1. Introduction
Myocardial fibrosis is a hallmark of several cardiovascular diseases (CVDs) including dilated cardiomyopathy (DCM), and is characterised by an aberrant over-production of various extracellular matrix (ECM) proteins, primarily collagen [
1,
2]. Fibrosis results from a failed wound-healing response to tissue injury [
3], and is exacerbated in the heart due to its poor regenerative capacity, which renders any form of myocardium damage susceptible to heart failure (HF) [
4]. DCM is typically defined as left ventricular (LV) dilation and systolic dysfunction, which results in an impaired ability of the heart to effectively pump blood to other parts of the body, and is the most commonest cause of HF with reduced ejection fraction (HFrEF) [
5]. DCM is often undiagnosed but has been reported to affect 1:250–1:400 up to 1:2500 of the general population [
5,
6], and can affect individuals of all ages and races. However, males are at a greater risk of disease exposure compared to their females counterparts [
7]. There are no specific treatments for DCM. Many available therapies used to treat cardiomyopathies fail to effectively resolve, let alone attenuate the multifactorial nature of fibrosis and hence, mainly provide symptomatic management of disease progression [
8]. Hence, there is an urgent need to better understand the pathophysiology of DCM, to develop more direct anti-fibrotic therapies that are safe.
There are various animal models that have been established to better understand the pathophysiology of DCM-induced myocardial fibrosis and related HF [
9,
10], and/or test novel therapies for the disease, most notably via surgically-induced myocardial infarction (MI) or ischemia [
11,
12]/ischemia-reperfusion injury [
13]. Temporary or permanent obstruction of blood flow from the left coronary artery/and the reperfusion-induced restoration of blood flow leads to significant structural and functional damage to the myocardium, which leads to the rapid onset of HF. However, whilst these models can be consistently established in both rodent [
11,
12] and larger [
14,
15] animal models, the invasive nature of the procedures involved often lead to ~10–40% mortality rates post-surgery [
12], which can vary depending on the species and strain of animal used, the surgical skills of the operator and/or the infarct size that develops post-MI.
To overcome this, a non-surgical means of injecting isoproterenol (or isoprenaline; ISO) to rats was found to induce myocardial lesions, over 60 years ago [
16,
17]. ISO is a synthetic catecholamine and -adrenergic agonist, that causes severe oxidative stress in the myocardium, resulting in infarct-like necrosis of the heart muscle [
18]. When administered via a single injection (at doses of 1–100 mg/kg), ISO induces myocardial necrosis within 24 hours [
19,
20] and myocardial fibrosis after 2–3 weeks [
21]. This degree of fibrosis as well as some animal mortality (due to ISO-induced cardiac arrhythmia or hemodynamic changes) can be increased by the dosing and frequency of ISO administration [
18,
20,
22,
23,
24], but can also be affected by the age and strain of the species employed, particularly in mice [
22,
23,
24,
25]. To this extent, Brooks and Conrad [
22] demonstrated that once-daily subcutaneous (s.c) injections of ISO (100 mg/kg/day) to 8-month old male Swiss-Webster mice for five consecutive days led to significantly increased left ventricular (LV) cardiomyocyte hypertrophy, fibrosis and limited animal mortality (1/15 mice; ~7%) after 14-days. However, these mice underwent diastolic dysfunction (elevated LV diastolic pressure) rather than any marked systolic dysfunction. On the other hand, when applied to 8–10 week-old male 129sv mice, which are more sensitive to MI-induced LV rupture [
26] and related mortality [
27], ISO had to be s.c-injected for five consecutive days at a lower dose of 25 mg/kg for a large proportion of animals to survive (35/50 survived; 30% mortality rate [
25]), but was able to induce several features of DCM including LV inflammation, oxidative stress, cardiomyocyte hypertrophy, remodelling, fibrosis and systolic dysfunction (reduced ejection fraction, fractional shortening and global longitudinal strain rate) after 14-days in mice that survived the procedure [
25]. This pointed to the fact that strain-dependent sensitivity to myocardial injury could influence the structural and functional outcomes, as well as the mortality of the ISO-induced model of DCM. To this extent, whilst mouse strain-dependent differences in LV hypertrophy [
28], fibrosis [
29] and dysfunction [
30] to various stressors, and the myocardial wound-healing response to MI [
31] have previously been documented, the impact of mouse strain on the myocardial fibrosis that develops in the ISO-induced model of DCM has not been evaluated.
Hence, in this study, we compared the impact of this repeated ISO (25 mg/kg)-induced protocol in equivalently-aged adult 129sv mice and more commonly accessible strains, namely C57BL/6J and FVB/N mice. Notably, the C57BL/6 strain is also the background strain for the majority of mutant mouse models that have been established [
32]. However, given that C57BL/6J mice were more resistant to myocardial injury and related fibrosis compared to their 129sv counterparts, we also determined whether administering higher doses of ISO (50 or 100 mg/kg) to age-equivalent C57BL/6J mice could induce a similar phenotype to that observed in 129sv mice given the lower dose (25 mg/kg) of ISO over five consecutive days.
2. Materials and Methods
2.1. Materials
Isoproterenol (isoprenaline hydrochloride) was purchased from Sigma-Aldrich (I5627; St. Louis, MO, USA). Arrane (Isoflurane) was supplied by Baxter Healthcare (Toongabbie, NSW, Australia).
2.2. Animals
8–12-week old male 129sv mice (provided by the Animal Resource Centre, Perth, Western Australia, Australia), C57BL/6J and FVB/N mice (provided by the Monash Animal Research Platform (MARP), Monash University, Clayton, Victoria, Australia) were allowed to acclimatize (in groups of 2–3 mice per cage) for at least 6–7 days prior to experimentation and were maintained on a 12 h light:12 h dark cycle with free access to standard rodent chow (Barastoc Stockfeeds, Pakenham, Victoria, Australia) and water. Male mice were used as they are more prone to cardiomyopathy-induced HF [
7,
33]. The experiments outlined were approved by the Animal Ethics Committee of Monash University (under MARP/2012/049 or MARP/2023/37326), which adheres to the Australian Code of Practice for the Care and Use of Laboratory Animals for Scientific Purposes.
2.3. Induction of the ISO-induced Model of Myocardial Fibrosis in Mice
The non-surgical ISO-induced model of cardiomyopathy was employed [
22,
25] in age-matched adult 129sv, C57BL/6J and FVB/N mice, to evaluate the impact of mouse strain on the myocardial injury-induced fibrosis that developed after 14-days. Once acclimatised, each strain of mice (
n = 5 per group) were given once-daily subcutaneous (s.c) injections of ISO (25 mg/kg body weight (BW) over 5 consecutive days, then left for a further 9-days for fibrotic healing to occur in the myocardium (given the poor regenerative capacity of the mammalian heart [
34]). In each case, separate sub-groups of each mouse strain (
n = 5 per group) were given once-daily injections of saline (the vehicle for ISO) over 5 consecutive days, and then also left for a further 9-days (as the respective control groups).
In a separate set of experiments, male C57BL/6J mice were s.c-injected with increasing doses of ISO: 25 mg/kg (
n = 8), 50 mg/kg (
n = 11) or 100 mg/kg (
n = 11) BW;
n = 11 per group); or saline (
n = 8), once-daily for 5 consecutive days, then left for a further 9-days for fibrotic healing to occur in the myocardium. A higher number of C57BL/6J mice given the intermediate (50 mg/kg) and higher (100 mg/kg) dose of ISO were incorporated into this latter study, to account for expected animal mortality.
2.4. Echocardiography
As LV functional parameters were previously assessed by transthoracic echocardiography in 129sv mice subjected to the repeated administration of ISO (25 mg/kg) detailed above (at day-14 post-injury) [
25], echocardiography was only performed on male C57BL/6J mice repeatedly injected with saline or increasing doses of ISO (25–100 mg/kg), at the corresponding 14-day time-point. Measurements were performed on mice anaesthetised with Aerrane (isoflurane; 2–3% in oxygen, by inhalation via a nose cone; Baxter Healthcare, Toongabbie, New South Wales, Australia), using a Vevo 2100 ultrasound system (VisualSonics, Toronto, Canada; housed at the Monash Biomedical Imaging Facility) utilising an ultra-high frequency 30 MHz linear-array transducer for imaging of mouse cardiac function; as detailed previously [
25]. Measures of LV function and myocardial stiffness were determined, as reported before [
25].
2.5. Tissue Collection and Analysis
Following the functional assessment of mice at day-14 post-ISO-induced injury, all mice were weighed and then killed with an overdose of anaesthetic (Aerrane (Isoflurane; Baxter Healthcare, Brunswick, VIC, Australia); 5% in oxygen, by inhalation). The heart and then left ventricle (LV) were isolated from all animals. LV tissues were transversely divided into 3 portions: the apical region for measuring hydroxyproline content, the midzone for fixation in 10% neutral buffered formalin, and the basal region. Unfixed tissue was immediately snap frozen in liquid nitrogen and stored at −80 °C. To ensure standardization and enable intergroup comparisons, each assay used the same portion of LV tissue from each animal.
2.6. Hydroxyproline Analysis
The LV apical portion of each mouse was processed as described before [
35] for the measurement of hydroxyproline content. Briefly, LV apical samples were lyophilized to dry weight (for dry weight measurement), rehydrated and hydrolysed in 6M hydrochloric acid (HCl). LV hydrolysates were then assayed in duplicate against a standard curve of purified trans-4-hydroxy-L-proline (Sigma-Aldrich, Richmond, CA, USA). Total collagen content was then extrapolated from the hydroxyproline values determined [
35], and in turn, were divided by the dry weight of each corresponding tissue to yield percent collagen content per dry weight tissue (collagen concentration).
2.7. Histological Analysis
Given the variable levels of LV fibrosis that were detected from the different strains of mice by hydroxyproline analysis, histological analysis of interstitial LV fibrosis was only determined from 129sv and C57BL/6J mice. Formalin-fixed and embedded LV sections were cut into serial (5 µm) sections, and stained with 0.1% picrosirius red (Polysciences, Inc, Warrington, PA, USA) to identify interstitial fibrillar collagen, as detailed previously [
23,
25]. Whole LV sections were captured using the Aperio AT Turbo scanner (Leica Biosystems, Nussloch, Germany) and stored as digital high-resolution images on a local server associated with the instrument. Images were viewed and morphometrically analysed with the Aperio ImageScope v12.1.0.5029 software (Leica Biosystems).
2.8. Statistical Analysis
All data are expressed as the mean ± standard deviation of mean (SD), and were statistically analysed using GraphPad Prism v9.0.1 (GraphPad Software Inc, San Diego, CA, USA), on group sizes of at least
n = 5. The data were analysed by a one-way ANOVA followed by a Tukey’s post-
hoc test to allow for multiple comparisons between the groups analysed. No approaches were used to reduce unwanted sources of variation by data normalization or to generate normal data. Differences were considered statistically significant at
p < 0.05 and the threshold value was not varied during the study.
3. Results
3.1. The Impact of Mouse Strain on ISO-induced Myocardial Fibrosis
All mice from each strain evaluated, that were injected with saline (
n = 5/5 per strain) or 25 mg/kg ISO (
n = 5/5 per strain) survived the 14-day protocol. Adult (8–12-week old) 129sv, C57BL/6J and FVB/N mice subjected to repeated saline (vehicle)-injections presented with a similar LV collagen concentration (collagen content per dry weight tissue) of ~0.50–0.55% at day-14 (9 days after the fifth injection), as determined by hydroxyproline analysis (A). However, when age-matched counterparts were subjected to repeated ISO (25 mg/kg) administration, 129sv, C57BL/6J and FVB/N mice presented with significantly elevated LV collagen concentration levels of 1.52%, 0.95% and 0.67%, respectively, at day-14 post-injury. This corresponded to a ~2-fold, ~0.7-fold and ~0.3-fold increase, respectively, at the time-point studied over respective levels measured in their saline-injected counterparts (all
p < 0.001 vs the strain-respective saline-injected group; A). The levels of LV collagen concentration measured in ISO-injured C57BL/6J mice were significantly greater than that measured in ISO-injured FVB/N mice (
p < 0.01 vs ISO-injured FVB/N mice), and in turn, the levels of LV collagen concentration measured in ISO-injured 129sv mice were markedly greater than that measured in C57BL/6J or FVB/N mice (
p < 0.001 vs both ISO-injured C57BL/6J or FVB/N mice; A).
. The effects of repeated ISO (25 mg/kg body weight) administration on myocardial fibrosis in different mouse strains. (A) Shown is the mean ± SD LV % collagen content per dry weight tissue (% LV collagen concentration; as a measure of fibrosis) in adult 129sv, C57BL/6J and FVB/N mice injected with saline or ISO at day-14 post-injury. (B) Representative images of picrosirius red-stained LV (midzone) tissue sections from adult 129sv and C57BL/6J mice injected with saline or ISO, show the histological extent of interstitial LV collagen deposition and distribution (fibrosis) in each strain at day-14 post-injury. Also shown is the mean ± SD % interstitial LV collagen deposition (per fractional area stained) in each of the groups evaluated. In each case, the data were obtained from n = 5 mice per group; where the white circles within each bar represent individual data points for each animal analysed per group. ∗ p < 0.05, ∗∗ p < 0.01, ∗∗∗ p < 0.001 vs the respective group compared.
Given the modest increase in myocardial collagen concentration that was detected in ISO-injured FVB/N mice (A), ISO-induced changes in interstitial LV collagen deposition were only further examined histologically in 129sv and C57BL/6J mice, by morphometric analysis of picrosirius red-stained tissue sections from the LV midzone (B). Saline-injected 129sv and C57BL/6J mice presented with interstitial LV collagen levels of 1–2% of the fractional area stained (B). Comparatively, age-matched 129sv and C57BL/6J mice subjected to repeated ISO (25 mg/kg)-administration presented with interstitial LV collagen levels of ~17% and 2.2% of the fractional area stained, respectively, at day-14 post-injury. This represented a ~7-fold and ~1-fold increase in interstitial collagen deposition, respectively, at the time-point studied over respective levels measured in their saline-injected counterparts (both
p < 0.01 vs the strain-respective saline-injected group; B). The magnitude of the changes seen in interstitial LV collagen deposition (B) was greater than that seen by hydroxyproline analysis (A), which is consistent with findings from other studies conducted in the ISO model [
23,
25] and other models [
36] of heart disease characterised by myocardial fibrosis. A number of factors may contribute to these discrepant findings, which include scale (extrapolation of a single tissue section area compared to the volume of apical tissue assessed by hydroxyproline analysis); correction for dry weight (biochemical analysis accounts for hypertrophy and atrophy, whereas histological analysis does not); the extent to which fine collagen fibres can be detected; and a tendency for picrosirius red-staining to overestimate collagen [
37]. Nevertheless, the findings from both the biochemical (A) and histological (B) analysis of LV fibrosis in these strains of mice determined that 129sv mice were more prone to ISO-induced myocardial fibrosis compared to their age-matched C57BL/6J and FVB/N counterparts.
3.2. The Impact of Higher Doses of ISO Administration on Myocardial Fibrosis and Related Dysfunction in C57BL/6J Mice
To determine if the severity of the ISO (25 mg/kg)-induced myocardial fibrosis measured in 129sv mice could be provoked by higher doses of ISO (50 or 100 mg/kg) administration to C57BL/6 mice, adult (8–12-week old) C57BL6J mice were subjected to repeated saline or ISO (25, 50 or 100 mg/kg) injections and maintained until day-14 post-injury (9-days after the fifth ISO injection). Notably, although all
n = 8/8 saline-injected and
n = 8/8 low-dose ISO (25 mg/kg)-injected mice survived the 14-day protocol, only
n = 5/11 mice injected with 50 mg/kg ISO and
n = 6/11 mice injected with 100 mg/kg ISO survived the experimental period; indicating that higher doses of ISO administered to C57BL/6J mice could induce up to ~50% mortality.
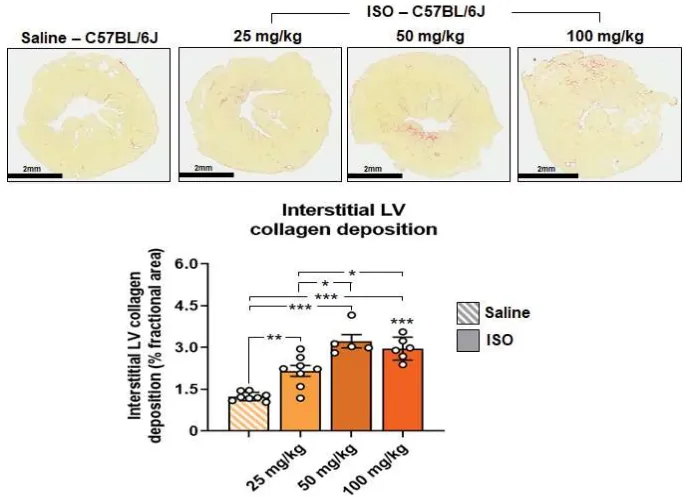
Given the increased sensitivity of detecting interstitial LV collagen deposition by histological means, only the morphometric analysis of picrosirius red-stained interstitial collagen was performed in this follow-up study. Compared to the interstitial LV collagen deposition measured in saline-injected mice (1.2% of the fractional area stained), ISO-injected mice presented with 2.15%, 3.2% and 3.0% of the fractional area stained at day-14 post-injury, when administered with 25, 50 and 100 mg/kg, respectively (all
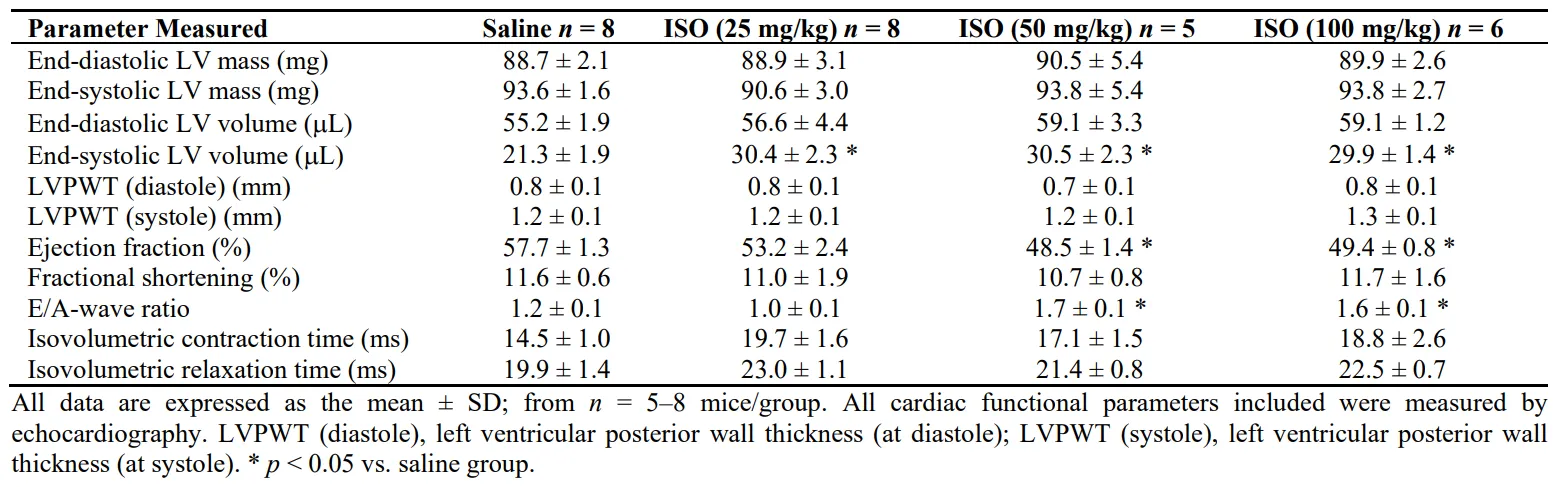
p < 0.01 vs the level measured in saline-injected control mice; ). This represented a ~1-fold, ~1.6-fold and ~1.4-fold increase in interstitial LV fibrosis, respectively, at the time-point studied over respective levels measured in the saline-injected control group. Interestingly, although the administration of higher doses of ISO induced increased mortality of C57BL/6J mice, they also caused some LV systolic dysfunction in the mice that survived the 14-day experimental period, as determined by echocardiography (). When injected at 50 or 100 mg/kg body weight, ISO-injured C57BL/6J mice had significantly reduced LV ejection fraction and significantly increased end-systolic LV volume, with a trend towards an increase in end-diastolic LV volume. These higher doses of ISO also induced a significant increase in E/A-wave ratio (of ~1.6–1.7; indicative of borderline diastolic dysfunction) in C57BL/6J mice (), which would be considered to be just above the normal range; and a trend towards an increased isovolumetric contraction (IVCT) and relaxation (IVRT) time (), indicative of these mice having stiffened hearts. The LV dysfunction measured in C57BL/6J mice, however, was still not as severe as that measured in 129sv mice given repeated ISO administration at a lower dose (25 mg/kg) at day-14 post-injury [
25].
. The effects of increasing doses of ISO administration on myocardial fibrosis in C57BL/6J mice. Representative images of picrosirius red-stained LV (midzone) tissue sections, from adult C57BL/6J mice injected with saline or ISO (25, 50 or 100mg/kg body weight), show the histological extent of interstitial LV collagen deposition and distribution (fibrosis) at day-14 post-injury. Also shown is the mean ± SD % interstitial LV collagen deposition (per fractional area stained) in each of the groups evaluated. In each case, the data were obtained from n = 5–8 mice per group; where the white circles within each bar represent individual data points for each animal analysed per group. ∗ p < 0.05, ∗∗ p < 0.01, ∗∗∗ p < 0.001 vs the respective group compared.
. Cardiac functional parameters from ISO-injured C57BL/6J mice.
4. Discussion
In line with previous studies which have identified strain-dependent effects on the severity of LV fibrosis and dysfunction in murine models of CVD [
29,
30], this study identified that the intensity of ISO-induced myocardial fibrosis and related dysfunction in mice is also strain-dependent. Adult 129sv mice subjected to repeated ISO (25 mg/kg) administration underwent a more marked progression of LV collagen concentration and interstitial LV collagen deposition after 14-days of injury, compared to that measured in age-matched C57BL/6 and FVB/N mice. These findings are consistent with other studies demonstrating that 129sv mice are more sensitive to MI-induced LV rupture [
26] and related mortality [
27], whereas C57BL/6J mice are more resistant to cardiac and renal fibrosis [
29]. Although FVB/N mice were also reported to be resistant to hepatic fibrosis [
29], the current study showed that FVB/N mice are even more resistant to ISO-induced myocardial fibrosis compared to their 129sv and C57BL/6J counterparts (). When higher doses of ISO (50 or 100 mg/kg) were repeatedly administered to C57BL/6J mice, these mice were more susceptible to ISO-induced mortality, underwent a modest increase in interstitial LV fibrosis, but also underwent some LV systolic dysfunction (reduced ejection fraction which correlated with an increased end-systolic LV volume and a trend towards an increased end-diastolic LV volume) after 14-days of injury. Furthermore, C57BL/6J mice subjected to repeated 50 or 100 mg/kg ISO underwent an increased LV E/A-wave ratio, suggestive that these sub-groups of mice had borderline diastolic dysfunction, although this elevated ISO-induced E/A-wave ratio would be considered just above the upper limit of the normal range. Despite this, C57BL/6J mice subjected to repeated higher dosing of ISO still did not undergo the degree of insterstitial LV fibrosis or dysfunction [
25] detected in 129sv mice given a lower dose (25 mg/kg) over 5 consecutive days.
It is now well-recognised that the genetic composition of the various mouse strains commonly used for scientific research purposes underscores how sensitive or resistant each strain is to tissue injury/disease in general, and CVD in particular [
29,
30]. 129s(v) mice have been reported to possess higher vascular tensile stiffness and are less responsive to acetylcholine-induced vasorelaxation [
38], but are more susceptible to MI-induced vascular rupture [
26], owing to this strain of mice having high levels of LV gelatinase activity that destabilise the tensile strength of the infarcted myocardium post-MI. Furthermore, 129sv mice have two renin genes (compared to C57BL/6 mice only having one) [
39], which makes them more prone to undergoing hypertension and associated myocardial hypertrophy and fibrosis [
40]. Comparatively (to C57BL/6 mice), 129sv mice had higher baseline levels of interstitial LV collagen deposition (~1.5–3% of the fractional area stained), and ~15–25% of the fractional area stained when subjected to repeated ISO (25 mg/kg) administration [
25]; B). This in turn led to these mice undergoing significant systolic dysfunction (reduced ejection fraction, fractional area and abnormal global longitudinal strain rate in conjunction with increased end-systolic volume; which results from an increased LV afterload post-MI), an E/A-wave ratio of ~3 (indicative of an elevated filling pressure in an abnormal heart) and myocardial stiffness (which led to these mice undergoing significantly increased isovolumetric contraction and relaxation time compared to their saline-injected counterparts) in response to repeated ISO (25 mg/kg) administration [
25]. Notably though, the increased sensitivity of these mice to CVD and related mortality [
27], led to higher doses of ISO administration to these mice (50 or 100 mg/kg over 5 consecutive days) causing significantly increased mortality (unpublished findings by C. S. Samuel). However, the heightened levels of LV fibrosis and dysfunction that can be measured in this strain of mice (along with the increased LV inflammation, oxidative stress, cardiomyocyte hypertrophy and remodelling these mice present with post-ISO (25 mg/kg) administration [
25]) makes them an ideal choice to be utilised for scientific investigations that aim to evaluate the pathological consequences of DCM and/or the testing of various therapies that can be employed to treat the disease. However, this strain of mouse is not always as readily available as other more commonly utilised mouse strains.
To address this, we determined if more accessible murine strains such as C57BL/6J and FVB/N mice could undergo the same levels of LV fibrosis and dysfunction as their 129sv counterparts, particularly when given higher doses of ISO (to account for these more commonly accessible strains being more resistant to cardiac injury and related LV fibrosis [
34]; ). However, as reported, we found that even when consecutively administered at higher doses (50 or 100 mg/kg), ISO induced significant mortality of C57BL/6J mice, and in the mice that survived until day-14 post-injury, only induced a modest increase in interstitial LV fibrosis. Interestingly though, this modest increase in interstitial LV fibrosis led to mice receiving 50 or 100 mg/kg ISO to undergo some systolic dysfunction (reduced ejection fraction in conjunction with increased end-systolic volume) and borderline LV stiffness and diastolic dysfunction, in the absence of any noticeable changes to LV mass. This suggested that to even induce some level of LV dysfunction in more cardiac fibrosis-resistant mouse strains, these animals had to be stimulated to undergo higher levels of oxidative stress and necrosis-induced LV damage that ultimately led to a detectable level of systolic dysfunction, but at the expense of a higher mortality rate. Although other features of DCM were not investigated in C57BL/6J mice in this study, it is questionable whether it is worth pursuing studies in these cardiac fibrosis-resistant mouse strains to evaluate the pathological features of DCM and to test the efficacy of novel therapeutics or therapeutic strategies that can treat the disease (given the limited pathology that can be detected in fibrosis-resistant mouse strains). Knowing the specific mouse strain employed when doing such experiments is important, as many experiments are performed on mixed background mice, which could be associated with potential complications in data outputs.
It should be taken account that there were a few limitations to this study that need to be addressed in the future: (i) only 8–12 week-old adult male mice were used, so the impact of repeated ISO administration on the fibrosis that develops in age-matched female mice and older (12–24 month old) male versus female mice requires investigation (as ageing is a major risk factor for CVDs). (ii) The study focused on the myocardial fibrosis that developed in this model after a 14-day period, hence, other features of cardiomyopathy including LV inflammation, oxidative stress, hypertrophy and remodelling over varying time-points post-ISO injury could provide further insights into strain and sex-dependent outcomes in this model. (iii) The molecular mechanisms that underpin the findings acquired were not determined, but should be investigated to identify the main contributors to these strain-dependent differences.
5. Conclusions
This study identified that the severity of ISO-induced myocardial fibrosis and related dysfunction in age-matched adult mice is strain-dependent. It also determined that the consecutive administration of higher dosing (50 or 100 mg/kg) of ISO to a more cardiac fibrosis-resistant mouse strain (C57BL/6J) induced a moderately elevated level of LV fibrosis and related systolic dysfunction, that was not detectable in mice repeatedly given a lower dose (25 mg/kg). However, this higher dosing of ISO to C57BL/6J mice led to a high incidence of animal mortality, whilst the aberrant structural and functional consequences measured were still not as severe as that measured in a cardiac fibrosis-sensitive mouse strain (129sv) given repeated lower dosing of ISO (25 mg/kg). These findings point to ensuring that the correct mouse strain is utilized for studies evaluating the pathological consequences of ISO-induced DCM, and particularly for testing novel treatment options for the fibrosis and related dysfunction that develops in this model.
Acknowledgments
We are grateful to the Monash Histology Platform for the assistance provided on tissue processing, staining and scanning.
Author Contributions
Conceptualization, C.S.S.; Methodology, C.W., A.C., D.V.N.S., M.N., C.W., C.S.S.; Formal Analysis, C.W., A.C., C.S.S.; Investigation, C.W., A.C., D.V.N.S., M.N., C.W., C.S.S.; Resources, R.E.W.; Data Curation, C.W., A.C., D.V.N.S., M.N., C.W., C.S.S.; Writing – Original Draft Preparation, C.S.S.; Writing – Editing: C.W., A.C., D.V.N.S., M.N., C.W., R.E.W.; Supervision, C.S.S., R.E.W., C.W., A.C.; Project Administration, C.S.S.; Funding Acquisition, C.S.S.
Ethics Statement
The study was conducted according to the guidelines of the Australian Code of Practice for the Care and Use of Laboratory Animals for Scientific Purposes, and approved by the Animal Ethics Committee of Monash University. Two protocol codes apply to this research: MARP/2012/049 (date of approval: 24 April 2012) for experiments investigating the impact of mouse strain on isoproterenol (ISO)-induced myocardial fibrosis (data presented in Figure 1), and MARP/2023/37326 (date of approval: 20 March 2023) for experiments examining the dose-dependent effects of ISO in C57BL/6 mice (data presented in Figure 2).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Funding
This work was supported by Monash Graduate Scholarships to D.V.N.S.; and a Monash Biomedicine Discovery Fellowship to C.S.S.
Declaration of Competing Interest
All authors have nothing to disclose.
References
-
1.
Frangogiannis NG. Cardiac fibrosis: Cell biological mechanisms, molecular pathways and therapeutic opportunities.
Mol. Aspects Med. 2019,
65, 70–99.
[Google Scholar]
-
2.
Frangogiannis NG. Cardiac fibrosis.
Cardiovasc. Res. 2021,
117, 1450–1488.
[Google Scholar]
-
3.
Henderson NC, Rieder F, Wynn TA. Fibrosis: from mechanisms to medicines.
Nature 2020,
587, 555–566.
[Google Scholar]
-
4.
Mehdipour M, Park S, Huang GN. Unlocking cardiomyocyte renewal potential for myocardial regeneration therapy.
J. Mol. Cell Cardiol. 2023,
177, 9–20.
[Google Scholar]
-
5.
Weintraub RG, Semsarian C, Macdonald P. Dilated cardiomyopathy.
Lancet 2017,
390, 400–414.
[Google Scholar]
-
6.
Hershberger RE, Hedges DJ, Morales A. Dilated cardiomyopathy: the complexity of a diverse genetic architecture.
Nat. Rev. Cardiol. 2013,
10, 531–547.
[Google Scholar]
-
7.
Fairweather D, Beetler DJ, Musigk N, Heidecker B, Lyle MA, Cooper LT, et al. Sex and gender differences in myocarditis and dilated cardiomyopathy: An update.
Front. Cardiovasc. Med. 2023,
10, 1129348.
[Google Scholar]
-
8.
Harding D, Chong MHA, Lahoti N, Bigogno CM, Prema R, Mohiddin SA, et al. Dilated cardiomyopathy and chronic cardiac inflammation: Pathogenesis, diagnosis and therapy.
J. Intern. Med. 2023,
293, 23–47.
[Google Scholar]
-
9.
Bacmeister L, Schwarzl M, Warnke S, Stoffers B, Blankenberg S, Westermann D, et al. Inflammation and fibrosis in murine models of heart failure.
Basic Res. Cardiol. 2019,
114, 19.
[Google Scholar]
-
10.
Wang Y, Wang M, Samuel CS, Widdop RE. Preclinical rodent models of cardiac fibrosis.
Br. J. Pharmacol. 2022,
179, 882–899.
[Google Scholar]
-
11.
Bhindi R, Witting PK, McMahon AC, Khachigian LM, Lowe HC. Rat models of myocardial infarction. Pathogenetic insights and clinical relevance.
Thromb. Haemost. 2006,
96, 602–610.
[Google Scholar]
-
12.
Lindsey ML, Brunt KR, Kirk JA, Kleinbongard P, Calvert JW, de Castro Bras LE, et al. Guidelines for in vivo mouse models of myocardial infarction. Am. J. Physiol. Heart Circ. Physiol. 2021, 321, H1056–H1073.
-
13.
Frank A, Bonney M, Bonney S, Weitzel L, Koeppen M, Eckle T. Myocardial ischemia reperfusion injury: from basic science to clinical bedside.
Semin. Cardiothorac. Vasc. Anesth. 2012,
16, 123–132.
[Google Scholar]
-
14.
Munz MR, Faria MA, Monteiro JR, Aguas AP, Amorim MJ. Surgical porcine myocardial infarction model through permanent coronary occlusion.
Comp. Med. 2011,
61, 445–452.
[Google Scholar]
-
15.
Tang YP, Liu Y, Fan YJ, Zhao YY, Feng JQ, Liu Y. To develop a novel animal model of myocardial infarction: A research imperative.
Animal Model Exp. Med. 2018,
1, 36–39.
[Google Scholar]
-
16.
Rona G, Chappel CI, Balazs T, Gaudry R. An infarct-like myocardial lesion and other toxic manifestations produced by isoproterenol in the rat.
AMA Arch. Pathol. 1959,
67, 443–455.
[Google Scholar]
-
17.
Handforth CP. Isoproterenol-induced myocardial infarction in animals.
Arch. Pathol. 1962,
73, 161–165.
[Google Scholar]
-
18.
Murugesan M, Revathi R, Manju V. Cardioprotective effect of fenugreek on isoproterenol-induced myocardial infarction in rats.
Indian J. Pharmacol. 2011,
43, 516–519.
[Google Scholar]
-
19.
Gazenfeld E, Rosenmann E, Davies AM, Laufer A. Isoproterenol induced myocardial lesions in the immunized and non-immunized rat. II. Histopathological lesions after specific immunization.
Immunology 1966,
10, 193–198.
[Google Scholar]
-
20.
Benjamin IJ, Jalil JE, Tan LB, Cho K, Weber KT, Clark WA. Isoproterenol-induced myocardial fibrosis in relation to myocyte necrosis.
Circ. Res. 1989,
65, 657–670.
[Google Scholar]
-
21.
Dudnakova TV, Lakomkin VL, Tsyplenkova VG, Shekhonin BV, Shirinsky VP, Kapelko VI. Alterations in myocardial ultrastructure and protein expression after a single injection of isoproterenol.
Mol. Cell Biochem. 2003,
252, 173–181.
[Google Scholar]
-
22.
Brooks WW, Conrad CH. Isoproterenol-induced myocardial injury and diastolic dysfunction in mice: structural and functional correlates.
Comp. Med. 2009,
59, 339–343.
[Google Scholar]
-
23.
Samuel CS, Bodaragama H, Chew JY, Widdop RE, Royce SG, Hewitson TD. Serelaxin is a more efficacious antifibrotic than enalapril in an experimental model of heart disease.
Hypertension 2014,
64, 315–222.
[Google Scholar]
-
24.
Grant MKO, Abdelgawad IY, Lewis CA, Seelig D, Zordoky BN. Lack of sexual dimorphism in a mouse model of isoproterenol-induced cardiac dysfunction.
PLoS ONE 2020,
15, e0232507.
[Google Scholar]
-
25.
Wang C, Gaspari TA, Ferens D, Spizzo I, Kemp-Harper BK, Samuel CS. Simultaneous targeting of oxidative stress and fibrosis reverses cardiomyopathy-induced ventricular remodelling and dysfunction.
Br. J. Pharmacol. 2021,
178, 2424–2442.
[Google Scholar]
-
26.
Fang L, Gao XM, Samuel CS, Su Y, Lim YL, Dart AM, et al. Higher levels of collagen and facilitated healing protect against ventricular rupture following myocardial infarction.
Clin. Sci. 2008,
115, 99–106.
[Google Scholar]
-
27.
Salimova E, Nowak KJ, Estrada AC, Furtado MB, McNamara E, Nguyen Q, et al. Variable outcomes of human heart attack recapitulated in genetically diverse mice.
NPJ Regen. Med. 2019,
4, 5.
[Google Scholar]
-
28.
Barrick CJ, Rojas M, Schoonhoven R, Smyth SS, Threadgill DW. Cardiac response to pressure overload in 129S1/SvImJ and C57BL/6J mice: temporal- and background-dependent development of concentric left ventricular hypertrophy. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H2119–H2130.
-
29.
Walkin L, Herrick SE, Summers A, Brenchley PE, Hoff CM, Korstanje R, et al. The role of mouse strain differences in the susceptibility to fibrosis: a systematic review.
Fibrogen. Tissue Rep. 2013,
6, 18.
[Google Scholar]
-
30.
Barnabei MS, Palpant NJ, Metzger JM. Influence of genetic background on ex vivo and in vivo cardiac function in several commonly used inbred mouse strains.
Physiol. Genom. 2010,
42, 103–113.
[Google Scholar]
-
31.
van den Borne SW, van de Schans VA, Strzelecka AE, Vervoort-Peters HT, Lijnen PM, Cleutjens JP, et al. Mouse strain determines the outcome of wound healing after myocardial infarction.
Cardiovasc. Res. 2009,
84, 273–282.
[Google Scholar]
-
32.
Mekada K, Yoshiki A. Substrains matter in phenotyping of C57BL/6 mice.
Exp. Anim. 2021,
70, 145–160.
[Google Scholar]
-
33.
Blenck CL, Harvey PA, Reckelhoff JF, Leinwand LA. The importance of biological sex and estrogen in rodent models of cardiovascular health and disease.
Circ. Res. 2016,
118, 1294–1312.
[Google Scholar]
-
34.
Kikuchi K, Poss KD. Cardiac regenerative capacity and mechanisms.
Ann. Rev. Cell Dev. Biol. 2012,
28, 719–741.
[Google Scholar]
-
35.
Samuel CS. Determination of collagen content, concentration, and sub-types in kidney tissue.
Methods Mol. Biol. 2009,
466, 223–235.
[Google Scholar]
-
36.
Lekgabe ED, Kiriazis H, Zhao C, Xu Q, Moore XL, Su Y, et al. Relaxin reverses cardiac and renal fibrosis in spontaneously hypertensive rats.
Hypertension 2005,
46, 412–418.
[Google Scholar]
-
37.
de Jong S, van Veen TA, de Bakker JM, van Rijen HV. Monitoring cardiac fibrosis: a technical challenge.
Netherlands Heart J. 2012,
20, 44–48.
[Google Scholar]
-
38.
Steppan J, Jandu S, Wang H, Kang S, Savage W, Narayanan R, et al. Commonly used mouse strains have distinct vascular properties.
Hypertens. Res. 2020,
43, 1175–1181.
[Google Scholar]
-
39.
Emathinger JM, Nelson JW, Gurley SB. Advances in use of mouse models to study the renin-angiotensin system.
Mol. Cell Endocrinol. 2021,
529, 111255.
[Google Scholar]
-
40.
Soppert J, Frisch J, Wirth J, Hemmers C, Boor P, Kramann R, et al. A systematic review and meta-analysis of murine models of uremic cardiomyopathy.
Kidney Int. 2022,
101, 256–273.
[Google Scholar]