-19 Pandemic in China: The Mediating Role of Emotion Regulation
Received: 12 December 2025 Revised: 25 December 2025 Accepted: 16 March 2026 Published: 25 March 2026

© 2026 The authors. This is an open access article under the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
1. Introduction
The global population aged 60 and above is projected to account for 22% by 2050, highlighting the increasing significance of aging-related issues worldwide [1]. Individuals’ attitudes to aging (ATA) have been identified as a pivotal determinant in shaping the psychological well-being of middle-aged and older adults [2,3]. ATA are multidimensional and influence multiple life domains, including physical health, interpersonal relationships, and social-emotional functioning [4]. However, the COVID-19 pandemic has exacerbated psychological distress and negative affective states among this diverse demographic [5]. This is particularly concerning, as both middle-aged and older individuals have faced increasing age-related challenges, such as declining physical health, age discrimination, and disruptions to employment and social engagement [6,7]. Under these conditions, emotion regulation could become a fundamental ability in the process of social adaptation, helping maintain well-being. Given that ATA may be associated with the emotion regulation individuals employ, which in turn shape affective outcomes, examining emotion regulation as a potential mediator can provide valuable insights into the psychological mechanisms linking ATA to well-being during the pandemic.
1.1. Attitudes to Aging and Emotional Well-Being
The ATA refers to one’s feelings and perceptions of their own aging, encompassing both affective and cognitive representations [8]. Empirical studies have shown that positive attitudes toward aging are associated with more favorable and successful aging outcomes [9], whereas negative perceptions may exacerbate emotional reactivity to daily stressors [10] and increase the risk of mental illnesses [11]. While research has linked ATA to various mental health outcomes, a more comprehensive understanding of the multifaceted relationship between the positive attitudes to aging (PATA) and negative attitudes to aging (NATA) and mental health remains underexplored. The dual-factor model of mental health conceptualizes mental health as encompassing both positive and negative dimensions [12]. However, limited research has synthesized how PATA and NATA relate to the dual indicators of mental health within this framework. Recent studies have examined the validity of the dual-factor model in the context of older adults and found that PATA and NATA had opposite pathways on mental health outcomes [13,14]. Another study on older adults’ aging attitudes and sleep quality found distinct relationships between the two attitude types and sleep quality. PATA played a moderating role between stressful life events and sleep quality, while NATA mediated this association, further highlighting the complex relationships between the two attitude types and older adults’ well-being [15]. These align with similar results from previous studies [7,8], providing a valuable foundation for further in-depth research in this area.
The COVID-19 pandemic has exacerbated age stereotypes and ageism, potentially driving a shift toward more negative attitudes toward aging, particularly among older adults [10,16]. Compounding this dynamic, older adults faced substantially higher risks of severe illness and mortality from COVID-19 compared to younger and middle-aged groups, and they also reported greater anxiety in the face of pandemic-related stressors [16,17,18]. Interestingly, most research regarding ATA has focused on older adults, while paying less attention to middle-aged individuals. However, age-related loss experiences have been found to be associated with depressive symptoms in both middle-aged and older adults [19]. Moreover, age discrimination may increase aging anxiety through the internalization of self-perception about aging, resulting in subsequent negative consequences such as depression and loneliness, not only in older persons, but also in the middle-aged population [20]. These findings highlight the importance of investigating ATA patterns across middle-aged and older groups.
Emotional well-being has been defined as the affective part of subjective well-being [21], which is an essential indicator of quality of life [3] and healthy psychological functioning. Based on the dual-factor model of mental health [12], both positive affect (PA) and negative affect (NA) are considered key components of emotional well-being [22].
While prior studies suggest distinct roles for PATA and NATA in relation to mental health outcomes [2,12], the underlying psychological pathways linking ATA to emotional well-being remain unclear. Distinct patterns may also exist between middle-aged and older adult populations, as research indicates older adults tend to report more positive emotions and less anxiety compared to middle-aged individuals during the prolonged COVID-19 pandemic [18,23], despite being less influenced by optimism [24]. Investigating the relationship between emotional well-being and two types of ATA amid COVID-19 threats is therefore essential, as different attitudes may play distinct roles across middle-aged and older generations.
1.2. The Mediating Role of Emotion Regulation
How people manage their emotions through emotion regulation may be a crucial factor in understanding the associations between ATA and emotional well-being. Emotion regulation refers to the processes through which individuals modulate their emotions in response to external environments [25]. The capacity for effective emotion regulation is of paramount importance in fostering emotional well-being, particularly for those in the later stages of the life course [26,27,28].
Theoretical perspectives offer different predictions regarding age-related patterns in emotion regulation. On the one hand, the Socioemotional Selectivity Theory (SST) [25] and the Strength and Vulnerability Integration Model (SAVI) [29] both suggest that older adults tend to exhibit greater efficacy and efficiency in managing their emotions. SST posits that individuals’ social motivations are shaped by their perceptions of their remaining lifetime. When people perceive their future time as limited, they prioritize emotionally meaningful, satisfying social goals [25], which might explain why older adults display more positive emotions and adopt more adaptive strategies compared to younger adults [30]. SAVI emphasizes that older adults’ emotional well-being depends on whether they can avoid sustained, high-arousal negative stimuli. Age-related emotional advantages are evident when such stimuli are avoidable, but diminish or even vanish when they are unavoidable. Taken together, SST and SAVI suggest that older adults potentially be motivated to avoid arousal and experience more pleasant affect through emotion regulation during the COVID-19 pandemic [4,31].
On the other hand, recent theoretical advances, particularly the constructionist approach to emotional aging [32], emphasize that emotions are constructed by domain-general core systems and a conceptualization process that may remain relatively stable across adulthood. This perspective suggests that the fundamental psychological processes underlying emotional experiences may exhibit continuity rather than age-related differences. While older and middle-aged adults may differ in the frequency of specific strategies used [33,34], it remains unclear whether the mediating pathways through which ATA are linked to emotional well-being via emotion regulation are age-specific or consistent across age groups, particularly when facing health-threatening events.
Therefore, based on the dual-factor model of mental health [35], the present study aims to: (1) investigate whether adaptive and maladaptive emotion regulation strategies mediate the relationships between PATA and PA, NATA and NA, respectively; (2) employ moderated mediation analysis to test the age consistency of these mediating mechanisms across middle-aged and older populations.
2. Materials and Methods
2.1. Participants
The data were collected from 22 April to 24 April 2020, during the first wave of the COVID-19 pandemic in China. A web-link of the questionnaire was advertised on popular social network software in China, such as WeChat and QQ. A total of 7135 participants completed the self-report questionnaires. Participants were excluded from the data analysis if they: (1) failed the lie detector test, which comprised 3 items, by false responses over two times; (2) exhibited straight-lining responses; (3) completed the questionnaires in less than 100 s or more than one hour. There were 5546 participants left after exclusions. Based on the China Health and Retirement Longitudinal Study (CHARLS) [36], we included participants aged 45 and above in the current study. To examine potential life-stage differences, we adopted a group-comparison design, classifying participants into the middle-aged group (45–59 years old) and the older group (≥60 years). This classification aligns with the statutory definition of “elderly” in Chinese policy [37] and is commonly employed in gerontological and social science research [38,39]. This research was examined and approved by the Ethics Review Board of Central China Normal University. Written informed consent was obtained from all participants prior to study commencement.
2.2. Measures
2.2.1. Attitudes to Aging
Attitudes to Aging were measured with a shortened version of the Chinese version of Attitude to Ageing Questionnaire (C-AAQ) [40], with two conceptualized dimensions: PATA and NATA. Reducing the number of scale items has been recognized as a strategy to improve research efficacy [41,42]. Hence, we selected four items from the C-AAQ, each measured on a 5-point Likert scale (1 = totally disagree, 5 = totally agree). Two items were used to measure PATA (i.e., “As people getting older, they are better able to cope with life”, “It is a privilege to grow old”), while two items were used to measure NATA (i.e., “Old age is a time of loneliness”, “Old age is a depressing time of life”). Higher scores on the PATA subscale indicated more positive attitudes toward aging, whereas higher scores on the NATA subscale reflected more negative attitudes. In the middle-aged group, the correlation between the two PATA items was 0.50 (p < 0.001), while the correlation between the two NATA items was 0.50 (p < 0.001). In the older group, the correlations between the two PATA items and the two NATA items were 0.60 (p < 0.001) and 0.61 (p < 0.001), respectively.
2.2.2. Emotion Regulation
The Emotion Regulation Strategies Scale was used to measure the ways individual regulated their emotions during the peak of the national pandemic [43]. The instruments were explicitly framed within the pandemic context, such as “during the pandemic, how did you typically regulate and manage your emotions”. The scale consisted of 6 items, with reflection, reappraisal, social sharing, and distraction categorized as adaptive strategies; while rumination and expressive suppression were considered as maladaptive strategies [25,44]. Participants rated each item on a 5-point Likert scale ranging from 0 (not at all) to 4 (very much), with higher scores indicating greater frequency of strategy use. In the middle-aged group, the Cronbach’s alphas were 0.70 for adaptive emotion regulation, and the correlation was 0.31 (p < 0.001) between the two maladaptive emotion regulation items. In the older group, the Cronbach’s alphas were 0.70 for adaptive emotion regulation, and the correlation was 0.36 (p < 0.001) between the two maladaptive emotion regulation items.
2.2.3. Affect States
Items from the Positive and Negative Affect Schedule (PANAS) [45] were used to assess participants’ current affective states. To optimize measurement efficiency [41,42], positive affect (PA) was measured with four items (i.e., excited, energetic, calm, and relaxed). Similarly, negative affect (NA) was measured using four items (i.e., angry, worried, bored, and lonely). Participants rated each item on a five-point scale ranging from 1 (not at all) to 5 (extremely), resulting in separate measures of PA and NA. Higher scores indicated higher levels of PA and NA, respectively. In the middle-aged group, the Cronbach’s alphas were 0.77 for the PA subscale and 0.85 for the NA subscale. In the older group, the Cronbach’s alphas were 0.81 for the PA subscale and 0.84 for the NA subscale.
2.3. Data Analysis
Descriptive statistics and correlations for all variables included in the models were conducted using SPSS version 26.0. The mediating effects were assessed using the PROCESS version 3.3 with a bootstrap procedure, with 5000 bootstrapped samples drawn and 95% confidence intervals calculated [46]. First, the mediating role of emotion regulation was examined using Model 4 of the PROCESS macro program. Next, Model 59 of the PROCESS macro program was used to examine the age differences in the mediating mechanism, conditional indirect effects were estimated for each group separately. And the significance of age group differences was tested using the moderated mediation index. A Harman’s single factor test was performed to examine common method variance [47]. And variance inflation factors (VIFs) were examined to assess multicollinearity [48].
3. Results
3.1. Descriptive Statistics and Correlation Analysis
The Harman’s single-factor test revealed that the total variance for a single factor was 22.37%, which was lower than the 40% threshold, indicating that common method variance was not a significant issue in the present study [47]. Additionally, the VIFs for all predictor variables were below 2, suggesting that multicollinearity did not exist in our study [48].
The demographic characteristics of the study sample are presented in Table 1. Overall, 194 participants (29.71%) were aged 60 years and older, and 370 (56.67%) were male. The majority of the sample (82.54%) resided in urban areas, and 608 participants (93.11%) lived with others. Regarding self-rated health status, the proportions of subjects with good, moderate, and poor health levels were 53.60%, 38.28%, and 8.12%, respectively. All participants reported higher PATA (M = 3.17, SD = 0.96) than NATA (M = 2.68, SD = 1.07) (t = 8.858, p < 0.001), with higher PA (M = 3.28, SD = 0.83) than NA (M = 2.45, SD = 0.98). Noteworthy, older adults reported higher NATA, NA, and used more emotion regulation strategies than the middle-aged group. To clarify the specific differences between the two groups, we conducted further comparisons of discrete emotions and regulation strategies, with gender, marital status, health status, region, and residence types as covariates. Specifically, older samples reported slightly higher levels of calmness (F = 9.837, p = 0.002, η2 = 0.015) and boredom (F = 11.873, p = 0.001, η2 = 0.018) than middle-aged participants. They also used social sharing (F = 7.530, p = 0.006, η2 = 0.012), distraction (F = 9.323, p = 0.002, η2 = 0.014) and rumination (F = 5.354, p = 0.021, η2 = 0.008) somewhat more frequently for emotion regulation. Detailed demographics and specific differences for the two groups are provided in Supplementary Materials Table S1 and Table S2.
Table 1. Participants Characteristics and Associations with Primary Variables (N = 653).
|
Variables |
N |
PATA |
NATA |
AR |
MR |
PA |
NA |
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Mean (SD) |
F |
Mean (SD) |
F |
Mean (SD) |
F |
Mean (SD) |
F |
Mean (SD) |
F |
Mean (SD) |
F |
||||||||
|
Age (years) |
0.229 |
5.391 * (0.008) |
4.849 * (0.007) |
15.614 *** (0.023) |
3.441 |
18.858 *** (0.028) |
|||||||||||||
|
45–59 |
459 |
3.18 (0.95) |
2.61 (1.04) |
2.33 (0.75) |
1.66 (0.91) |
3.25 (0.84) |
2.34 (0.96) |
||||||||||||
|
60–76 |
194 |
3.14 (1.02) |
2.83 (1.14) |
2.47 (0.67) |
1.97 (0.90) |
3.38 (0.83) |
2.70 (0.97) |
||||||||||||
|
Gender |
4.082 * (0.006) |
2.449 |
0.416 |
16.656 *** (0.025) |
1.081 |
9.535 ** (0.014) |
|||||||||||||
|
Male |
370 |
3.18 (0.95) |
2.61 (1.04) |
2.33 (0.75) |
1.66 (0.91) |
3.25 (0.84) |
2.34 (0.96) |
||||||||||||
|
Female |
283 |
3.14 (1.02) |
2.83 (1.14) |
2.47 (0.67) |
1.97 (0.9) |
3.38 (0.83) |
2.70 (0.97) |
||||||||||||
|
Education |
1.823 |
2.199 |
0.28 |
0.217 |
0.48 |
1.147 |
|||||||||||||
|
primary |
29 |
3.03 (0.85) |
3.10 (1.19) |
2.31 (0.81) |
1.74 (0.91) |
3.27 (0.63) |
2.74 (0.81) |
||||||||||||
|
junior |
115 |
3.15 (1.03) |
2.67 (1.12) |
2.33 (0.73) |
1.82 (0.92) |
3.26 (0.78) |
2.48 (0.95) |
||||||||||||
|
senior |
253 |
3.12 (0.97) |
2.63 (1.06) |
2.36 (0.75) |
1.75 (0.93) |
3.27 (0.84) |
2.43 (0.97) |
||||||||||||
|
Undergraduate |
226 |
3.3 (0.93) |
2.63 (1.03) |
2.41 (0.71) |
1.74 (0.91) |
3.29 (0.88) |
2.38 (1) |
||||||||||||
|
Graduate |
30 |
2.92 (1.1) |
3.03 (1.22) |
2.39 (0.77) |
1.68 (0.86) |
3.48 (0.88) |
2.62 (1.11) |
||||||||||||
|
Marital status |
0.214 |
4.372 * (0.011) |
0.904 |
0.206 |
0.522 |
7.640 * (0.013) |
|||||||||||||
|
single |
39 |
3.10 (0.90) |
3.03 (1.19) |
2.26 (0.76) |
1.82 (0.8) |
3.38 (0.67) |
2.87 (0.88) |
||||||||||||
|
married |
614 |
3.18 (0.97) |
2.66 (1.06) |
2.38 (0.73) |
1.75 (0.93) |
3.28 (0.84) |
2.42 (0.98) |
||||||||||||
|
Health status |
3.728 * (0.011) |
10.032 *** (0.030) |
0.043 |
11.727 *** (0.035) |
5.979 ** (0.018) |
26.584 *** (0.076) |
|||||||||||||
|
① poor |
53 |
2.97 (0.98) |
③ > ① ③ > ② |
3.05 (1.07) |
① > ③ ② > ③ |
2.39 (0.69) |
2.17 (0.84) |
① > ② > ③ |
3.08 (0.84) |
③ > ① ③ > ② |
3.06 (0.99) |
① > ② > ③ |
|||||||
|
② moderate |
250 |
3.09 (0.88) |
2.83 (1.04) |
2.36 (0.67) |
1.87 (0.90) |
3.19 (0.79) |
2.64 (0.91) |
||||||||||||
|
③ good |
350 |
3.26 (1.02) |
2.51 (1.07) |
2.37 (0.78) |
1.61 (0.92) |
3.39 (0.85) |
2.22 (0.96) |
||||||||||||
|
Region |
0.243 |
4.376 * (0.007) |
0.204 |
9.205 ** (0.014) |
0.472 |
5.410 * (0.008) |
|||||||||||||
|
urban |
539 |
3.18 (0.96) |
2.64 (1.06) |
2.37 (0.73) |
1.71 (0.91) |
3.27 (0.84) |
2.41 (0.97) |
||||||||||||
|
rural |
114 |
3.13 (1.04) |
2.87 (1.12) |
2.4 (0.73) |
1.99 (0.92) |
3.33 (0.84) |
2.64 (1.02) |
||||||||||||
|
Residence types |
5.187 * (0.008) |
0.626 |
3.986 * (0.006) |
1.017 |
1.053 |
8.267 * (0.013) |
|||||||||||||
|
live alone |
45 |
2.86 (0.89) |
2.80 (1.25) |
2.16 (0.79) |
1.89 (0.79) |
3.16 (0.92) |
2.85 (0.92) |
||||||||||||
|
live with others |
608 |
3.20 (0.97) |
2.67 (1.06) |
2.39 (0.73) |
1.75 (0.93) |
3.29 (0.83) |
2.42 (0.98) |
||||||||||||
|
Monthly income |
2.881 |
0.777 |
2.029 |
1.246 |
1.382 |
0.278 |
|||||||||||||
|
0–5000 |
258 |
3.06 (0.95) |
2.62 (1.12) |
2.3 (0.69) |
1.69 (0.94) |
3.22 (0.82) |
2.42 (0.97) |
||||||||||||
|
5001–20,000 |
311 |
3.25 (0.94) |
2.69 (1.04) |
2.41 (0.74) |
1.81 (0.89) |
3.34 (0.8) |
2.46 (0.97) |
||||||||||||
|
20,000+ |
84 |
3.23 (1.11) |
2.79 (1.09) |
2.44 (0.81) |
1.79 (0.95) |
3.29 (0.99) |
2.50 (1.06) |
||||||||||||
Note: PATA = Positive attitudes to aging; NATA = Negative attitudes to aging; AR = Adaptive Emotion Regulation; MR = Maladaptive Emotion Regulation; PA = Positive Affect; NA = Negative Affect. * p < 0.05; ** p < 0.01; *** p < 0.001.
Means, standard deviations, and partial correlations among the study variables are shown in Table 2, with a few relevant demographic variables (age, gender, health status, marital status, and region) controlled. PATA were positively correlated with adaptive emotion regulation (r = 0.208, p < 0.001) and PA (r = 0.276, p < 0.001). NATA were positively correlated with maladaptive emotion regulation (r = 0.261, p < 0.001) and NA (r = 0.451, p < 0.001). Additionally, PA was negatively correlated with NA (r = −0.243, p < 0.001). Notably, PATA were not significantly correlated with NATA (r = 0.043, p = 0.261) or NA (r = 0.007, p = 0.832). Similarly, the associations between NATA and adaptive emotion regulation (r = 0.044, p = 0.281) or and PA (r = −0.037, p = 0.307) were not significant.
Table 2. Means, Standard Deviations, and Correlations Between the Variables (N = 653).
|
M ± SD |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
|
|---|---|---|---|---|---|---|---|---|---|
|
1. Positive attitudes to aging |
3.17 ± 0.97 |
1 |
|||||||
|
2. Negative attitudes to aging |
2.68 ± 1.07 |
0.043 |
1 |
||||||
|
3. Adaptive emotion-regulation |
2.37 ± 0.73 |
0.208 *** |
0.044 |
1 |
|||||
|
4. Maladaptive emotion-regulation |
1.76 ± 0.92 |
0.162 *** |
0.261 *** |
0.411 *** |
1 |
||||
|
5. Rumination |
1.77 ± 1.14 |
0.072 |
0.227 *** |
0.350 *** |
0.813 *** |
1 |
|||
|
6. Expressive suppression |
1.74 ± 1.11 |
0.191 *** |
0.194 *** |
0.312 *** |
0.800 *** |
0.302 *** |
1 |
||
|
7. Positive affect |
3.28 ± 0.84 |
0.276 *** |
−0.037 |
0.228 *** |
0.010 |
−0.052 |
0.071 |
1 |
|
|
8. Negative affect |
2.45 ± 0.98 |
0.007 |
0.451 *** |
0.040 |
0.342 *** |
0.289 *** |
0.263 *** |
−0.243 *** |
1 |
Note: M = Mean; SD = Standard Deviation. *** p < 0.001.
3.2. Mediation Model Analysis
The results of the mediation analyses are presented in Table 3. The first mediation model (Model 4 in PROCESS) was assessed, with PATA, adaptive emotion regulation strategies, and PA as the variables of interest, and health status as a covariate. PATA positively predicted adaptive emotion regulation (β = 0.162, p < 0.001) and PA (β = 0.205, p < 0.001). Additionally, adaptive emotion regulation positively predicted PA (β = 0.211, p < 0.001). The bias-corrected bootstrap procedure revealed a significant indirect effect of PATA on PA through adaptive emotion regulation (Effect = 0.034, 95% CI [0.018, 0.066]; accounting for 14.23% of the total effect), supporting the mediating role of adaptive emotion regulation in the link between PATA and PA among middle-aged and older adults (Figure 1).
A second mediation model (Model 4 in PROCESS) was then assessed to examine whether maladaptive emotion regulation mediated the relationship between NATA and NA among the two age groups, with gender, health status, living situation, marital status, and monthly household income per capita as covariates. The results showed that NATA positively predicted maladaptive emotion regulation (β = 0.222, p < 0.001) and NA (β = 0.342, p < 0.001). Maladaptive emotion regulation also positively predicted NA (β = 0.257, p < 0.001). The bias-corrected bootstrap procedure showed a significant indirect effect of negative ATA on NA through maladaptive emotion regulation (Effect = 0.057, 95% CI [0.037, 0.093]; accounting for 14.29% of the total effect), which also supported the mediating role of maladaptive emotion regulation between NATA and NA across both age groups (Figure 1).
Specifically, as previous research has argued that rumination and expressive suppression may manifest different emotional goals [44], a parallel mediation model (Model 4 in PROCESS) was additionally tested, with NATA as the independent variable, rumination and expressive suppression as parallel mediating variables, and NA as the dependent variable. Results showed that both indirect effects via rumination and expressive suppression were significant (Effect = 0.033, 95% CI [0.015, 0.056]; Effect = 0.024, 95% CI [0.009, 0.045]). Detailed information is provided in the Supplementary Materials Table S3.
Table 3. Summary of the Mediation Models.
|
Predictor |
Outcome |
SE |
β |
t |
p |
95% CI |
|---|---|---|---|---|---|---|
|
Positive attitudes to aging |
Adaptive emotion regulation |
0.029 |
0.162 |
5.566 |
<0.001 |
[0.105, 0.219] |
|
Positive attitudes to aging |
Positive affect |
0.033 |
0.205 |
6.303 |
<0.001 |
[0.141, 0.269] |
|
Adaptive emotion regulation |
Positive affect |
0.043 |
0.211 |
4.925 |
<0.001 |
[0.127, 0.295] |
|
Negative attitudes to aging |
Maladaptive emotion regulation |
0.032 |
0.222 |
6.943 |
<0.001 |
[0.159, 0.285] |
|
Negative attitudes to aging |
Negative affect |
0.031 |
0.342 |
11.004 |
<0.001 |
[0.281, 0.402] |
|
Maladaptive emotion regulation |
Negative affect |
0.037 |
0.257 |
6.988 |
<0.001 |
[0.185, 0.329] |
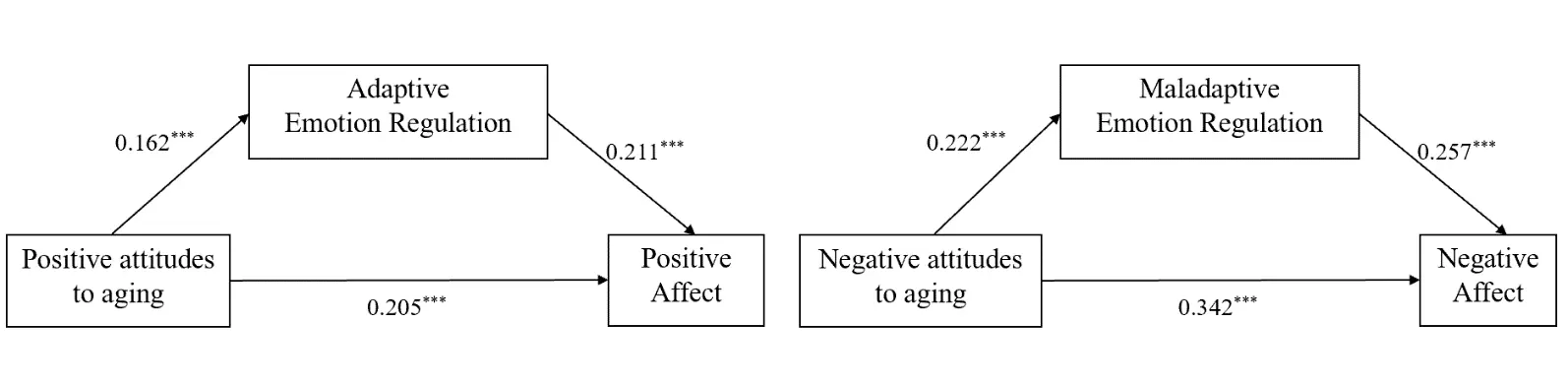
Figure 1. The mediation analysis of emotion regulation. Note: Path values are path coefficients. *** p < 0.001.
3.3. Moderated Mediation Analysis
As shown in Table 4, the moderated mediation model revealed that the interaction between PATA and age group on adaptive emotion regulation was not significant (β = −0.076, p = 0.217). The interactions between PATA and age group on PA (β = −0.070, p = 0.919), between adaptive emotion regulation and age group on PA were also not significant (β = −0.089, p = 0.366). Specifically, the conditional indirect effects showed a significant indirect effect in the middle-aged group (Effect = 0.042, 95% CI [0.019, 0.069]), while the indirect effect was not significant in the older group (Effect = 0.015, 95% CI [−0.007, 0.054]). The moderated mediation index was −0.027 (95% CI [−0.063, 0.019]), suggesting that age group did not significantly moderate this mediating pathway.
Similarly, none of the interactions between NATA and age group on maladaptive emotion regulation (β = 0.015, p = 0.825), NATA and age group on NA (β = −0.025, p = 0.703), or maladaptive emotion regulation and age group on NA were non-significant (β = 0.116, p = 0.149). The indirect effects were significant in both the middle-aged group (Effect = 0.047, 95% CI [0.021, 0.080]) and the older group (Effect = 0.077, 95% CI [0.034, 0.130]). The moderated mediation index was 0.030 (95% CI [−0.022, 0.090]), which was also non-significant, indicating that the mediating role of maladaptive emotion regulation was consistent across two age groups.
Table 4. Summary of Moderated Mediation Models.
|
Dependent Variable |
Path |
SE |
β |
t |
p |
95% CI |
|---|---|---|---|---|---|---|
|
Adaptive emotion regulation |
Positive attitudes to aging |
0.087 |
0.263 |
3.032 |
0.003 |
[0.093, 0.433] |
|
Age group |
0.063 |
0.143 |
2.286 |
0.023 |
[0.020, 0.266] |
|
|
Positive attitudes to aging × age group |
0.062 |
−0.076 |
−1.236 |
0.217 |
[−0.197, 0.045] |
|
|
Positive affect |
Positive attitudes to aging |
0.097 |
0.215 |
2.219 |
0.027 |
[0.025, 0.405] |
|
Adaptive emotion regulation |
0.131 |
0.313 |
2.394 |
0.017 |
[0.056, 0.570] |
|
|
Age group |
0.069 |
0.168 |
2.436 |
0.015 |
[0.033, 0.304] |
|
|
Positive attitudes to aging × age group |
0.069 |
−0.007 |
−0.101 |
0.919 |
[−0.142, 0.128] |
|
|
Adaptive emotion regulation× age group |
0.098 |
−0.089 |
−0.904 |
0.366 |
[−0.282, 0.104] |
|
|
Maladaptive emotion regulation |
Negative attitudes to aging |
0.095 |
0.200 |
2.102 |
0.036 |
[0.013, 0.386] |
|
Age group |
0.077 |
0.161 |
2.079 |
0.038 |
[0.009, 0.313] |
|
|
Negative attitudes to aging × age group |
0.067 |
0.015 |
0.222 |
0.825 |
[−0.116, 0.146] |
|
|
Negative affect |
Negative attitudes to aging |
0.093 |
0.373 |
4.022 |
0.001 |
[0.191, 0.555] |
|
Maladaptive emotion regulation |
0.109 |
0.104 |
0.951 |
0.342 |
[−0.111, 0.319] |
|
|
Age group |
0.073 |
0.098 |
1.342 |
0.181 |
[−0.046, 0.242] |
|
|
Negative attitudes to aging × age group |
0.065 |
−0.025 |
−0.382 |
0.703 |
[−0.153, 0.103] |
|
|
Maladaptive emotion regulation × age group |
0.080 |
0.116 |
1.444 |
0.149 |
[−0.042, 0.274] |
3.4. Supplementary Analyses
A series of supplementary analyses was conducted to examine the robustness and extensibility of the hypothesized models. First, we tested the reverse mediation model (i.e., adaptive emotion regulation mediated the association between NATA and NA, and maladaptive emotion regulation mediated the association between PATA and PA), and the results showed that all paths were not significant. The absence of significant indirect effects in these reverse models provided evidence for the discriminant validity of the dual-factor approach, demonstrating that positive and negative constructs are associated through distinct regulatory pathways rather than cross-domain associations. Second, we tested the moderating role of key demographic variables (age, health status, region, and gender) in the hypothesized models (Model 59 in PROCESS), and all moderating effects were not significant. This indicated that the mediating mechanism of emotional regulation between aging attitudes and affective states was relatively consistent across groups with different levels of health, gender, or residential backgrounds, and the age-related mediating pattern was robust. Detailed information is presented in the Supplementary materials Table S4 and Table S5.
4. Discussion
The current study investigated the mediating role of emotion regulation in the association between attitudes to aging and emotional well-being and examined the cross-age consistency of this mechanism among middle-aged and older adults during the COVID-19 pandemic. First, results revealed that compared to middle-aged adults, older adults reported slightly higher levels of NATA, boredom, and calmness, alongside a slightly higher overall frequency of emotion regulation strategies used. More importantly, the mediating role of emotion regulation manifested age-related consistency across the two age groups. Adaptive emotion regulation mediated the relationship between PATA and PA, whereas maladaptive emotion regulation mediated the link between NATA and NA.
The present study revealed a relatively consistent pattern of emotional well-being in both middle-aged and older adult participants. Specifically, both age groups reported a prevalent experience of positive affect despite the threats posed by the COVID-19 pandemic. Additionally, ATA was significantly associated with affective states in both age groups, which is consistent with previous research conducted during and before the pandemic [13,18,20,28]. In particular, PATA were linked to higher PA, while NATA were linked to higher NA. These findings are accordant with the dual-factor model of mental health, demonstrating that PATA and NATA have independent, parallel associations with emotional well-being [14,15]. Notably, age-related increases in negative attitudes toward aging (NATA) among older adults may stem from COVID-ageism [10,31], while their marginally higher levels of both calmness and boredom might suggest a shift toward lower-arousal emotional experiences consistent with SST [29]. They also employed social sharing, distraction, and rumination more frequently, likely as attempts to regulate this low-arousal emotional landscape [34,49].
Beneath these group differences, the two mediation models further supported the dual-factor model in our data, indicating that positive and negative pathways to well-being in midlife and later adulthood may operate concurrently, with relatively balanced regulatory efforts and emotional outcomes [35]. For the positive pathway, PATA may help individuals maintain better mood states and facilitate adaptive functioning, improving effective stress management by enhancing adaptive emotion regulation to deal with ongoing uncertainties and stresses [8,13,14]. For the negative pathway, individuals with NATA may have difficulties disengaging their attention from undesirable information (i.e., ageism, morality, economic recession) and even internalize stereotypical views [7], decreasing their self-regulation capacity for life management [13,15]. Importantly, however, the frequency differences in strategy use do not imply that the effectiveness or functional role of these strategies differs by age. The moderated mediation indices demonstrate that the functional pathways linking aging attitudes to emotional well-being through emotion regulation operate similarly in both age groups. This might align with the constructionist perspective on emotional aging [32]. While emotional strategies or momentary affect may vary across individuals and contexts, the underlying conceptualization systems that construct emotional experiences are relatively stable across adulthood.
It is noteworthy, however, that the indirect effects through emotion regulation accounted for approximately 14% of the total effects, indicating that the direct pathways from aging attitudes to emotional well-being were substantially stronger. This pattern suggests that aging attitudes exert a more direct and automated influence on emotional outcomes. As fundamental cognitive schemas, attitudes toward aging shape how individuals interpret age-related experiences, anticipate their future, and appraise daily events [11,18]. These influences likely operate through multiple systems, such as affective responses or meaning-making processes, which together contribute to the robust direct associations observed in our data. From a constructionist perspective, attitudes may function as part of the conceptual framework that individuals draw upon to construct emotional experiences [32], further explaining their potent direct effects. Given that direct and indirect pathways may represent different levels of psychological processing, future research should explore how these multiple mechanisms interact and whether their relative contributions differ across contexts or populations.
In summary, our findings demonstrate that emotion regulation mediates the relationship between attitudes to aging and emotional well-being in both middle-aged and older adults, and crucially, that these mediating pathways are consistent across age groups. Positive attitudes to aging foster positive affect through adaptive emotion regulation, while negative attitudes to aging exacerbate negative affect through maladaptive regulation. Therefore, interventions aimed at promoting the emotional well-being of middle-aged and older adults should emphasize both enhancing positive attitudes toward aging and mitigating negative perceptions of aging.
5. Limitations and Future Directions
There are several limitations that warrant consideration. First, the study relied on self-report measures to evaluate emotion regulation strategies and affect states. And emotion response data collected may have been restricted by specific items used in the assessment instrument [34]. In addition, the present findings did not differentiate between self-perceptions of aging and generalized aging stereotypes, suggesting that future research should incorporate more fine-grained measures of aging perceptions. Second, though the study identified plausible pathways linking aging attitudes, emotion regulation, and emotional well-being, the cross-sectional design precluded any causal conclusions. Third, no significant moderating effects of key demographic covariates were detected, which may also reflect limitations inherent to our sample, cross-sectional design, and measurement approach. Future research is warranted to delineate the boundary conditions of the current findings by examining other potential moderators, such as personality traits and specific health conditions. Fourth, the present findings must be interpreted within the specific cultural context of China, which may shape both aging attitudes and preferred emotion regulation strategies [50]. Caution should be exercised when generalizing the findings to other cultural backgrounds or groups. Future research should employ longitudinal or dynamic methods to explore how these associations unfold over time and across changing contexts, particularly during and after major life stressors.
6. Conclusions
This study provides novel evidence on the relationship between individuals’ attitudes to aging and their emotional well-being when facing threatening life events, and this psychological pattern exhibits cross-age consistency among middle-aged and older adults. Stressful events such as the COVID-19 pandemic may amplify differences in emotional experiences or strategy use, but do not alter the fundamental mechanisms linking aging attitudes to well-being. These core mechanisms operate similarly across the second half of life, underscoring the stability of fundamental associative patterns even in the face of adversity.
Statement of the Use of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this manuscript, the authors did not use any AI text-generation tools for drafting. In the final manuscript polishing stage, the authors used Deepseek to refine the article’s content and structure. Following the use of these tools, the author has thoroughly reviewed and edited the content and assumes full responsibility for the published material.
Supplementary Materials
The following supporting information can be found at: https://www.sciepublish.com/article/pii/926, Table S1: General Characteristics of the middle-aged group (N = 459) and the older group (N = 194). Table S2: General Characteristics of the emotion and strategies in two groups. Table S3: Results of the parallel mediation analysis. Table S4: Summary of the Opposite mediation models. Table S5: Moderation analysis of demographic variables (age, area and gender).
Author Contributions
Conceptualization, W.P., X.L. (Xiaoyu Lu) and X.L. (Xu Li); Methodology, W.P., X.L. (Xiaoyu Lu) and X.L. (Xu Li); Software, X.L. (Xiaoyu Lu), S.W. (Shuang Wang); Validation, S.W. (Sisi Wu); Formal Analysis, X.L. (Xiaoyu Lu); Investigation, L.D., J.W.; Resources, W.P.; Data Curation, Z.H.; Writing—Original Draft Preparation, W.P., X.L. (Xiaoyu Lu); Writing—Review & Editing, W.P., X.L. (Xiaoyu Lu) and X.L. (Xu Li); Visualization, S.W. (Sisi Wu); Supervision, W.P. and X.L. (Xu Li); Project Administration, W.P.; Funding Acquisition, W.P. and X.L. (Xu Li).
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Central China Normal University (protocol code CCNU-IRB-202002001b, date of approval: 15 February 2020).
Informed Consent Statement
Informed consent was obtained from all participants prior to their involvement in the study.
Data Availability Statement
Datasets of this study are available from the corresponding author on reasonable request.
Funding
This research was funded by the MOE (Ministry of Education in China) Project of Humanities and Social Sciences (24YJA19009), Key Laboratory of Adolescent Cyberpsychology and Behavior Central China Normal University (CCNU), Ministry of Education (CCNUCYPSYLAB2025A02) and the Natural Science Foundation of Hubei Province (2023AFB318).
Declaration of Competing Interest
The authors declare that they have no known financial or personal conflicts of interest that could have influenced the design, conduct, data analysis, or reporting of this research.
References
- UN Population Division. World Family Planning 2022: Meeting the Changing Needs for Family Planning: Contraceptive Use by Age and Method; United Nations: New York, NY, USA, 2022. Available online: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/files/documents/2023/Feb/undesa_pd_2022_world-family-planning.pdf (accessed on 11 January 2026).
- Yeung DY, Chung EK, Lam AH, Ho AK. Effects of subjective successful aging on emotional and coping responses to the COVID-19 pandemic. BMC Geriatr. 2021, 21, 128. DOI:10.21203/rs.3.rs-102941/v1 [Google Scholar]
- Charles ST, Rush J, Piazza JR, Cerino ES, Mogle J, Almeida DM. Growing old and being old: Emotional well-being across adulthood. J. Pers. Soc. Psychol. 2023, 125, 455–469. DOI:10.1037/pspp0000453 [Google Scholar]
- Kornadt AE, Kessler EM, Wurm S, Bowen CE, Gabrian M, Klusmann V. Views on ageing: A lifespan perspective. Eur. J. Ageing 2020, 17, 387–401. DOI:10.1007/s10433-019-00535-9 [Google Scholar]
- Choi SL, Lee YG. Financial hardship and change in emotional well-being before to during COVID-19 pandemic among middle-aged and older Americans: Moderating effects of internal coping resources. Soc. Sci. Med. 2023, 317, 115572. DOI:10.1016/j.socscimed.2022.115572 [Google Scholar]
- Infurna FJ, Gerstorf D, Lachman ME. Midlife in the 2020s: Opportunities and challenges. Am. Psychol. 2020, 75, 470–485. DOI:10.1037/amp0000591 [Google Scholar]
- Garrison-Diehn C, Rummel C, Au YH, Scherer K. Attitudes toward older adults and aging: A foundational geropsychology knowledge competency. Clin. Psychol. Sci. Pract. 2022, 29, 4–15. DOI:10.1037/cps0000043 [Google Scholar]
- Freeman AT, Santini ZI, Tyrovolas S, Rummel-Kluge C, Haro JM, Koyanagi A. Negative perceptions of ageing predict the onset and persistence of depression and anxiety: Findings from a prospective analysis of the Irish Longitudinal Study on Ageing (TILDA). J. Affect. Disord. 2016, 199, 132–138. DOI:10.1016/j.jad.2016.03.042 [Google Scholar]
- Long S, Laidlaw K, Lorimer A, Ferreira N. Attitudes to ageing and quality of life in young and old older adults: An international cross-sectional analysis. Work. Older People 2021, 25, 39–57. DOI:10.1108/WWOP-06-2020-0032 [Google Scholar]
- Wettstein M, Wahl HW. Trajectories of attitude toward own aging and subjective age from 2008 to 2020 among middle-aged and older adults: Partial evidence of a “COVID-19 effect”. Psychol. Aging 2021, 36, 790–805. DOI:10.1037/pag0000645 [Google Scholar]
- Brothers A, Kornadt AE, Nehrkorn-Bailey A, Wahl HW, Diehl M. The Effects of Age Stereotypes on Physical and Mental Health Are Mediated by Self-perceptions of Aging. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 845–857. DOI:10.1093/geronb/gbaa176 [Google Scholar]
- Suldo SM, Shaffer EJ. Looking beyond psychopathology: The dual-factor model of mental health in youth. Sch. Psychol. Rev. 2008, 37, 52–68. DOI:10.1080/02796015.2008.12087908 [Google Scholar]
- Chen YT, Gao XT, Chen ZL, Huang SH. Meaning in life and mental health of the elderly based on the dual-factor model: Mediating effects of attitudes toward aging. Stud. Psychol. Behav. 2022, 20, 88–95. DOI:10.12139/j.1672-0628.2022.01.013 [Google Scholar]
- Li Y, Chan WCH, Chen H, Ran M. Widowhood and depression among Chinese older adults: Examining coping styles and perceptions of aging as mediators and moderators. Aging Ment. Health 2022, 26, 1161–1169. DOI:10.1080/13607863.2021.1935455 [Google Scholar]
- Zhang D, Ruan H, Gao MG, Chen F, Li S. Stressful life events and subjectively rated sleep quality among older adults in China: The roles of positive and negative attitudes towards ageing. Ageing Soc. 2024, 44, 2116–2134. DOI:10.1017/S0144686X22001222 [Google Scholar]
- Wettstein M, Spuling SM, Wünsche J, Henning G. Middle-aged and older adults’ psychosocial functioning trajectories before and during the COVID-19 pandemic: Evidence for multidirectional trends. Psychol. Aging 2023, 38, 627–643. DOI:10.1037/pag0000760 [Google Scholar]
- Pearman A, Hughes ML, Smith EL, Neupert SD. Age Differences in Risk and Resilience Factors in COVID-19-Related Stress. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e38–e44. DOI:10.1093/geronb/gbaa120 [Google Scholar]
- Fu M, Guo J, Chen X, Han B, Ahmed F, Shahid M, et al. American Older Adults in COVID-19 Times: Vulnerability Types, Aging Attitudes, and Emotional Responses. Front. Public Health 2022, 9, 778084. DOI:10.3389/fpubh.2021.778084 [Google Scholar]
- Sabatini S, Wahl HW, Diehl M, Clare L, Ballard C, Brooker H, et al. Testing Bidirectionality in Associations of Awareness of Age-Related Gains and Losses with Physical, Mental, and Cognitive Functioning Across 1 Year: The Role of Age. J. Gerontol. B Psychol. Sci. Soc. Sci. 2023, 78, 2026–2036. DOI:10.1093/geronb/gbad150 [Google Scholar]
- Bergman YS, Segel-Karpas D. Aging anxiety, loneliness, and depressive symptoms among middle-aged adults: The moderating role of ageism. J. Affect. Disord. 2021, 290, 89–92. DOI:10.1016/j.jad.2021.04.077 [Google Scholar]
- Diener E, Oishi S, Lucas RE. Personality, culture, and subjective well-being: Emotional and cognitive evaluations of life. Annu. Rev. Psychol. 2003, 54, 403–425. DOI:10.1146/annurev.psych.54.101601.145056 [Google Scholar]
- Park CL, Kubzansky LD, Chafouleas SM, Davidson RJ, Keltner D, Parsafar P, et al. Emotional Well-Being: What It Is and Why It Matters. Affect. Sci. 2023, 4, 10–20. DOI:10.1007/s42761-022-00163-0 [Google Scholar]
- Carstensen LL, Shavit YZ, Barnes JT. Age Advantages in Emotional Experience Persist Even Under Threat From the COVID-19 Pandemic. Psychol. Sci. 2020, 31, 1374–1385. DOI:10.1177/0956797620967261 [Google Scholar]
- Pasion R, Paiva TO, Fernandes C, Barbosa F. The AGE Effect on Protective Behaviors During the COVID-19 Outbreak: Sociodemographic, Perceptions and Psychological Accounts. Front. Psychol. 2020, 11, 561785. DOI:10.3389/fpsyg.2020.561785 [Google Scholar]
- McRae K, Gross JJ. Emotion regulation. Emotion 2020, 20, 1–9. DOI:10.1037/emo0000703 [Google Scholar]
- DeSteno D, Gross JJ, Kubzansky L. Affective science and health: The importance of emotion and emotion regulation. Health Psychol. 2013, 32, 474–486. DOI:10.1037/a0030259 [Google Scholar]
- Barlow MA, Willroth EC, Wrosch C, John OP, Mauss IB. When daily emotions spill into life satisfaction: Age differences in emotion globalizing. Psychol. Aging 2023, 38, 644–655. DOI:10.1037/pag0000771 [Google Scholar]
- Wettstein M, Nowossadeck S, Vogel C. Well-being trajectories of middle-aged and older adults and the corona pandemic: No “COVID-19 effect” on life satisfaction, but increase in depressive symptoms. Psychol. Aging 2022, 37, 175–189. DOI:10.1037/pag0000664 [Google Scholar]
- Carstensen LL, Isaacowitz DM, Charles ST. Taking time seriously. A theory of socioemotional selectivity. Am. Psychol. 1999, 54, 165–181. DOI:10.1037/0003-066X.54.3.165 [Google Scholar]
- Charles ST. Strength and vulnerability integration: A model of emotional well-being across adulthood. Psychol. Bull. 2010, 136, 1068–1091. DOI:10.1037/a0021232 [Google Scholar]
- Whatley MC, Siegel ALM, Schwartz ST, Silaj KM, Castel AD. Younger and Older Adults’ Mood and Expectations Regarding Aging During COVID-19. Gerontol. Geriatr. Med. 2020, 6, 2333721420960259. DOI:10.1177/2333721420960259 [Google Scholar]
- Mikkelsen MB, O’Toole MS, Gutchess A. The Constructionist Approach to Emotional Aging: Theoretical Insights and Predictions. J. Gerontol. Ser. B 2022, 77, 1571–1579. DOI:10.1093/geronb/gbac048 [Google Scholar]
- Whitmoyer P, Fisher ME, Duraney EJ, Manzler C, Isaacowitz DM, Andridge R, et al. Age differences in emotion regulation strategy use and flexibility in daily life. Aging Ment. Health 2024, 28, 330–343. DOI:10.1080/13607863.2023.2256245 [Google Scholar]
- Livingstone KM, Isaacowitz DM. Age and emotion regulation in daily life: Frequency, strategies, tactics, and effectiveness. Emotion 2021, 21, 39–51. DOI:10.1037/emo0000672 [Google Scholar]
- Bonneville-Roussy A, Laberge F. Stability and Change in Mental Health Profiles from Middle Adulthood to Very Old Age. Clin Gerontol. 2024, 1–15. DOI:10.1080/07317115.2024.2329150 [Google Scholar]
- Chen X, Wang Y, Strauss J, Zhao Y. China health and retirement longitudinal study (CHARLS). In Encyclopedia of Gerontology and Population Aging; Gu D, Dupre ME, Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 948–956. [Google Scholar]
- Law of the People’s Republic of China on the Protection of the Rights and Interests of the Elderly. Available online: https://www.gov.cn/guoqing/2021-10/29/content_5647622.htm (accessed on 11 January 2026).
- Shi JM, Liu XT. The Effects of Intergenerational Supports on Depressive Symptoms for Older Adults: The Mediate Effect of Attitude toward Ageing and The Moderate Effect of Urban-Rural Disparity. J. Psychol. Sci. 2024, 47, 695–702. DOI:10.16719/j.cnki.1671-6981.20240323 [Google Scholar]
- Liu D, Xi J, Hall BJ, Fu M, Zhang B, Guo J, et al. Attitudes toward aging, social support and depression among older adults: Difference by urban and rural areas in China. J. Affect. Disord. 2020, 274, 85–92. DOI:10.1016/j.jad.2020.05.052 [Google Scholar]
- Huang YF, Wang DH, Liu YG, Laidlaw K. Application of Attitudes to Aging Questionnaire (AAQ) among Chinese Aged Adults. Chin. J. Clin. Psychol. 2010, 18, 447–450. DOI:10.16128/j.cnki.1005-3611.2010.04.021 [Google Scholar]
- Rammstedt B, Beierlein C. Can’t we make it any shorter? The limits of personality assessment and ways to overcome them. J. Individ. Differ. 2014, 35, 212–220. DOI:10.1027/1614-0001/a000141 [Google Scholar]
- Pan W, Zhou W, Wu J, Huang Z, Ding L, Guo L, et al. The effect of exposure to COVID-19 on life satisfaction: The mediating role of hyperarousal and moderating/mediating role of affective forecasting. J. Affect. Disord. 2023, 337, 1–10. DOI:10.1016/j.jad.2023.05.062 [Google Scholar]
- Brans K, Koval P, Verduyn P, Lim YL, Kuppens P. The regulation of negative and positive affect in daily life. Emotion 2013, 13, 926–939. DOI:10.1037/a0032400 [Google Scholar]
- Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. DOI:10.1016/j.cpr.2009.11.004 [Google Scholar]
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. DOI:10.1037/0022-3514.54.6.1063 [Google Scholar]
- Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Perspective; 2nd ed.; The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. DOI:10.1037/0021-9010.88.5.879 [Google Scholar]
- Kim JH. Multicollinearity and misleading statistical results. Korean J. Anesthesiol. 2019, 72, 558–569. DOI:10.4097/kja.19087 [Google Scholar]
- Scheibe S, English T, Tsai JL, Carstensen LL. Striving to feel good: Ideal affect, actual affect, and their correspondence across adulthood. Psychol. Aging 2013, 28, 160–171. DOI:10.1037/a0030561 [Google Scholar]
- Tamir M, Ito A, Miyamoto Y, Chentsova-Dutton Y, Choi JH, Cieciuch J, et al. Emotion regulation strategies and psychological health across cultures. Am. Psychol. 2024, 79, 748–764. DOI:10.1037/amp0001237 [Google Scholar]