1. Introduction
Kawasaki disease (KD) is an acute, self-limited vasculitis affecting medium to small vessels, predominantly in infants and young children, with an unknown etiology. Although 80% of patients are younger than 5 years of age, KD can also occur during adolescence. The disease primarily affects cardiovascular structures, especially the coronary arteries, often leading to the development of coronary artery aneurysms (CAAs). These aneurysms are commonly observed in affected individuals [
1]. CAAs are defined as focal dilations of coronary segments that are at least 1.5 times the diameter of adjacent normal segments and are rarely observed in 0.3–5% of patients undergoing coronary angiography (CAG) [
2]. In older patients with traditional cardiovascular risk factors, atherosclerosis is considered the main cause of CAAs. However, in children and adolescents, KD is the primary cause of CAA, which can lead to adverse cardiovascular events such as myocardial infarction (MI) [
3]. The 2017 American Heart Association (AHA) scientific statement classifies CAAs into three categories—small, medium and large/giant—based on the diameter and Z-Score [
4]. It is generally accepted that small and medium CAAs in KD tend to regress. In contrast, giant aneurysms (Z-Score ≥ 10 or absolute dimension ≥ 8 mm) typically do not regress and are associated with a poorer prognosis. These giant CAAs are more likely to lead to stenosis, thrombosis or calcification, resulting in myocardial ischemia, infarction and even sudden cardiac death [
5,
6]. Here, we report a typical case of a juvenile with KD and a history of acute myocardial infarction (AMI) caused by multiple giant coronary aneurysms.
2. Case Presentation
A 16-year-old boy with a medical history of KD presented to the cardiology clinic with occasional precordial discomfort for 3 months, following a recent hospital admission for acute inferior myocardial infarction (AIMI) on 15 July 2022.
The patient’s “atypical KD” was first diagnosed in 2012 when he was 6 years old. Initially, the boy presented with persistent fever for more than 2 weeks, accompanied by cervical lymph node swelling and erythema multiforme. Echocardiography showed no obvious coronary ectasia at that time. Therefore, the boy was diagnosed as KD somewhat empirically. However, his parents couldn’t provide enough information about the specific drug regimen then, except for the nonacceptance of standard medication, including intravenous immunoglobulin (IVIG). According to his parents’ description, the boy has not experienced any acute recrudescence or accepted any specific therapy during the past 10 years. Given the low overall recognition of KD, this family ignored a close follow-up, including any cardiac imaging.
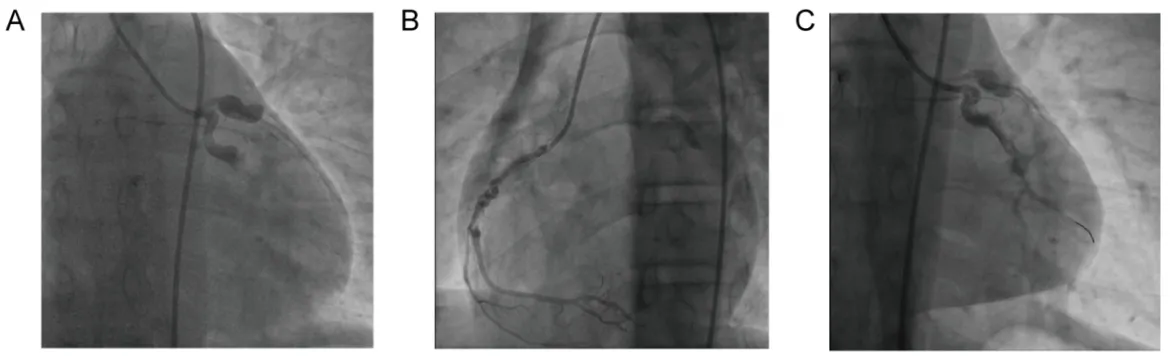
Three months ago, the juvenile presented to the local emergency department at 6:06 a.m., complaining of a 2-h history of aggravating chest pain with sweating, shortness of breath, malaise and even an unconscious apopsychia for 5 min. Vital signs on arrival were unremarkable except for a severe decrease in blood pressure (BP) to 74/41 mmHg. Electrocardiogram (ECG) demonstrated an inferior-wall MI. Emergency CAG revealed a total obstruction in the middle of the left circumflex coronary artery (LCX) and ectasia at the proximal portion with TIMI 0 level. The left anterior descending artery (LAD) was also observed to have proximal ectasia and distal occlusion with TIMI 0 level. Severe tortuosity and ectasia existed in the middle of the right coronary artery (RCA), while maintaining a TIMI III level (
A,B). Thus, the diagnosis of CAAs was confirmed. Given diffuse ectatic changes of all coronaries with no suitable lesion identified for stenting, he was only managed with balloon angioplasty and intracoronary thrombolysis for LCX, the culprit vessel (
C). After the BP stabilized at a normal level, the patient was admitted to the Coronary Care Unit (CCU) for comprehensive medical treatment.Upon admission, laboratory findings revealed several abnormalities: the routine blood test exhibited a white blood cell (WBC) count at 12.2 × 10
9/L (normal range, 4 × 10
9–10 × 10
9/L), a neutrophil count at 8.5 × 10
9/L (normal range, 1.8 × 10
9–6.3 × 10
9/L) and a monocyte count at 1.23 × 10
9/L (normal range, 0.1 × 10
9–0.6 × 10
9/L). Additionally, cardiac biomarkers were also notable, with an elevated serum creatine kinase (CK) level of 2468.00 U/L (nomal range, 0–190 U/L), a creatine kinase isoenzyme level of 164.4 U/L (normal range, 0–24 U/L), a cardiac troponin I (cTnI) level of 1.48 ng/mL (normal range, ≤1.75 ng/mL) and an N-terminal pro-brain natriuretic peptide (NT-proBNP) level of 509.76 pg/mL (normal range, 0–125 pg/mL). Liver function tests indicated elevated serum aspartate aminotransferase (AST) at 288.6 U/L (normal range, 0–38 U/L), alanine aminotransferase (ALT) at 73.2 U/L (normal range, 0–38 U/L) and total bilirubin (TBIL) at 48.2 ummol/L (normal range, 2–20.4 ummol/L). Lipid panel showed a low-density lipoprotein cholesterol of 1.99 mmol/L (normal range, 0–3.36 mmol/L), high-density lipoprotein cholesterol of 1.01 mmol/L (normal range, 1.03–1.55 mmol/L) and that the total cholesterol and triglyceride were both within normal limits. The patient received medical treatment comprising anticoagulation with low-molecular-weight heparin (LMWH), dual antiplatelet therapy (DAPT) with aspirin and clopidogrel, a β-receptor blocker (betaloc), a lipid-lowering drug (atorvastatin), diuretics (furosemide and spironolactone) and a proton pump inhibitor (PPI) (pantoprazole). By the second hospital day, the serum cTnI level had decreased to 0.68 ng/mL. By the third day, the blood routine results had normalized, although mild hepatic insufficiency persisted. An echocardiography performed on July 20th revealed a left ventricular ejection fraction (LVEF) of 54% and segmental dyskinesia in the inferior posterior wall of the left ventricle. After 12 days of medical treatment, the patient’s general condition improved significantly, leading to his discharge from the local hospital.
. Representative emergency CAG images during the AMI in April 2022. (<b>A</b>) Proximal large ectasia, total obstruction of LCX, and proximal large ectasia and distal occlusion of LAD. (<b>B</b>) Severe tortuosity and diffuse ectasia of RCA. (<b>C</b>) Still, nearly 80% remnant stenosis in the middle segment of LCX after balloon angioplasty and intracoronary thrombolysis.
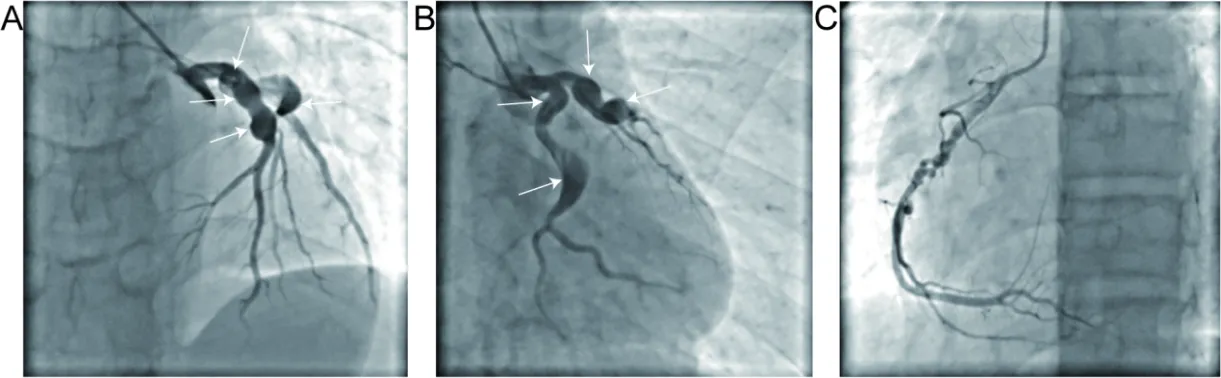
After a period of extramural oral medication, the boy presented to our cardiology department with a 3-month history of chest stuffiness and precordial discomfort, raising concerns about another acute heart attack. A 24-h ECG revealed frequent ventricular premature contractions. Echocardiography indicated left ventricular systolic dysfunction with a LVEF of 0.40 and motion abnormality of the left ventricular inferior wall. CAG detected multiple giant CAAs at the proximal LAD and LCX, with no distal stenosis and TIMI II flow (
A,B). Additionally, a spiral meander was observed in the middle segment of RCA without significant stenosis (
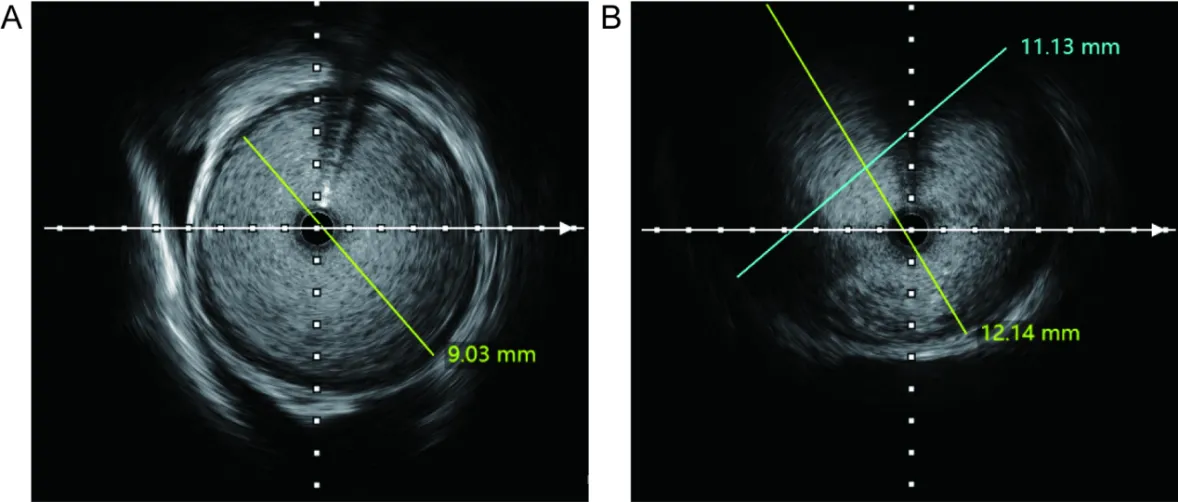
C). Macroscopically, the coronary aneurysmal dilations were notably larger than before. Intravascular ultrasound (IVUS) further assessed the coronary lesions, revealing a maximum diameter of at least 9 mm for the LAD ectasia and an aneurysm exceeding 12 mm in the LCX, with ambiguous boundaries likely due to previous balloon angioplasty (
). Although elective coronary artery bypass grafting (CABG) was recommended, the patient’s family refused the procedure. Serum levels of antinuclear antibody, C-reactive protein, antistreptolysin O, rheumatoid factor and antineutrophil cytoplasmic antibody were inconclusive, ruling out active vasculitis, rheumatic or immunologic diseases. Further review of familial history revealed that no cardiovascular disease (CVD) had been diagnosed for the patient’s parents so far, while his grandfather had ischemic stroke and hypertension. Based on the medical history and characteristic coronary lesions, we speculated that the patient’s large CAAs probably originated from KD. Concurrently, ischemic heart disease (IHD) and microvascular changes in the coronary arteries were believed to be present and worsening. Consequently, we optimized the drug treatment plan. Because of frequent epistaxis, clopidogrel of 75 mg was substituted for aspirin, and warfarin of 3 mg qd was administered with a target international normalized ratio (INR) of 2.0–3.0. Rosuvastatin was used not for intensive lipid-lowering therapy but for its anti-inflammatory and protective effects on vascular endothelial cells. Nicorandil, trimetazidine and ivabradine were added to manage heart rate control and coronary microcirculatory disorder. The patient also received standard quadruple therapy for heart failure (HF), including spironolactone, metoprolol, sacubitril/valsartan and dapagliflozin, which also addressed old myocardial infarction (OMI) and IHD. The dose of β-blockers and angiotensin receptor-neprilysin inhibitors reached 118.75 mg qd and 50 mg bid, respectively, before discharge. Importantly, the patient was told to get regular outpatient reviews to adjust the drug dosage. Echocardiography and ECG were scheduled to be performed at 1, 2, 3, 6, 9, and 12 months during the first year, and every 3 to 6 months thereafter, to monitor changes in CAA size and assess heart function parameters, such as ejection fraction.
. Representative CAG images from Qilu Hospital in July 2022. (<b>A</b>,<b>B</b>) Giant CAAs (white arrows) at the proximal LAD and LCX with no distal stenosis. (<b>C</b>) Spiral meander at the middle segment of RCA with no obvious stenosis.
. Representative IVUS images of the giant aneurysms. (<b>A</b>,<b>B</b>) CAAs with about 9 mm in diameter in LAD and more than 12 mm in LCX with ambiguous boundaries.
3. Discussion
Myocardial infarction due to atherosclerosis is predominantly observed in older patients with classical cardiovascular risk factors. In contrast, the occurrence of MI in younger individuals remains under-researched and presents a distinct risk profile characterized by fewer traditional cardiovascular risk factors compared to the older population. What’s more, as adolescents or young adults are predisposed to developing collateral circulation, their symptoms and signs of myocardial ischemia may be masked and sometimes even ignored. However, the risk of adverse cardiovascular events, such as MI, heart dysfunction and sudden cardiac death, is persistent. In other words, these young individuals require longer and more consistent follow-up than adults throughout their lifetime, which places a greater socioeconomic burden. While plaque rupture continues to be the most common etiology of MI across all age groups, younger individuals exhibit a higher prevalence of rare causes and syndromes [
7]. This case aims to highlight an uncommon etiology of MI in juveniles—coronary artery aneurysms resulting from KD in childhood—thereby drawing attention to the need for further investigation into early-onset cardiac events due to these unique risk factors.
When a patient develops significant coronary artery ectasia or aneurysm formation at a young age and with minimal risk factors for atherosclerotic coronary artery disease (CAD), KD should be speculated as a potential diagnosis [
8]. Kawasaki disease, also known as mucocutaneous lymph node syndrome, has been reported in more than 60 countries and regions worldwide since first reported by doctors in Japan in 1967. This disease is most prevalent in Japan, followed by Korea, and its incidence has been increasing recently in various countries around the world[
9]. Though the etiology and pathogenesis of KD remain unclear, it is generally considered to be a self-limiting disease with acute systemic vasculitis, primarily affecting small and mediun-sized arteries, such as the coronary arteries. KD predominantly, but not exclusively, affects children aged 6 months to 5 years. In developed countries, KD with coronary artery lesions, including coronary artery stenosis, dilation and the formation of CAAs, has now surpassed rheumatic fever as the leading cause of acquired heart disease in children [
10]. It has been reported that the familial history of CVD, including hypertension, dyslipidemia, myocardial infarction, stroke and diabetes, is associated with increased risk of KD for newborns [
11], which seems to be the only risk factor for our patient to suffer from KD.
Coronary artery aneurysm represents the most common and hazardous late complication of KD, typically manifesting several years post-onset. Notably, up to 25% of untreated KD juveniles develop coronary aneurysms. Even with treatment, the incidence of persistent aneurysms remains between 3% and 5% [
12]. The most frequent sites of aneurysm formation, in descending order of prevalence, are the proximal LAD, proximal RCA, left main coronary artery, LCX, and, finally, the distal RCA. [
13]. These young patients with persistent coronary ectasia face a lifelong risk of thrombosis and the development of stenotic lesions during vascular remodeling, which can lead to myocardial ischemia, infarction or even cardiac death. As children with KD-induced CAAs age, the risk of acute ischemic events escalates, particularly in those with large or giant aneurysms [
14], as observed in our patient.
Giant CAAs are relatively rare, with an incidence of only 0.02% in patients with coronary aneurysms [
15]. Notably, cases involving simultaneous multiple giant CAAs in two or more major coronary arteries are exceedingly uncommon. Our patient presents a rare instance of large CAAs, with dimensions of approximately 9 mm in LAD and more than 12 mm in LCX. This case underscores the diagnostic and therapeutic challenges associated with giant CAAs in KD patients. According to Z-score and diameter, the aneurysms are categorised as small (2.5 ≤ Z score < 5), medium (5 ≤ Z score < 10, and absolute dimension <8 mm), and giant (absolute dimension ≥ 8 mm or Z score ≥ 10). Large or giant CAAs do not “resolve”, “regress”, or “remodel”, and while they rarely rupture, they almost always contain thrombi, which can calcify and become occlusive [
4,
16,
17]. Consequently, complications such as stenotic lesions, thrombosis, and major cardiac events, including MI, are more likely to occur in giant CAAs [
18]. A long-term study involving 1215 KD patients found that 64(5%) developed giant CAAs. Subgroup analysis revealed that 3(5%) of these cases showed regression, 30(47%) experienced occlusion or stenosis and 15 (23%) suffered from MI [
19]. Therefore, it is evident that the larger the aneurysm, the poorer the prognosis. This case was a typical example of multiple giant CAAs in more than one major coronary artery and sudden thrombotic occlusion of an aneurysm precipitating MI.
ECG, echocardiography, computed tomographic angiography (CTA), magnetic resonance imaging (MRI) and CAG are the main methods to examine coronary arteries. Among these, CAG is the most invasive imaging examination for KD and is the gold standard for evaluating the severity, prognostic prediction and therapeutic indications of CAAs [
4,
16]. CAG provides detailed image assessment of the coronary artery lumen and characteristic angiographic findings suggestive of KD, such as marked proximal ectasia followed by a sudden transition to an angiographically normal distal segment. Another pathognomonic feature is the presence of calcification along the arterial wall at sites where former aneurysms have been remodeled [
8]. A better estimation of luminal size and arterial wall changes can be achieved through intravascular ultrasound (IVUS), which aids in evaluating the severity of intimal hyperplasia, as well as detecting thrombi, calcification, and luminal narrowing[
20]. In our case, the young boy underwent CAG twice. Initially, an ECG showed acute inferior myocardial infarction and then emergency CAG revealed distinct ectasias in all three coronary arteries. During the second CAG, combined with IVUS, we confirmed the presence of giant CAAs in both the LAD and LCX. Given the typical ECG results, elevated myocardial injury markers, severe hemodynamic disorder, and most importantly, the features of coronary lesions, it was retrospectively further clarified that the definitive diagnosis was MI secondary to giant coronary aneurysms associated with KD. Patients diagnosed with giant CAAs are recommended to undergo long-term follow-up assessments with echocardiography frequently and possibly angiography to monitor for increases in luminal dimensions, thrombotic risk, and signs of ventricular dysfunction, enabling timely intervention [
4]. Unfortunately, this patient could not provide detailed echocardiogram results of the coronary arteries since his last MI.
The standard medical protocol for CAA, particularly giant ones, remains inadequately addressed. Despite the absence of fixed guidelines for managing giant CAAs in acute settings, it is imperative to prevent further dilatation and even rupture, as well as thrombus formation. Several case reports have documented the successful management of patients with super-giant CAAs during the acute phase by stabilizing hemodynamic status and maintaining anticoagulation [
21]. According to the Japanese Circulation Society guideline, patients with KD who develop angina or MI are treated similarly to those with such conditions due to other causes [
16]. For KD patients with large or giant aneurysms (≥8 mm or Z score ≥ 10) and a high risk of coronary artery thrombosis, available therapeutic options include double antiplatelet agents such as aspirin and clopidogrel, as well as anticoagulants like warfarin or LWMH [
20,
22], which also helps prevent severe cardiovascular complications at the early stage. What’s more, the combination of warfarin and aspirin is known to have been associated with high cardiac-event-free survival in patients with giant CAA caused by KD [
23]. However, in our case, frequent massive epistaxis indicated the patient’s intolerance to aspirin. Finally, we chose clopidogrel instead of aspirin, which is also consistent with the current guidelines for antithrombotic medication[
4]. Hemodynamic forces play a crucial role in the further dilation of aneurysms, necessitating strict control of blood pressure and heart rate through β-blockers and other antihypertensive medications. The AHA scientific statement incorporates β-blocking agents into the long-term management algorithm for KD patients with large or giant aneurysms. It was reported that KD is associated with accelerated atherosclerosis and early-onset heart failure [
4,
24]. For the juvenile in our case, there was no history of diabetes or hypertension, he had never smoked, maintained a normal body mass index (BMI) of 22.2, and his lipid panel was within normal limits. A familial history of CVD was considered to be the only risk factor. However, it is still crucial for him to accept the early intervention and aggressive medical management of CAD, even without a typical risk profile. Consequently, empirical treatment with low-dose statins is recommended for these KD patients with past or current aneurysms regardless of age or sex, on account of the pleiotropic effects of statins on inflammation, endothelial function, oxidative stress, platelet aggregation, coagulation, and fibrinolysis. Effective medical treatment of angina pectoris and heart failure is also beneficial for our patients [
4].
For patients with coexisting obstructive lesions and ongoing ischemia, percutaneous and/or surgical coronary revascularization are available options [
20]. However, percutaneous coronary intervention (PCI) and stent placement have limited roles in managing ectatic infarction-related arteries compared to non-ectatic coronary disease [
25]. It is always too difficult to select an appropriate scaffold size to match the aneurysmal coronary lesions. Such patients are also at high risk for stent malapposition, evagination or migration in the future [
26]. Thus, in our case, thrombolytic therapy with urokinase-type plasminogen activator was administered for occlusive coronary artery thrombosis to re-establish blood flow as rapidly as possible. Moreover, the long-term prognosis of CABG in young KD patients with severe coronary lesions remains uncertain [
27]. At present, there is not a standard guidline on the selection of revascularization methods against thrombosis caused by CAA. According to our case, it may be beneficial for such patients to accept early thrombolytic therapy as soon as possible. Fortunately, during the patient’s second CAG in our hospital, no severe stenosis or total occlusion was found in any of the three coronary arteries, and the TIMI blood flow level was adequate. Hence, neither PCI nor CABG is urgently required.
Current guidelines about CAAs associated with KD recommend that it is reasonable to stratify patients according to their risk of myocardial ischemia related to thrombosis and stenosis, which mainly depends on the extent of maximal involvement in coronary arteries, together with the evolution of coronary abnormalities over time [
4]. The risk stratification varies as a result of follow-up changes. Therefore, it is essential to conduct close follow-up with cardiology assessments, including echocardiography, electrocardiography, and CCTA, for the boy in our case to monitor for future major adverse cardiovascular events (MACE) post-discharge.
4. Patient’s Perspective
I never expected that a fever of unknown origin at the age of six could lead to such severe heart issues later in my life. The myocardial infarction I suffered in 2022 continued to be a significant event in my life. Fortunately, due to the prompt intervention and the administration of drug therapy from doctors, I was able to recover. However, my concern for my cardiac health prevented me from fully participating in campus life after discharge. With the support of my parents, I adhered to regular outpatient reviews and adjusted my medication as necessary. Although coronary aneurysms persisted, my cardiac function gradually improved over the past two years, with the ejection fraction rising to over 50%. As a college student now, I am able to lead a nearly normal life and engage in moderate exercise. The guidance and the prescribed medication from my doctors have been crucial in my recovery. I hope that increased attention will be given to young patients like me, who suffer from CAAs related to KD.
5. Conclusions
Thrombosis or rupture of coronary artery aneurysms is a rare cause of AMI in juveniles, typically associated with a history of KD from childhood. Approximately 25% of untreated KD patients develop coronary aneurysms, whereas this incidence decreases to 3–5% with appropriate treatment. Giant coronary aneurysms, defined as those with a diameter of ≥8 mm or a Z score ≥ 10, are particularly uncommon. It is widely recognized that the larger the aneurysm, the poorer the prognosis, especially the giant ones. KD juveniles with large or giant CAAs are recommended to get long-term follow-up with echocardiography and possibly angiography. Optimal medical therapeutic options include dual antiplatelet therapy as well as anticoagulants, with additional cardiovascular medications prescribed based on specific conditions, such as treatment for microvascular lesions, chronic heart failure (HF), and ischemic heart disease (IHD). It remains a challenging problem to deal with super-ectatic infarction-related arteries properly through PCI and stent placement. Therefore, unlike other MI patients, conservative drug treatment plays a more crucial role here. CABG and other various surgical options are reserved for these patients despite undefined long-term prognostic improvement. Thus, the development of a standardized guideline for the management of such patients is urgently needed.
Author Contributions
Conceptualization, C.C., L.Q., W.C. and C.Z.; Investigation, C.C. and C.Z.; Resources, W.C. and C.Z.; Writing–Original Draft Preparation, C.C.; Writing–Review & Editing, C.Z. and L.Q.; Visualization, C.C. and C.Z.; Supervision, L.Q. and W.C.; Project Administration, C.Z.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Qilu Hospital of Shandong University (KYLL-202407-054-1, July 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Funding
This research received no external funding.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
1.
Newburger JW, Takahashi M, Burns JC. Kawasaki Disease.
J. Am. Coll. Cardiol. 2016,
67, 1738–1749.
[Google Scholar]
-
2.
Kawsara A, Núñez Gil IJ, Alqahtani F, Moreland J, Rihal CS, Alkhouli M. Management of Coronary Artery Aneurysms.
JACC Cardiovasc. Interv. 2018,
11, 1211–1223.
[Google Scholar]
-
3.
Alioglu E, Turk UO, Engin C, Tengiz I, Tuzun N, Posacioglu H. Left main coronary artery aneurysm in young patient with acute myocardial infarction.
J. Cardiovasc. Med. 2009,
10, 494–496.
[Google Scholar]
-
4.
McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals from the American Heart Association.
Circulation 2017,
135, e927–e999.
[Google Scholar]
-
5.
Bayers S, Shulman ST, Paller AS. Kawasaki disease: Part II. Complications and treatment.
J. Am. Acad. Dermatol. 2013,
69, 513.e1–513.e8.
[Google Scholar]
-
6.
Yeu BK, Menahem S, Goldstein J. Giant coronary artery aneurysms in Kawasaki disease—The need for coronary artery bypass.
Heart Lung Circ. 2008,
17, 404–406.
[Google Scholar]
-
7.
Gulati R, Behfar A, Narula J, Kanwar A, Lerman A, Cooper L, et al. Acute Myocardial Infarction in Young Individuals.
Mayo Clin. Proc. 2020,
95, 136–156.
[Google Scholar]
-
8.
Bhagwat A, Mukhedkar S, Ekbote S, Gordon JB. Missed Kawasaki disease in childhood presenting as myocardial infarction in adults.
Indian. Heart J. 2015,
67, 385–388.
[Google Scholar]
-
9.
Elakabawi K, Lin J, Jiao F, Guo N, Yuan Z. Kawasaki Disease: Global Burden and Genetic Background.
Cardiol. Res. 2020,
11, 9–14.
[Google Scholar]
-
10.
Soni PR, Noval Rivas M, Arditi M. A Comprehensive Update on Kawasaki Disease Vasculitis and Myocarditis.
Curr. Rheumatol. Rep. 2020,
22, 6.
[Google Scholar]
-
11.
Kwak JH, Ha EK, Kim JH, Cha HR, Lee SW, Han MY. Association of Familial History of Diabetes, Hypertension, Dyslipidemia, Stroke, or Myocardial Infarction with Risk of Kawasaki Disease.
J. Am. Heart Assoc. 2022,
11, e023840.
[Google Scholar]
-
12.
Kuo HC. Preventing coronary artery lesions in Kawasaki disease.
Biomed. J. 2017,
40, 141–146.
[Google Scholar]
-
13.
Brogan PA, Bose A, Burgner D, Shingadia D, Tulloh R, Michie C, et al. Kawasaki disease: An evidence based approach to diagnosis, treatment, and proposals for future research.
Arch. Dis. Child. 2002,
86, 286–290.
[Google Scholar]
-
14.
Gray H, Cornish J. Kawasaki disease: A need for earlier diagnosis and treatment.
Arch. Dis. Child. 2019,
104, 615–616.
[Google Scholar]
-
15.
Pham V, Hemptinne Q, Grinda JM, Duboc D, Varenne O, Picard F. Giant coronary aneurysms, from diagnosis to treatment: A literature review.
Arch. Cardiovasc. Dis. 2020,
113, 59–69.
[Google Scholar]
-
16.
Fukazawa R, Kobayashi J, Ayusawa M, Hamada H, Miura M, Mitani Y, et al. JCS/JSCS 2020 Guideline on Diagnosis and Management of Cardiovascular Sequelae in Kawasaki Disease.
Circ. J. 2020,
84, 1348–1407.
[Google Scholar]
-
17.
Takahashi M, Mason W, Lewis AB. Regression of coronary aneurysms in patients with Kawasaki syndrome.
Circulation 1987,
75, 387–394.
[Google Scholar]
-
18.
McCrindle BW, Manlhiot C, Newburger JW, Harahsheh AS, Giglia TM, Dallaire F, et al. Medium-Term Complications Associated with Coronary Artery Aneurysms After Kawasaki Disease: A Study from the International Kawasaki Disease Registry.
J. Am. Heart Assoc. 2020,
9, e016440.
[Google Scholar]
-
19.
Imai Y, Sunagawa K, Ayusawa M, Miyashita M, Abe O, Suzuki JI, et al. A fatal case of ruptured giant coronary artery aneurysm.
Eur. J. Pediatr. 2006,
165, 130–133.
[Google Scholar]
-
20.
Mavrogeni S. Coronary artery ectasia: From diagnosis to treatment.
Hellenic J. Cardiol. 2010,
51, 158–163.
[Google Scholar]
-
21.
Lee J, Kim GB, Kwon BS, Bae EJ, Noh CI. Two cases of super-giant coronary aneurysms after kawasaki disease.
Korean Circ. J. 2014,
44, 54–58.
[Google Scholar]
-
22.
Ono R, Umehara N. Multiple Giant Coronary Artery Aneurysms in Kawasaki Disease.
Mayo Clin. Proc. 2021,
96, 1888–1889.
[Google Scholar]
-
23.
Suda K, Kudo Y, Higaki T, Nomura Y, Miura M, Matsumura M, et al. Multicenter and retrospective case study of warfarin and aspirin combination therapy in patients with giant coronary aneurysms caused by Kawasaki disease.
Circ. J. 2009,
73, 1319–1323.
[Google Scholar]
-
24.
Marek-Iannucci S, Junarta J, Vishnevsky A, Rajapreyar IN, Fradin JJ, Arditi M, et al. Severe late cardiovascular sequelae of Kawasaki disease in a young adult.
J. Paediatr. Child. Health. 2024,
60, 147–150.
[Google Scholar]
-
25.
Abugroun A, Vilchez D, Hallak O, Shahrrava A. A History of Kawasaki Disease from Childhood and Coronary Artery Ectasia with Recurrent ST Elevation Myocardial Infarction: A Therapeutic Challenge.
Cardiol. Res. 2017,
8, 344–348.
[Google Scholar]
-
26.
Kaneko U, Kashima Y, Hashimoto M, Fujita T. Very Late Stent Migration within a Giant Coronary Aneurysm in a Patient with Kawasaki Disease: Assessment with Multidetector Computed Tomography.
JACC Cardiovasc. Interv. 2017,
10, 1799–1800.
[Google Scholar]
-
27.
Tsuda E. Coronary artery bypass grafting for coronary artery stenosis caused by Kawasaki disease.
Expert. Rev. Cardiovasc. Ther. 2009,
7, 533–539.
[Google Scholar]