1. Introduction
After acute myocardial infarction (MI) mediated by atherosclerotic coronary disease, the risk of future cardiovascular events can be minimized by utilization of high intensity statin (HIS) therapy [
1,
2,
3]. This class of medication constitutes an essential aspect of treatment in the secondary prevention of atherosclerotic cardiovascular disease (ASCVD) [
4]. Recognizing the cardio-protective significance of HIS, since 2013, the American College of Cardiology and American Heart Association guidelines for lowering of blood cholesterol [
5] recommend HIS for all patients after MI. Health care providers were thus encouraged to forego the prior Adult Treatment Panel report (ATP) III recommendations to treat to a specific LDL-C goal and instead, without regard to initial LDL-C, place any patient with history of MI on HIS, with the goal of decreasing LDL-C by >50% [
6]. During the ATP III report era, only 21% of patients were discharged from the hospital with HIS following MI [
6,
7]. Prior to 2013, only 14% of patients discharged on HIS remained adherent at 1-year follow-up. Of those who were not discharged on HIS, only 4% were up titrated to HIS [
7]. After the guidelines changed, the rate of provider prescription of HIS during or following hospitalization for MI has improved yet remains suboptimal [
7,
8,
9].
One measure of patient adherence to statin therapy is reflected in the percentage of patients eventually filling a statin prescription after hospital discharge. In a recent study, the percentage of patients who filled a statin prescription following discharge was 27% [
8]. Those who were not discharged on HIS continued to have a low likelihood (11.5%) of appropriately being transitioned to HIS therapy within that year [
8]. Studying the trend of statin utilization and adherence provides value in identifying measures that increase the likelihood that patients will be discharged on the appropriate statin therapy and will demonstrate statin treatment persistence,
i.e., long-term adherence to statin therapy, which is essential in maximizing the secondary preventive benefits.
While there are studies documenting the under-utilization and overall adherence of HIS for the general population [
8], few studies analyze the variation of utilization and adherence within racial subgroups. Studies examining statin adherence within the Black population have been equivocal and have illustrated heterogeneity within the subgroup [
4]. There are even fewer studies analyzing the prescription and utilization of HIS on discharge following MI within minority populations, representing a large gap in literature.
Older individuals represent another subgroup that warrants special consideration. The risk of developing ASCVD increases with advancing age. Unfortunately, the utilization of statins in the elderly population is often underrepresented in randomized controlled trials [
10,
11]. Although there are documented benefits of statins in the elderly population, some prescribers hesitate to use them due to the potential for adverse reactions [
10,
11]. Overall, the use of statins in the elderly is estimated to decrease the risk of major cardiovascular events by 19% [
11,
12]. For example, The Heart Protection Study showed that the risk of future cardiovascular events was decreased by 18% in individuals aged 70 to 80 years old treated with simvastatin 40 mg [
11,
13]. Apart from the documented benefits of statins, it is anticipated that the proportion of older patients discharged on HIS is lower due to actual or perceived risk of statin associated myopathy and other adverse effects. It is important to identify trends within various populations regarding statin prescription at discharge, as tools can be created so that the cardio-protective benefits of statins are not dismissed in potentially marginalized populations.
Prior studies have indicated that less than one-third of individuals had a fill history of HIS after having an MI [
8]. It is hypothesized that statin utilization on discharge, following the 2013 guidelines would continue to be low at our institution. Analysis of statin utilization and adherence rates following MI is valuable, as it allows the identification of trends and development of policy and interventions to maximize utilization of this essential secondary prevention therapy among diverse populations.
Purpose/Objectives
Below you will find the primary objectives and secondary objectives of the study.
Primary Objectives
- Determine the proportion of patients with ACS who are discharged on a HIS.
- Evaluate potential sociodemographic and clinic differences among patients who are discharged on a HIS (race, age, sex, initial lipid profile).
Secondary Objectives
- Evaluate extent to which HIS are prescribed status post MI in the Ohio State University Wexner Medical Center (OSUWMC) population at 1 and 5 years.
- Ascertain the adherence of HIS at 1 year and 5 years status post MI in the OSUWMC population.
This study investigates the trends associated with statin utilization and overall statin adherence following discharge from a single academic medical center after hospitalization for MI. Some data suggest that the most important determinant of HIS persistence 1 year after discharge post MI is the statin dose [
8]. Further investigation is warranted to identify the most important determinants in our population of interest. In addition, the investigators aim to compare the potential differences between utilization of HIS based-on race and gender. It is hypothesized that underuse of HIS after MI is multi-factorial. Evaluating these factors can identify sub-populations that have the lowest rate of HIS prescription, on discharge.
2. Methods
2.1. Data Availability
Data cannot be made available upon request, in accordance with OSUWMC policy.
2.2. Study Population and Design
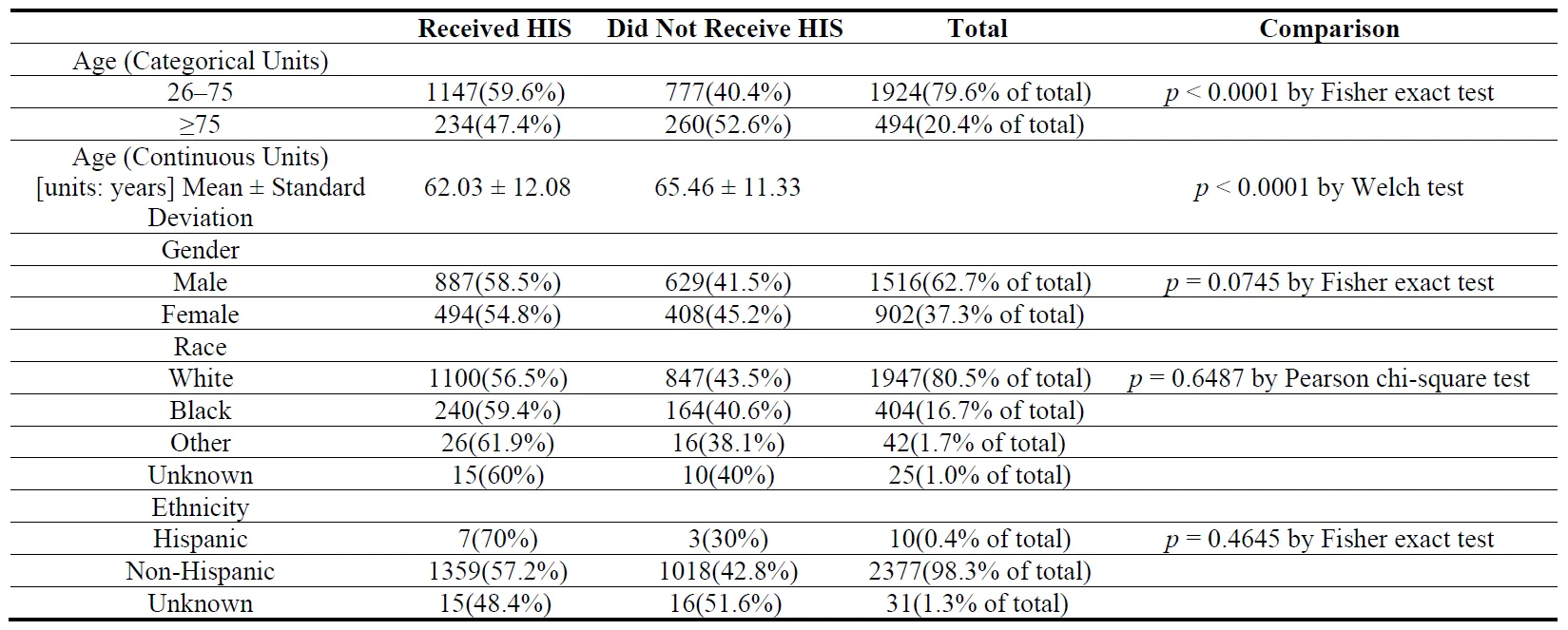
This single-center retrospective observational study was conducted at a major academic medical center. Subject selection included all patients managed at any point of hospitalization for MI from March 2013 through March 2018. This period was selected to identify trends in statin utilization after implementation of 2013 guidelines and to allow for a 1 and 5 year follow up after discharge. There were 2418 subjects (female 37.2%, male 62.8%) evaluated in the study []. This includes patients who had been admitted with ST-elevation myocardial infarction (STEMI) or non-ST-elevation myocardial infarction Type 1 (NSTEMI) at the academic medical center. Patients were considered inactive with the academic medical center if there was no documentation of an office visit within the year following discharge. Those with no recent documentation of statin adherence or who do not continue to follow at the academic medical center are excluded from the denominator for 1-year (Y1) and 5-year (Y5) adherence.
illustrates the baseline characteristics between the groups that received high intensity statins on discharge compared to those that did not.
. Baseline Characteristics.
The clinical data for this project was obtained from the institutional Information Data Warehouse utilizing the Center for Clinical and Translational Science platform of The Ohio State University. We extracted data from medical history documented in the form of ICD-9 and -10 codes, admission keywords, medications, laboratory results during hospitalization, and medication refills. Demographic information, specifically including age, gender, and race were collected from the electronic medical record. HIS classification is recorded as atorvastatin ≥40 mg daily or rosuvastatin ≥20 mg daily. Statin adherence at 1 and 5 years was determined primarily by chart review (assessed for active prescriptions in EMR).
2.4. Statistical Analysis
Pearson chi-square test and Fisher exact test were utilized for comparison of proportions. Baseline proportions were significantly different from Y1 and Y5 proportions compared to Y1 versus Y5 where there is no (significant) difference in the HIS adherence. This was calculated using 3 McNemar tests and Bonferroni correction for 3 comparisons.
3. Results
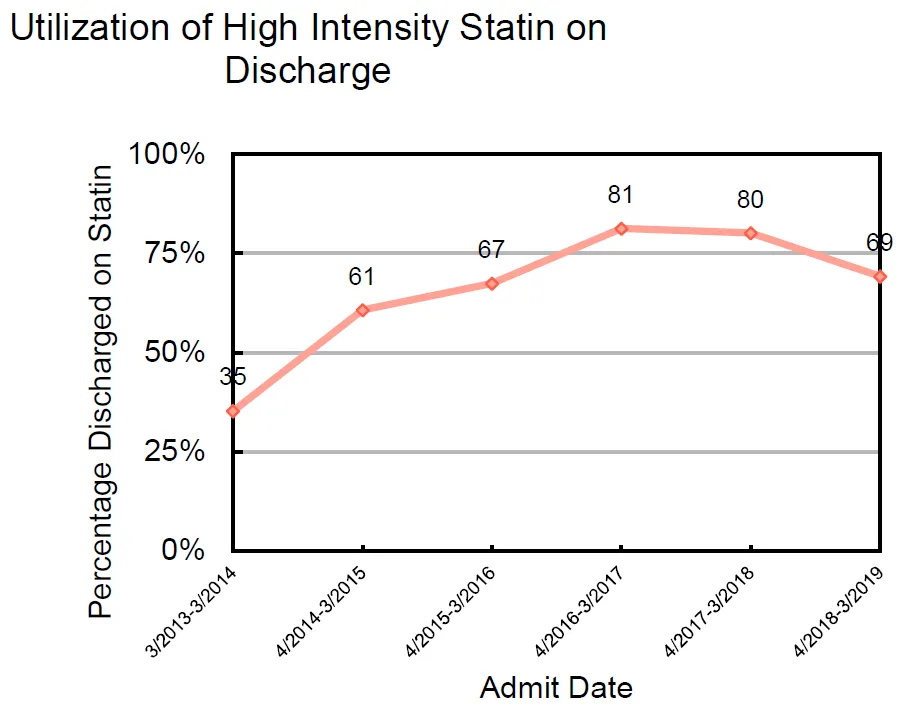
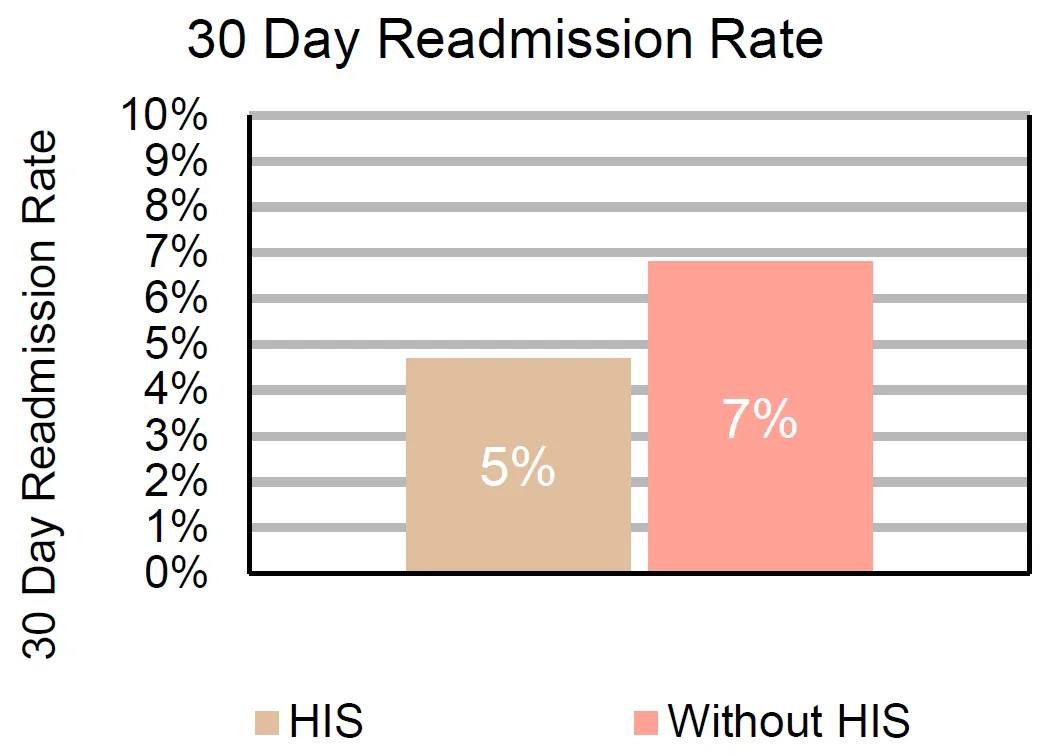
There was a statistically significant increase in the trend of HIS prescriptions on discharge as time progressed following the cholesterol treatment guideline changes in 2013. Within the first year of guideline change (March 2013–2014), only 35.3% of patients with ACS were discharged on a statin. Four years later (March 2018), 80.1% of patients with ACS were discharged on a high intensity statin []. The most common HIS prescribed was Atorvastatin 40 mg (84.7% of HIS), followed by Rosuvastatin 20 mg (9.8% of HIS), Rosuvastatin 40 mg (2.75% of HIS), and Atorvastatin 80 mg (2.75% of HIS) respectively. HIS use was associated with a significant reduction in the 30-day readmission rate (
p = 0.0311) compared to those without HIS utilization on discharge (4.7% or 64/1357 versus 6.8% or 70/1029) [].
. The utilization of high intensity statins on discharge over time.
. The 30-day readmission rates in patients on HIS versus those without. (<i>p</i> = 0.0311).
There was no significant difference in the rate of HIS use on discharge across racial groups (
p value 0.6487) and gender (
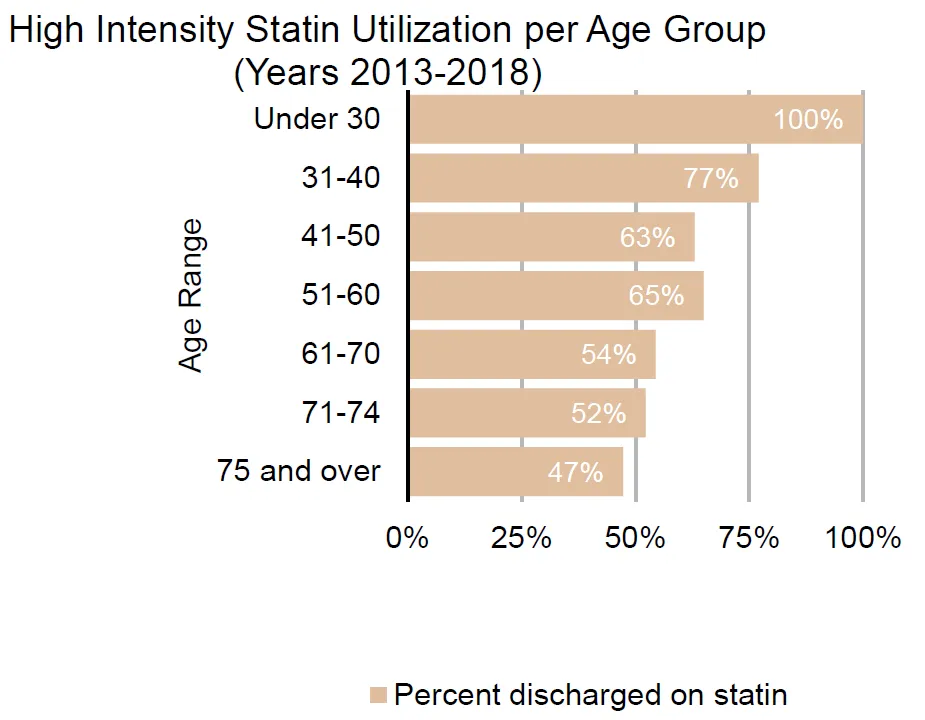
p value 0.0745). Females had a 54.8% HIS prescription rate or utilization on discharge compared to males 58.5%. Subjects who were Black, White, or from other racial groups were found to have 59.4%, 56.5%, and 61.9% HIS utilization at discharge, respectively. Age was found to be a statistically significant variable (
p value < 0.001) associated with HIS utilization. Individuals 75 and older had an expectedly lower rate of HIS utilization on discharge at 47.4% compared to 100% of individuals under 30 years. Overall, it was found that with each 10-year increment in age, the percentage of HIS utilization decreased in a progressive fashion [].
. The percentage of high intensity statin utilization per age group.
The use of statin treatment (including less than high intensity agent/dose combinations) prior to hospitalization resulted in a statistically significant lower percentage of subjects undergoing up-titration to HIS on discharge, compared to those on other lipid lowering therapy therapies. For instance, those who were on a low (LIS) or moderate intensity statin (MIS) on admission had a 15.5% (
p value < 0.0001) or 18.2% (
p value < 0.0001) probability of being discharged on a HIS, respectively. This contrasts to those who were previously treated with a non-statin lipid lowering therapy, who had a 45.9% chance of being discharged on a HIS. There was no statistically significant association between presenting lipid profile (
p value 0.0927) or elevated transaminases (defined as three times the upper limit of normal) and HIS intensity on discharge.
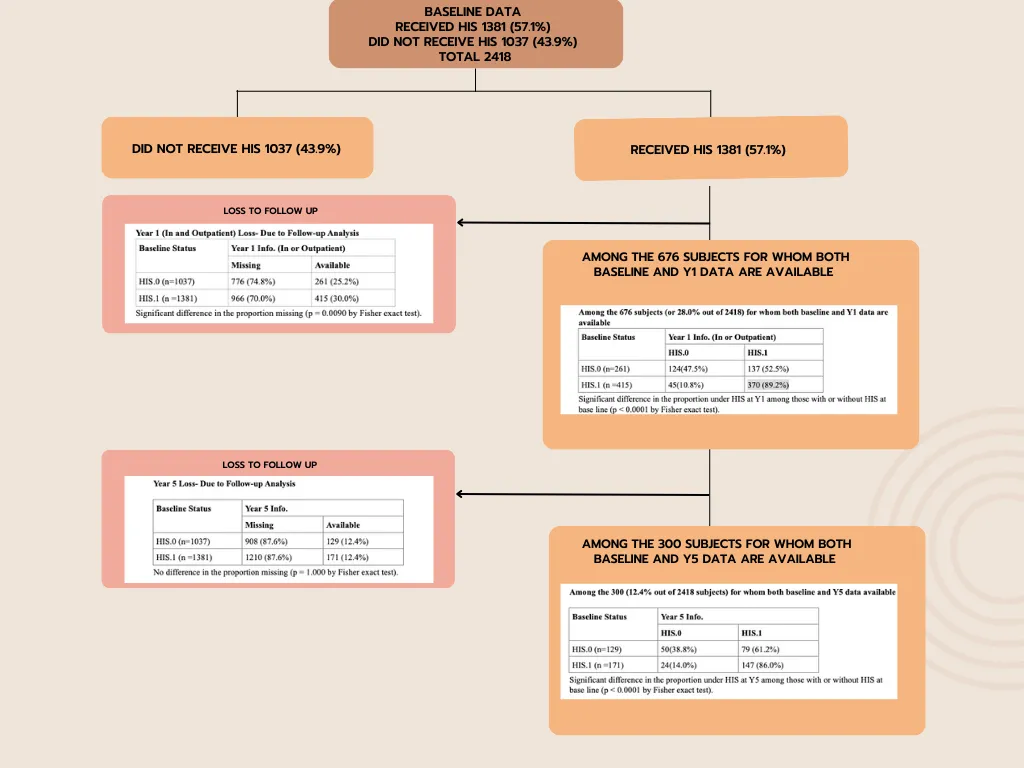
Overall, statin adherence was significantly increased at year 1 (Y1) post-discharge; 75% of the study population was on HIS at Y1 increased from 61.4% on discharge (Y0). Of the patients discharged on a HIS, 89.2% were still on HIS at Y1. All patients no longer on a HIS at Y1 were at least transitioned to either a LIS or MIS. In contrast, only 52% of the patients who were not discharged on a HIS, were up titrated at Y1. When looking at year 5–5.5 (Y5) data, the proportion of HIS adherence at Y5 was 75% compared to 57% at discharge; these proportions were significantly different. For those discharged on HIS, 86% were still on HIS at Y5. Among those who were not discharged on a HIS, 61% were up titrated to a HIS by Y5.
When we compared the proportions of longitudinal changes for subjects from Y0 through Y5, there were only 187 subjects who had data on all 3 time points (Y0, Y1, Y5) []. We analyzed the paired sample of 187 subjects and found that the proportion of HIS at Y0 was 59% (110/187), Y1 was 77.5% (145/187) and Y5 was 77.5% (145/187). Baseline proportions were significantly different from Y1 and Y5 proportions compared to Y1 versus Y5 where there was no significant difference in the HIS adherence. This was calculated using 3 McNemar tests and Bonferroni correction for 3 comparisons. Based on these data, we determined that once on a HIS, individuals have a 90% chance of being on HIS in the future. Mean length to follow up (determined as time to first prescription since discharge) was not found to be a statistically significant factor in appropriate post-discharge adherence to HIS.
4. Discussion
This study demonstrated that after the cholesterol treatment guideline change of 2013, there has been a sequential increase in HIS utilization in non-elderly patients who suffered an MI. Fortunately, underutilization of HIS within the Black population was not observed within our institution, contrary to what has been documented in previous studies. There is a need for further research to identify factors that contribute to this recognized disparity, as the reason for HIS underutilization in this population is not completely understood but could depend on pharmacogenomic factors that differ by race and/or social determinants of health [
14,
15].
Age was the sole demographic factor found to have a significant difference in HIS utilization patterns. This may be attributed to provider perceptions regarding the safety of statin use in the elderly population or higher probability of longitudinal exposure to statins and known statin intolerance leading to downward titration in the intensity of statin agent and/or dose prior to the index admission. The latter explanation can also explain the finding that individuals admitted to the hospital on prior lipid lowering therapy had lower likelihood of being up-titrated to HIS after MI on discharge, at year 1- and 5-years post-index admission. While some may attribute the nonuse of HIS in the elderly population to the ACC/AHA 2013 recommending use of moderate potency in this population, the guidelines do reiterate that there is a dearth of data on subjects within this age range in randomized control trials [
16]. Despite the lack of inclusion of the elderly in RCTs, certain data suggest benefit of HIS despite gender, baseline LDL or age [
17,
18,
19].
Our study demonstrated that individuals discharged on HIS had a high likelihood of HIS treatment persistence in the future and that subjects discharged on HIS had lower readmission rates. While it is well established that statin use is associated with lower mortality and MACE, there is limited evidence in the literature regarding the association between HIS utilization and reduced readmission rates [
17]. Thus, the relationship between HIS use and reduced readmissions rates presented in our study represents a potentially novel finding.
This observation raises the question whether suboptimal therapy is associated with multiple hospitalizations within a year. Post myocardial infarction HIS adherence leads to decreased risk of further adverse cardiac events and (per our study) subsequent admissions, which are key outcomes associated with quality of life and healthcare cost associated with the societal burden of cardiovascular disease.
The finding of HIS associating with reduction in readmission rate inspires the need for further quality improvement initiatives to ensure that inpatients continue to be discharged on HIS and remain adherent on follow up. These initiatives could also have the potential to improve other evidence-based medication regimens for ACS, as patients who are not appropriately discharged on HIS are also less likely to receive aspirin, P2Y12 inhibitors, beta blockers, or other lipid lowering agents [
17].
A recent study by Makmudoa et al. [
20], highlights the importance of an extensive and early lipid lowering strategy in patients with myocardial infarctions. This study demonstrated that when atorvastatin 80 mg was combined with ezetimibe 10 mg on admission, there was a significant improvement in LDL-C goal achievement (<55 mg/dL) in 38% of patients prior to discharge and in 80% after 6 weeks. The study also demonstrated that the addition of bempedoic acid or PSCK9i to a HIS facilitated all patients to reach the LDL-C goal. Such observations show the importance of iteratively studying and adjusting discharge processes to ensure that evidence-based therapies are prescribed during hospitalization for myocardial infarction. Health care providers have a duty to address suboptimal discharge processes, medication reconciliation, and/or patient education upon discharge. Identification of such trends allows for implementation of institutional workflow improvements such as clinical decision support technology that suggests appropriate statin dosage, subsequent laboratory studies and outpatient follow up.
Further research is needed to identify additional determinants of cardiovascular disease progression. In addition to statin adherence post MI, there are lifestyle, medical and psychosocial factors that influence the risk of recurrent MACE in patients [
21]. It has been shown that in addition to statin non-adherence, physical inactivity and higher depression scores were potentially modifiable risk factors associated with MACE [
21,
22]. These factors may play into provider bias on the utility of providing HIS to certain populations
i.e., the elderly [
22]. Other areas for consideration include dedicated analysis of additional clinical and sociodemographic differences among patients who are discharged on HIS, length of follow up post hospitalization for MI, type of practitioner on discharge, and type of insurance.
Limitations
This study had several notable limitations. First, any single-center study may have limited generalizability to other regions and/or health systems. Computer/coder misclassification of statins could have occurred, although the investigators have no reason to suspect a systematic coding problem. The diagnosis of ACS either from a patient’s encounter diagnosis or medical history was assumed to be correct. There is also an opportunity to further stratify ACS into STEMI and NSTEMI Type 1 to see if the type of presenting infarct led to provide misconceptions regarding the indication for HIS. Some potential pitfalls of data acquisition included the possibility that a large population of our subjects had relative contraindications to statins and a high likelihood that certain populations were less likely to follow up as our center. In addition, it was found that the distribution of admissions over time showed substantial reduction in the number of admissions around December 2015. This helps to account for why the number of subjects in each analysis (Y0, Y1, Y5) decreased substantially. In addition, there were multiple medication order (prescription) dates per subject. If there was at least one order for a HIS we classified the subject as having a positive HIS entry. The multiple medication order entries created a barrier in determining type of provider, length to Y1 appointment, and type of statin on discharge, Y1, and Y5. It must also be noted that characteristics of the academic institution may be associated with higher statin use among those with prior barriers with cholesterol lowering therapy given the institutional resource of a dedicated cardiovascular disease prevention and lipid lowering clinic, from which some of the participants may have benefited. The reduced readmission rate may have confounding factors such as potential intrinsically higher risk of readmission in individuals who have baseline contraindications to statins.
5. Conclusions
Increased age was associated with lower rates of HIS, which could have stemmed from prior statin exposure uncovering titrational or complete statin intolerance prior to the index event, a process that would have been much less likely in younger patients who tend to be statin naive. Although HIS have historically been underutilized in Blacks, this was not observed in our center. Further research is needed to define factors that contribute to this known disparity. Individuals discharged on HIS had lower readmission rates; while confounding factors separate from a pure treatment effect of HIS attenuating readmission rate may be represented, this remains a key finding underscoring the benefits of statin therapy in lowering societal burden of cardiovascular disease and associated costs.
Author Contributions
Conceptualization, A.F.A.-B., H.N.N. and M.W.M.; Methodology, A.F.A.-B., H.N.N. and M.W.M.; Software, H.N.N.; Validation, A.F.A.-B., H.N.N. and M.W.M.; Formal Analysis, A.F.A.-B., H.N.N. and M.W.M.; Investigation, A.F.A.-B., H.N.N. and M.W.M.; Resources, A.F.A.-B., H.N.N. and M.W.M.; Data Curation, A.F.A.-B., H.N.N. and M.W.M.; Writing–Original Draft Preparation, A.F.A.-B., H.N.N. and M.W.M.; Writing–Review & Editing, A.F.A.-B., H.N.N. and M.W.M.; Visualization, A.F.A.-B., H.N.N. and M.W.M.; Supervision, M.W.M.; Project Administration, M.W.M; Funding Acquisition, A.F.A.-B. and M.W.M.
Ethics Statement
All procedures were performed in compliance with relevant laws and institutional guidelines and have been approved by the appropriate institutional committees. IRB approval Reference number 00006378 Date 1/2021.
Informed Consent Statement
Patient consent was waived by institutional IRB as the determined risk level was minimal risk to study participants.
Funding
This work was supported by The Ohio State University Center for Clinical and Translational Science (Grant Number RUL1TR02733, 2021).
Declaration of Competing Interest
The senior author (MWM) reports receiving institutional research support from Amgen, Inc., and Novartis Pharmaceuticals.
References
-
1.
Schwartz GG, Olsson AG, Ezekowitz MD, Ganz P, Oliver MF, Waters D, et al.
Effects
of
atorvastatin
on
early
recurrent
ischemic
events
in
acute
coronary
syndromes:
The
MIRACL
study:
A
randomized
controlled
trial.
JAMA 2001,
285, 1711–1718.
[Google Scholar]
-
2.
Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, et al.
Intensive
versus
moderate
lipid
lowering
with
statins
after
acute
coronary
syndromes.
N. Engl. J. Med. 2004,
350, 1495–1504.
[Google Scholar]
-
3.
Pitt B, Loscalzo J, Monyak J, Miller E, Raichlen J. Comparison
of
lipid-modifying
efficacy
of
rosuvastatin
versus
atorvastatin
in
patients
with
acute
coronary
syndrome
(from
the
LUNAR
study).
Am. J. Cardiol. 2012,
109, 1239–1246.
[Google Scholar]
-
4.
Hickson RP, Robinson JG, Annis IE, Killeya-Jones LA, Korhonen MJ, Cole AL, et al.
Changes
in
Statin
Adherence
Following
an
Acute
Myocardial
Infarction
Among
Older
Adults:
Patient
Predictors
and
the
Association
With
Follow-Up
With
Primary
Care
Providers
and/or
Cardiologists.
J. Am. Heart Assoc. 2017,
6, e007106.
[Google Scholar]
-
5.
Stone NJ, Robinson JG, Lichtenstein AH, American College of Cardiology, American Heart Association Task Force on Practice Guidelines. 2013
ACC/AHA
guideline
on
the
treatment
of
blood
cholesterol
to
reduce
atherosclerotic
cardiovascular
risk
in
adults:
A
report
of
the
American
College
of
Cardiology/American
Heart
Association
Task
Force
on
Practice
Guidelines.
J. Am. Coll. Cardiol. 2014,
63 (25 Pt B), 2889–2934.
[Google Scholar]
-
6.
Cleeman JI. Executive
Summary
of
The
Third
Report
of
The
National
Cholesterol
Education
Program
(NCEP)
Expert
Panel
on
Detection,
Evaluation,
And
Treatment
of
High
Blood
Cholesterol
In
Adults
(Adult
Treatment
Panel
III).
JAMA 2001,
285, 2486–2497.
[Google Scholar]
-
7.
Wang WT, Hellkamp A, Doll JA, Thomas L, Navar AM, Fonarow GC, et al.
Lipid
Testing
and
Statin
Dosing
After
Acute
Myocardial
Infarction.
J. Am. Heart Assoc. 2018,
7, e006460.
[Google Scholar]
-
8.
Rosenson RS, Kent ST, Brown TM, Farkouh ME, Levitan EB, Yun H, et al. Underutilization
of
high-intensity
statin
therapy
after
hospitalization
for
coronary
heart
disease.
J. Am. Coll. Cardiol. 2015,
65, 270–277.
[Google Scholar]
-
9.
Wadia SK, Belkin M, Chow KS, Nattiv J, Appis A, Feinstein SB, et al. In-hospital
statin
underutilization
among
high-risk
patients:
Delayed
uptake
of
the
2013
cholesterol
guidelines
in
a
U.S.
cohort.
Hosp. Pract. 2017,
45, 16–20.
[Google Scholar]
-
10.
Leya M, Stone NJ. Statin
Prescribing
in
the
Elderly:
Special
Considerations.
Curr. Atheroscler. Rep. 2017,
19, 47.
[Google Scholar]
-
11.
Horodinschi RN, Stanescu AM, Bratu OG, Pantea Stoian A, Radavoi DG, Diaconu CC.
Treatment
with
Statins
in
Elderly
Patients.
Medicina 2019,
55, 721.
[Google Scholar]
-
12.
Robinson JG, Bakris G, Torner J, Stone NJ, Wallace R. Is
it
time
for
a
cardiovascular
primary
prevention
trial
in
the
elderly?
Stroke 2007,
38, 441–450.
[Google Scholar]
-
13.
Heart Protection Study Collaborative Group. MRC/BHF
Heart
Protection
Study
of
antioxidant
vitamin
supplementation
in
20,536
high-risk
individuals:
A
randomised
placebo-controlled
trial.
Lancet 2002,
360, 23–33.
[Google Scholar]
-
14.
Fatima S, Ferdinand KC, Nissen SE. High-Intensity
Statin
Use
in
African
Americans:
Clinical
Trials,
Observational
Studies,
and
Guidelines.
J. Clin. Hypertens. 2020,
22, 1763–1770. doi:10.1111/jch.14003.
[Google Scholar]
-
15.
Gupta SK, Shay CM, Althouse AD, Magnani JW, Newman AB, Allison M, et al.
Underutilization
of
statins
in
African
American
individuals
with
cardiovascular
disease
risk:
A
systematic
review
and
meta-analysis
. JAMA 2018,
7, e008972. doi:10.1161/JAHA.118.008972.
[Google Scholar]
-
16.
Eisen A, Cannon CP, Braunwald E, Steen DL, Zhou J, Goodrich EL, et al.
Predictors
of
Nonuse
of
a
High-Potency
Statin
After
an
Acute
Coronary
Syndrome:
Insights
From
the
Stabilization
of
Plaques
Using
Darapladib-Thrombolysis
in
Myocardial
Infarction
52
(SOLID-TIMI
52)
Trial.
J. Am. Heart Assoc. 2017,
6, e004332. doi:10.1161/JAHA.116.004332.
[Google Scholar]
-
17.
O’Brien EC, Wu J, Schulte PJ, Christian A, Laskey W, Bhatt DL, et al.
Statin
use,
intensity,
and
3-year
clinical
outcomes
among
older
patients
with
coronary
artery
disease.
Am. Heart J. 2016,
173, 27–34.
[Google Scholar]
-
18.
LaRosa JC, Grundy SM, Waters DD, Shear C, Barter P, Fruchart J-C, et al.
Intensive
Lipid
Lowering
with
Atorvastatin
in
Patients
with
Stable
Coronary
Disease.
N. Engl. J. Med. 2005,
352, 1425–1435. doi:10.1056/NEJMoa050461.
[Google Scholar]
-
19.
deLemos JA, Blazing MA, Wiviott SD, Lewis EF, Fox KAA, White HD, et al. Early
Intensive
vs
a
Delayed
Conservative
Simvastatin
Strategy
in
Patients
With
Acute
Coronary
SyndromesPhase
Z
of
the
A
to
Z
Trial.
JAMA 2004,
292, 1307–1316. doi:10.1001/jama.292.11.1307.
[Google Scholar]
-
20.
Makhmudova U, Samadifar B, Maloku A, Haxhikadrija P, Geiling JA, Römer R, et al. Intensive
lipid-lowering
therapy
for
early
achievement
of
guideline-recommended
LDL-cholesterol
levels
in
patients
with
ST-elevation
myocardial
infarction
(“Jena
auf
Ziel”).
Clin. Res. Cardiol. 2023,
112, 1212–1219. doi:10.1007/s00392-022-02147-3.
[Google Scholar]
-
21.
Sverre E, Peersen K, Weedon-Fekjær H, Perk J, Gjertsen E, Husebye E, et al.
Preventable
clinical
and
psychosocial
factors
predicted
two
out
of
three
recurrent
cardiovascular
events
in
a
coronary
population.
BMC Cardiovasc. Disord. 2020,
20, 61.
[Google Scholar]
-
22.
Zullo AR, Sharmin S, Lee Y, Daiello LA, Shah NR, John Boscardin W, et al. Secondary
Prevention
Medication
Use
After
Myocardial
Infarction
in
U.S.
Nursing
Home
Residents.
J. Am. Geriatr. Soc. 2017,
65, 2397–2404.
[Google Scholar]