Long-Term Impact of Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitors on Major Adverse Cardiovascular Events and All-Cause Mortality: A Systematic Review and Bayesian Meta-Analysis of Randomized Controlled Trials

Long-Term Impact of Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitors on Major Adverse Cardiovascular Events and All-Cause Mortality: A Systematic Review and Bayesian Meta-Analysis of Randomized Controlled Trials
Jahnavi Grover 1,2 Wendy Yao 1 Anjalee Amarasekera 3,4 Alice Leung 1 Ragavi Jeyamohan 1,4 Praba Sekhar 5,6 David Tian 5,7 Timothy Tan 1,2,3,*
Received: 21 March 2026 Revised: 13 April 2026 Accepted: 28 April 2026 Published: 10 June 2026

© 2026 The authors. This is an open access article under the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
1. Introduction
Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of global morbidity and mortality, highlighting the continued need for improved preventive strategies [1]. Specifically, prevention of ASCVD has long emphasised the critical role of reducing both the magnitude and duration of exposure to low-density lipoprotein cholesterol (LDL-C) [2]. Clinical guidelines spanning three decades advocate for aggressive lipid-lowering therapies and lower LDL-C targets, particularly in at-risk populations [3,4]. Statins (HMG-CoA reductase inhibitors) have remained the primary first-line agent of lipid-lowering therapy (LLT), with a 21% proportional reduction in MACE events found in randomised trials for every 1 mmol/L LDL-C reduction [5]. However, limitations of first-line therapies such as statins are evident in clinical practice. A European Union-wide registry revealed that only one-third of patients on statin monotherapy reach their recommended LDL-C target [6], while an Australian study reported that less than 50% of patients met their lipid targets 12 months after hospitalisation with acute coronary syndrome [7]. This discrepancy is even more pronounced among individuals with familial hypercholesterolemia, where less than 3% attain guideline-recommended LDL-C levels, despite their elevated cardiovascular risk [8]. The efficacy of statins is also limited by poor long-term adherence, with 24% non-adherence at 6 months and close to 49% non-adherence at 5 years in an Australian cohort study of national pharmacy data [9].
The landscape of lipid management has changed significantly with the availability of proprotein convertase subtilisin/kexin type 9 (PCSK9) monoclonal antibody therapy, particularly alirocumab and evolocumab. These monoclonal antibodies function by targeting PCSK9, a key regulator of LDL receptor expression [10]. By inhibiting PCSK9, these antibodies disrupt the intracellular degradation and recycling of LDL receptors, a process driven by the formation of complexes between PCSK9 and the LDL receptor [11,12]. This disruption significantly increases the availability of LDL receptors, enhancing the clearance of LDL-C from circulation [13]. These benefits have translated to the clinical setting with trials demonstrating remarkable 50–60% reductions in LDL-C levels with the use of PCSK9 monoclonal antibodies [14]. Further outcomes of trials have also emerged, demonstrating reductions in some major adverse cardiovascular events when PCSK9 monoclonal antibodies are used in conjunction with conventional treatments [15,16]. This systematic review aims to synthesise currently available data and to appraise the effect of PCSK9 inhibitors on MACE outcomes through the robust statistical methods of both Bayesian meta-analysis and Trial Sequential analysis. Bayesian methods provide additional information as posterior probabilities, which represent the likelihood of the treatment effect after incorporating prior knowledge and evidence from current clinical trials.
2. Materials and Methods
2.1. Protocol, Registration, and Ethics
This systematic review was conducted as outlined in the registered protocol (PROSPERO ID# CRD42022355382). It was completed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [17].
2.2. Search Strategy
A systematic search was conducted across the databases PubMed, Ovid Medline, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL, Scopus, and Science Direct for studies published between 2010 and May 2023. Additionally, the reference lists for relevant studies were searched, and grey literature was identified through ProQuest to ensure all relevant studies were included. The search was restricted to English-language articles. The terms used in the search strategy included cardiovascular disease, CVD, ASVCD, hyperlipidemia, hypercholesterolemia, PCSK9 inhibitors, PCSK9 monoclonal antibodies, alirocumab, evolocumab, Repatha, Praluent, and major adverse cardiovascular events. The completed search strategy is provided (Table S1).
2.3. Study Selection and Data Extraction
After duplicate records were removed, the remaining studies were imported into Covidence (Veritas Health Innovation, Melbourne, Australia) and screened by two independent reviewers (J.G. and W.Y.). Conflicts were resolved through discussion or with a third reviewer (A.L.). Inclusion criteria specified studies that were (1) randomised controlled trials; (2) considered adult populations with established cardiovascular risk; (3) compared the effect of a PCSK9 monoclonal antibody to placebo; and (4) reported MACE outcomes with a follow-up of at least 12 months from initiation of treatment. The MACE outcomes included as primary outcomes were myocardial infarction, coronary revascularisation, cardiovascular death, ischemic stroke, and all-cause mortality. Hospitalisation for heart failure and unstable angina were secondary outcomes.
All studies that fulfilled the eligibility criteria underwent data extraction by three independent reviewers (J.G., W.Y., and A.L.) and were compared to ensure concordance. A standardised table was developed on Microsoft Excel for data extraction. Extracted variables included study demographics, patient demographics (age, sex, baseline treatment), endpoints related to MACE outcomes, and follow-up duration. For each study, we extracted the number of events and total participants in each group for the outcomes of interest; data on covariates or multivariable analysis were not collected, as this meta-analysis used unadjusted event data. Where data was incomplete or not reported, analyses were based on available information, and authors were not contacted for additional or missing data, as sufficient data was available to conduct the planned analyses.
2.4. Risk of Bias
Risk of bias was assessed at the study level for the methodological quality of the included studies. Two authors (J.G. and P.S.) separately adjudicated the risk of bias for each study using the Joanna Briggs Institute Tool (JBI) [18]. Disagreements were resolved through discussion. Studies were critically appraised across the following domains for bias related to: selection and allocation, administration of the intervention/exposure, assessment, detection and measurement of the outcome, participant retention, and the validity of their statistical conclusions.
2.5. Statistical Analysis
The primary meta-analysis was performed using the Hartung-Knapp random-effects model (DerSimonian-Laird model), with effect sizes calculated as risk ratio (RR) and 95% confidence intervals (95% CI). Heterogeneity was measured using the I2 statistic, with pre-defined thresholds for low, moderate, and high as 0–39%, 40–70%, and over 70%, respectively. A random-effects model was chosen to account for variation in the true effect sizes across included study populations, follow-up durations, and intervention protocols. Publication bias was assessed using Egger’s test when at least 10 studies were included in the meta-analysis, and visually through inspection of funnel plots.
Bayesian meta-analysis was also conducted to further assess the robustness of the results and to estimate the probability that the treatment effect lies within a particular range, such as risk ratio (RR) < 1. Three different prior distributions were applied, firstly using a ‘non-informative’ prior distribution, with a risk ratio of 1 and a large variance (103) so that the pooled data dominated the posterior distribution, secondly, with a ‘sceptical’ prior distribution, and finally, with an ‘optimistic’ prior distribution. The ‘sceptical’ prior distribution assumes that on average, μ = 0, but there is only a 5% chance that RR will reduce by 30% (σ2 = 0.047). In the ‘optimistic’ prior, it is assumed RR is reduced by 30% (μ = log(0.7)), with the same variance. Between-study variance τ2 was modelled using three different priors to probe the sensitivity of results to different a priori assumptions of between-study heterogeneity. These models include: (i) a uniform prior for τ; (ii) a half-normal with 0.5 scale for τ (iii) a Tibshirani prior as an uninformative prior.
p-values were 2-sided, with p values < 0.05 considered statistically significant. Meta-analysis was performed using R Version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria) with packages meta and bayesmeta.
3. Results
After removing duplicates, the search strategy identified 1776 records. Following title and abstract screening, 41 studies were assessed for full-text eligibility, and nine records were included from the search strategy. One additional record was identified from citation searches, yielding a total of 11 studies eligible for inclusion (Figure 1).
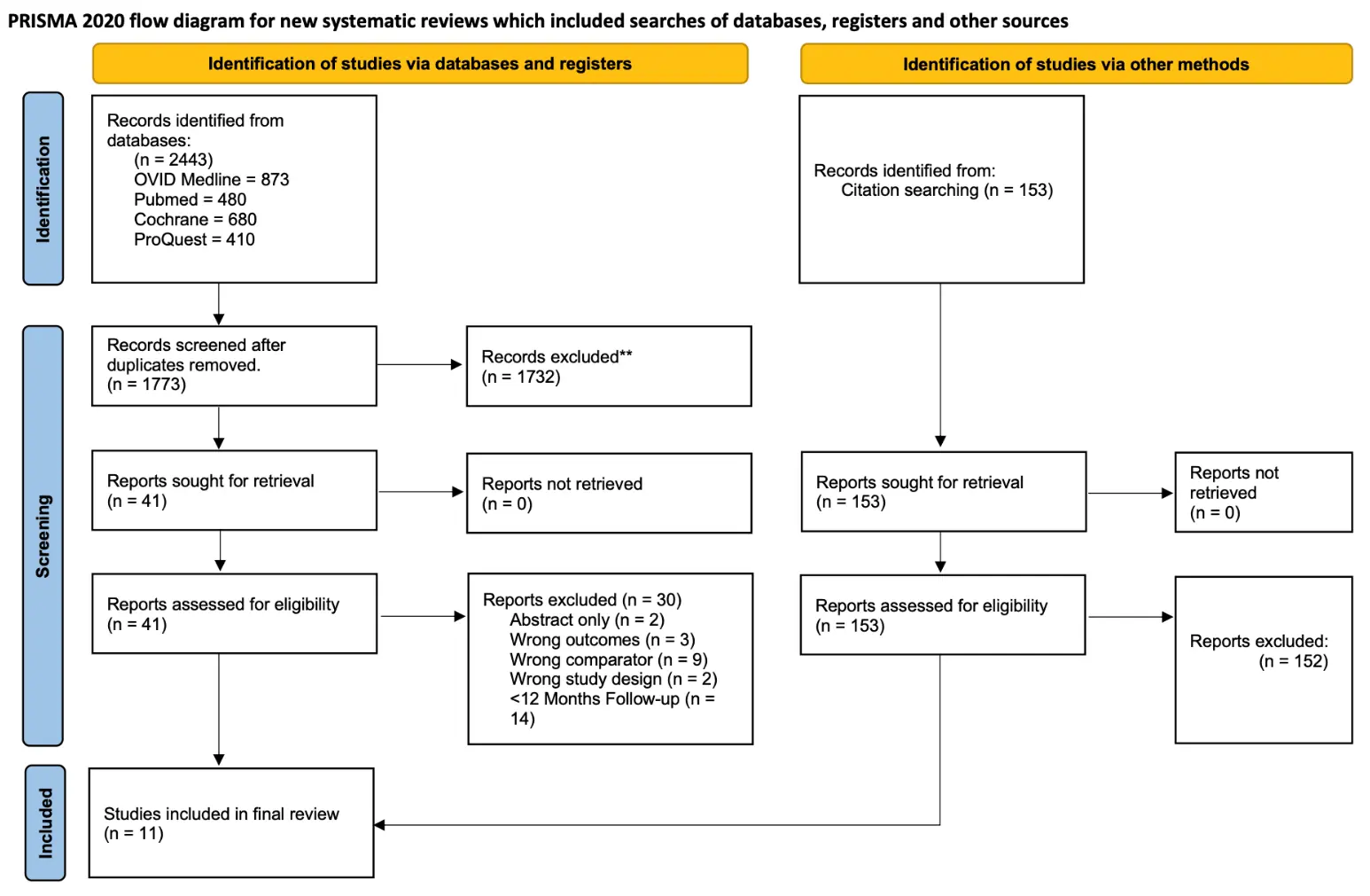
Figure 1. PRISMA flow diagram outlining screening, identification, and inclusion of studies in the meta-analysis. ** if automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools.
3.1. Study Characteristics
In total, 11 double-blinded randomised controlled trials were included in the meta-analysis, encompassing a pooled total of 52,372 patients [15,16,19,20,21,22,23,24,25,26]. Studies ranged from 107 to 27,564 participants, with a median study size of 486 patients, and three studies included over 1000 participants. All patients were enrolled between 2012–2021; one study was conducted in the United States, one in Japan, and the remaining studies were multinational in nature. Follow-up duration ranged from 12 months to 3.4 years, with a median of 78 weeks.
All studies included adult patients with significant cardiovascular disease risk defined as familial hypercholesterolemia, established ASCVD, or significant cardiovascular risk factors. Patients were also on guideline-directed lipid-lowering therapy and did not meet their LDL-C treatment goal with current pharmacological management. There were 2 studies comparing evolocumab (420 mg monthly or 140 mg fortnightly) to placebo and 8 studies comparing alirocumab (75 mg or 150 mg fortnightly) to placebo. The baseline characteristics of the included studies are provided (Table S2). All studies were assessed to have low risk of bias using the JBI tool for randomised controlled trials [18] and were included in statistical analysis (Table S3).
3.2. Primary Outcomes
3.2.1. Myocardial Infarction
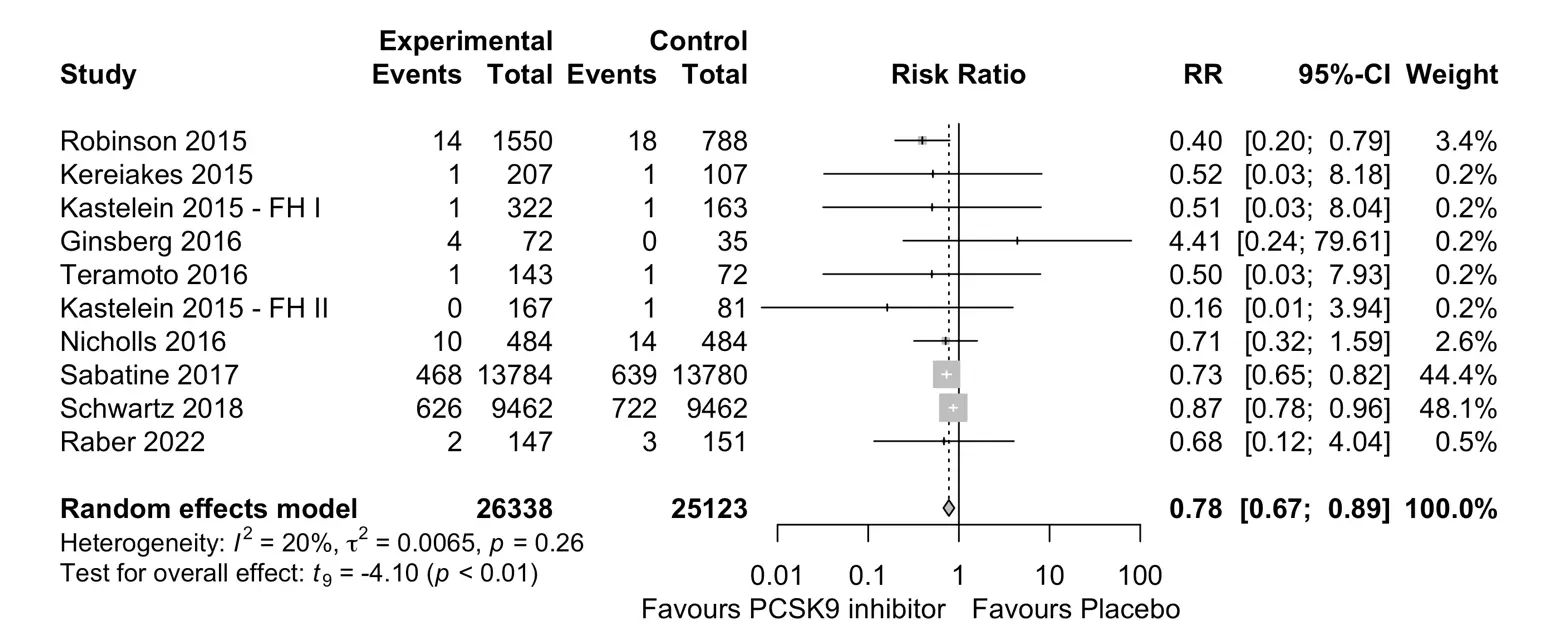
The use of PCSK9 monoclonal antibodies was associated with a significant reduction in the rate of myocardial infarction as compared to placebo (RR 0.78; 95% CI 0.67 to 0.89, p < 0.01). Heterogeneity amongst the ten studies (n = 51,461) was considered low (I2 = 20%) (Figure 2). The posterior probabilities from Bayesian analysis for PCSK9 inhibitors with RR <1, <0.9, and <0.8 were 94.2%, 88.8%, and 71.4%, respectively (Table S4). The TSA results indicated enough events had been accrued in the current trials to support the risk reduction with PCSK9 inhibitors (TSA-adjusted CI 0.74 to 0.86) (Figure S1).
3.2.2. Coronary Revascularisation
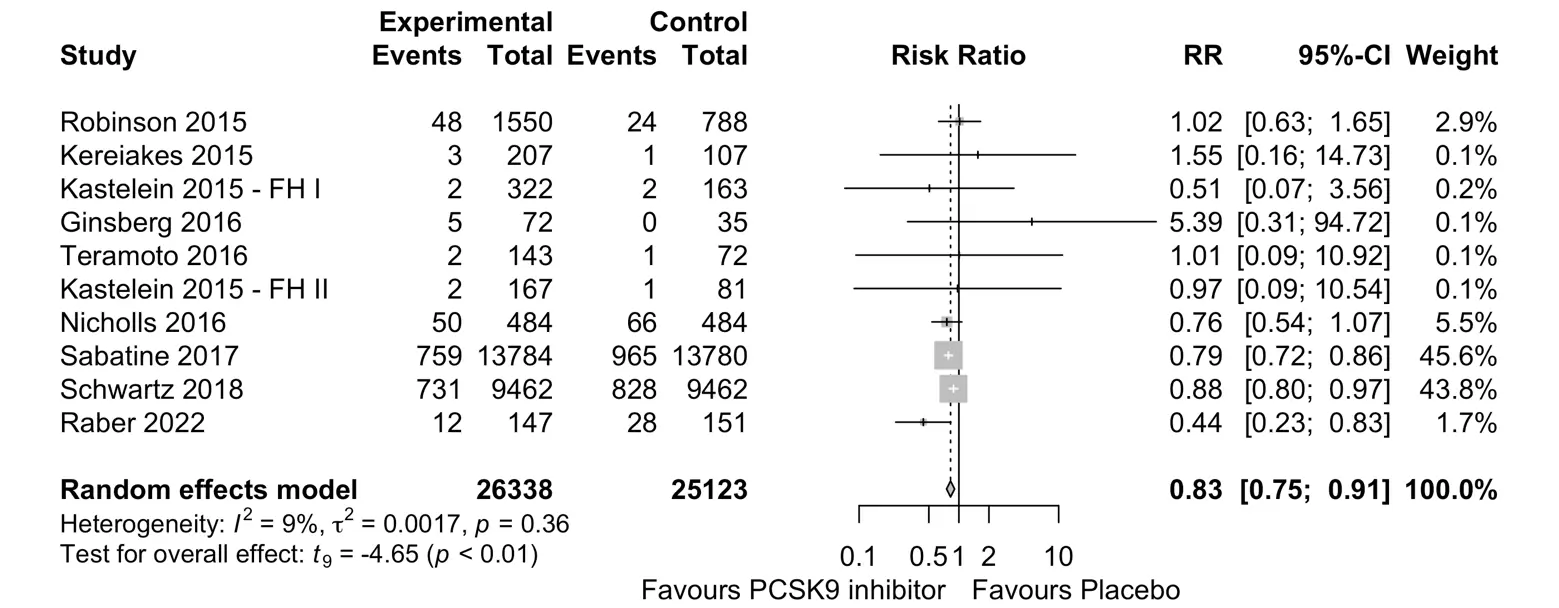
Amongst ten studies randomising a total of 51,461 participants, the use of PCSK9 monoclonal antibodies was associated with a significant reduction in the rate of coronary revascularisation as compared to placebo (RR 0.83; 95% CI 0.75 to 0.91, p < 0.01) (Figure 3). Heterogeneity amongst these studies was considered low (I2 = 9%). With Bayesian meta-analysis, the posterior probabilities resulting in RR <1, <0.9, and <0.8 were 91.4%, 79.4%, and 38.0%, respectively (Table S5). The TSA results indicated enough events had been accrued in the current trials to support the risk reduction with PCSK9 monoclonal antibodies (TSA-adjusted CI 0.78 to 0.88) (Figure S2).
3.2.3. Ischemic Stroke
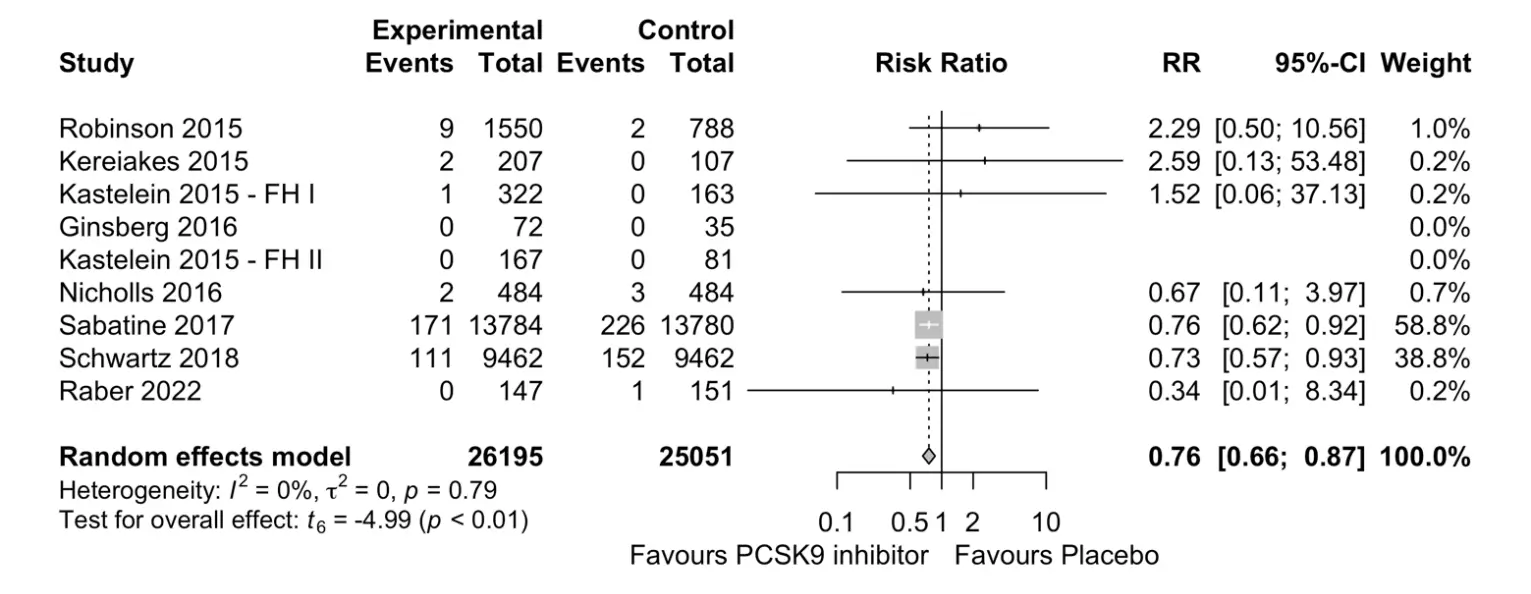
Among seven studies randomising 51,246 participants, the use of PCSK9 monoclonal antibodies was associated with a significant reduction in the risk of ischemic stroke as compared to placebo (RR 0.76; 95% CI 0.66 to 0.87, p < 0.01) (Figure 4). Heterogeneity between these studies was considered very low (I2 = 0%). With Bayesian meta-analysis, the posterior probabilities resulting in RR <1, <0.9, and <0.8 were 83.8%, 75.0%, and 55.0%, respectively (Table S6). The TSA results indicated enough events had been accrued in the current trials to support the risk reduction with PCSK9 monoclonal antibodies (TSA-adjusted CI 0.65 to 0.97) (Figure S3).
3.2.4. All-Cause Mortality
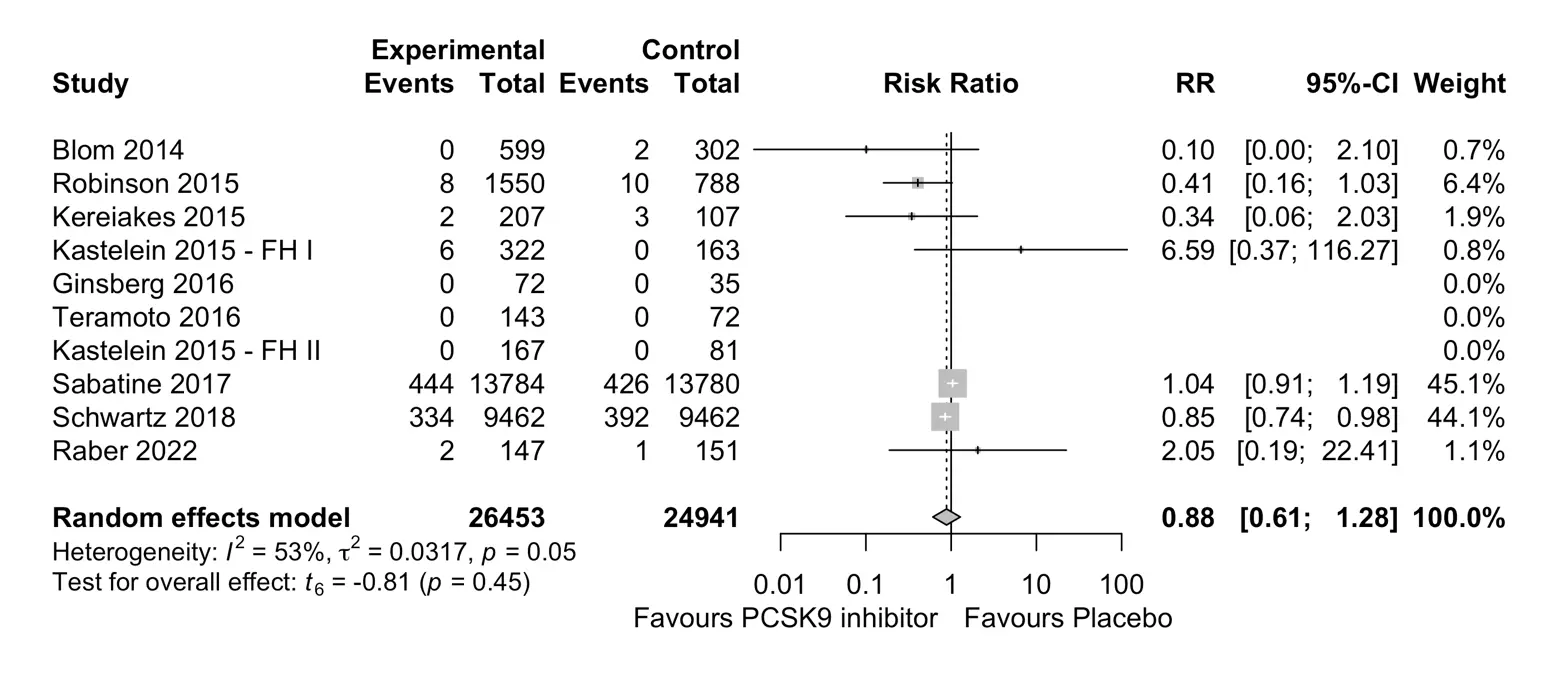
Among seven studies randomising 51,394 participants, no statistically significant effect was observed for the risk of all-cause mortality when comparing PCSK9 monoclonal antibodies and placebo (RR 0.88; 95% CI 0.61 to 1.28, p = 0.45) (Figure 5). Heterogeneity between these studies was considered moderate (I2 = 53%). With Bayesian meta-analysis, the posterior probabilities resulting in RR <1, <0.9, and <0.8 were 82.9%, 63.4%, and 42.4%, respectively (Table S7). The TSA results indicated that there was insufficient information accrued in the current trials to support a risk reduction with PCSK9 monoclonal antibodies for all-cause mortality (TSA-adjusted CI 0.39 to 1.93) (Figure S4).
3.2.5. Cardiovascular Death
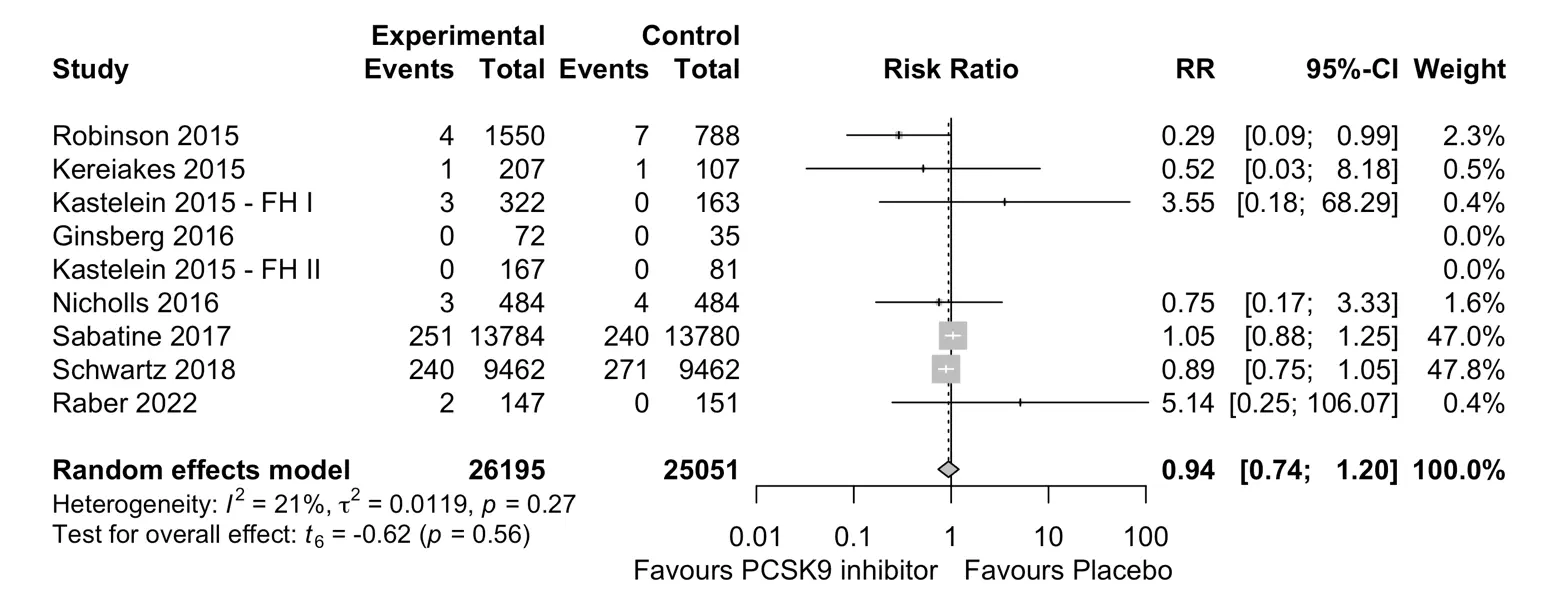
Among seven studies randomising a total of 51,246 participants, no statistically significant difference was observed for the risk of cardiovascular death (RR 0.94, 95% CI 0.74 to 1.20, p = 0.56) when comparing PCSK9 monoclonal antibodies and placebo. Heterogeneity between the studies was considered moderate (I2 = 21%) (Figure 6). With Bayesian meta-analysis, the posterior probabilities resulting in RR <1, <0.9, and <0.8 were 69.4%, 46.5%, and 28.1%, respectively (Table S8). The TSA results indicated that there was insufficient information accrued in the current trials to support a risk reduction in cardiovascular death with PCSK9 monoclonal antibodies (TSA-adjusted CI 0.68 to 1.28) (Figure S5).
3.3. Secondary Outcomes
3.3.1. Hospitalisation for Heart Failure
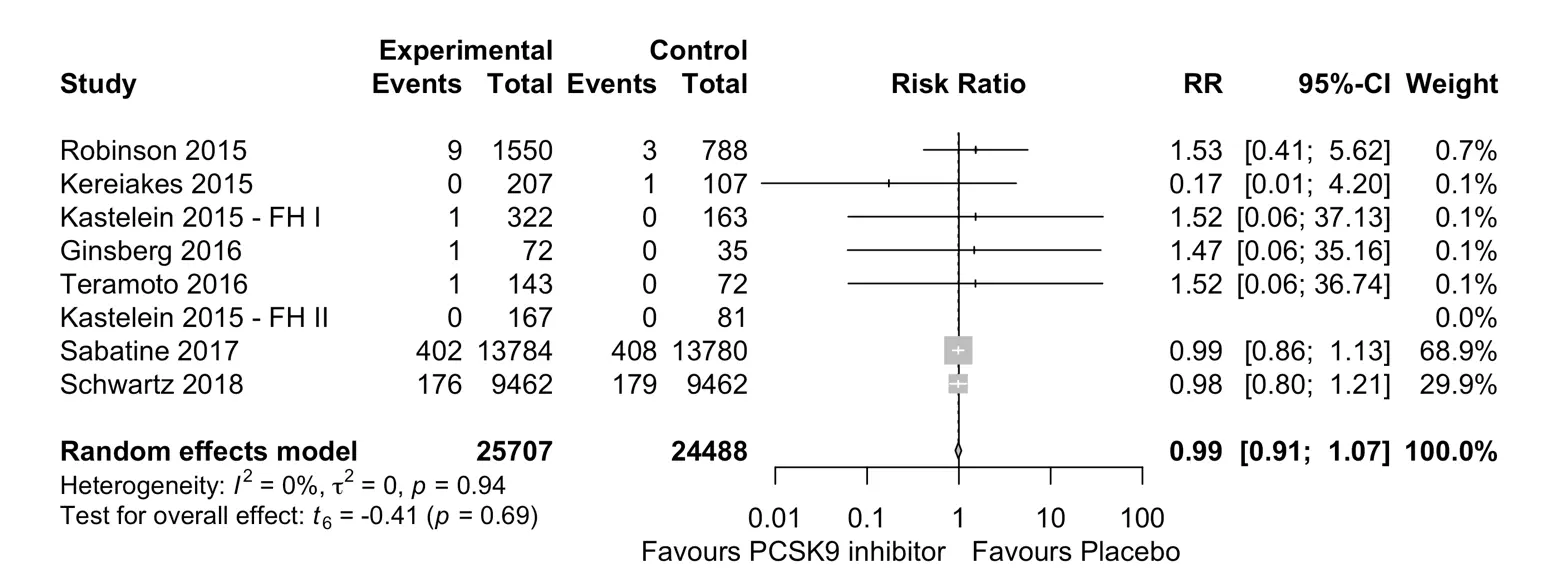
Seven studies randomising 50,195 participants found no statistically significant difference in the risk of hospitalisation for heart failure (RR 0.99, 95% CI 0.91 to 1.07, p = 0.69) when comparing PCSK9 monoclonal antibodies and placebo (Figure 7). Heterogeneity between the studies was considered very low (I2 = 0%).
3.3.2. Hospitalisation for Unstable Angina
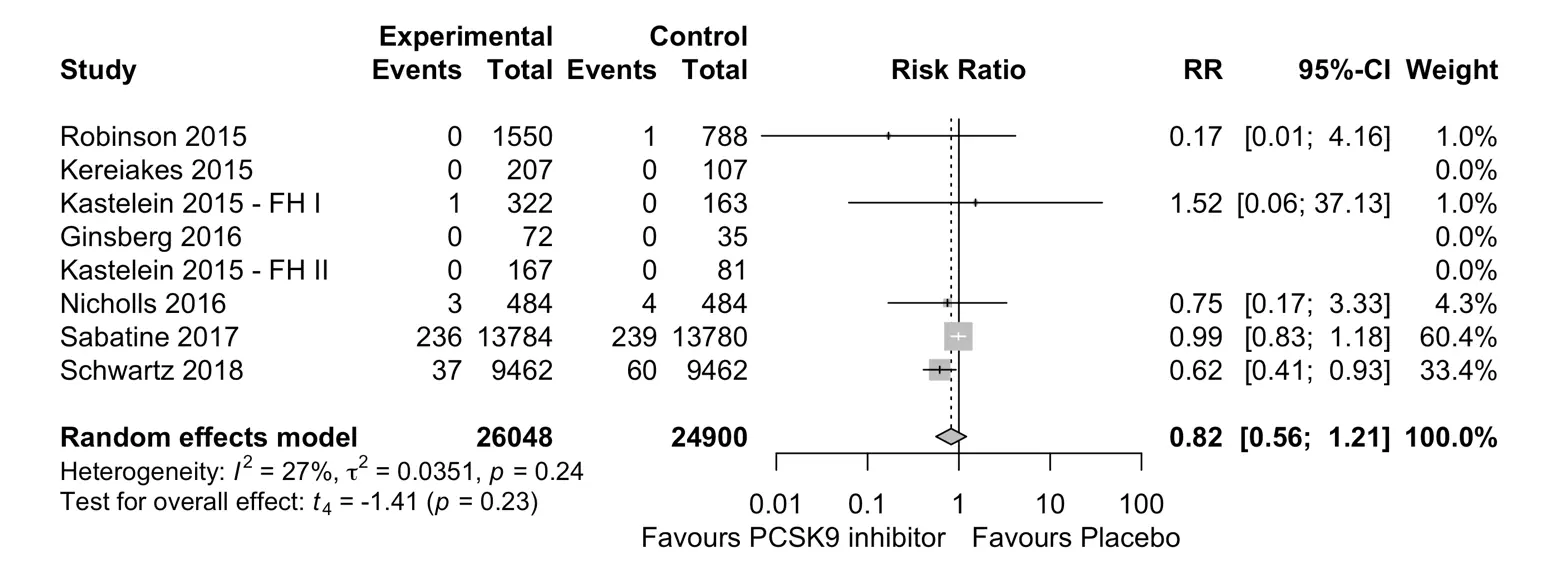
Five studies randomising 50,948 participants found no statistically significant difference in the risk of hospitalisation with unstable angina (RR 0.82, 95% CI 0.56 to 1.21, p = 0.24) when comparing PCSK9 monoclonal antibodies and placebo. Heterogeneity between the studies was considered moderate (I2 = 27%) (Figure 8).
3.4. Publication Bias
Publication bias was not evident through visual inspection of the funnel plots (Figure S6, Figure S7, Figure S8, Figure S9, Figure S10, Figure S11 and Figure S12) or by Egger’s test for any of the included meta-analyses, suggesting low risk of small-study bias over a median follow-up duration of 78 weeks. Leave-one-out analysis showed that the two major outcomes trials (FOURIER and ODYSSEY OUTCOMES) had a strong influence on the overall results but did not alter the overall direction or significance of the results (Figure S13, Figure S14, Figure S15, Figure S16 and Figure S17).
4. Discussion
The results of this meta-analysis demonstrate that, over a median follow-up duration of 78 weeks, the addition of PCSK9 monoclonal antibodies to standard lipid-lowering treatments provides significant benefits in the rates of myocardial infarction, coronary revascularisation, and ischemic stroke compared to placebo. However, no significant benefits were observed for cardiovascular death, all-cause mortality, hospitalisation for heart failure, and unstable angina (Figure 2 and Figure 3). This is consistent with the results of previous meta-analyses [27,28,29,30,31] that have attempted to investigate the efficacy of PCSK9 monoclonal antibodies. This study provides further validation of the reported benefits through rigorous statistical methods. Bayesian analysis allows for probabilities to be determined and improves communication of the effect, whilst Trial Sequential analysis strengthens the validity of the conclusions.
Developments in the understanding of PCSK9 have provided valuable insights on the cardiovascular benefits associated with extremely low levels of LDL-C. Initial studies, notably the Atherosclerosis Risk in Communities (ARIC) study, demonstrated that individuals identified with loss-of-function mutations in PCSK9 had between 21 and 40 per cent reductions in LDL-C levels. Amongst this population, a remarkable 88% reduction in the rate of developing coronary heart disease was identified over a 15-year follow-up period [32]. This effect persisted irrespective of the presence of traditional cardiovascular risk factors amongst the ARIC population. Further research on patients with PCSK9 loss-of-function mutations has reinforced their LDL-C lowering benefits and noted improvements in cardiovascular outcomes associated with the cumulative effect of very low LDL-C levels over time [33,34]. Thus, early studies of PCSK9 provided compelling evidence to support the use of PCSK-based therapies for continued LDL-C lowering.
Subsequent clinical trials of PCSK9 monoclonal antibodies have suggested a profound impact on LDL-C reduction that surpasses the effects of statins or ezetimibe [20,21]. The use of PCSK9 monoclonal antibodies has allowed patients to reach and maintain very low LDL-C levels, which are safe and associated with a significantly lower incidence of MACE [35]. Pre-specified analyses of outcomes from the major PCSK9 inhibitor trials, FOURIER and ODYSSEY, support these findings as strong monotonic relationships between very-low LDL-C levels and decreasing risk of cardiovascular events were observed in these trials [36,37]. Patients who reached very low LDL-C levels (less than 0.5 mmol/L) in these trials had the lowest risk of cardiovascular death, myocardial infarction, stroke, and coronary revascularisation [38]. Analyses of randomised controlled trials further support the safety of achieving very low LDL-C, with no significant increase in adverse events amongst patients who reached very low LDL-C levels on statins, alirocumab, and evolocumab [35,39,40]. The safety and efficacy of very low LDL-C levels are further substantiated by a recent meta-analysis of lipid-lowering trials, which suggested significantly lower levels of MACE amongst patients who achieved very low LDL-C levels (less than 1.0 mmol/L) compared to those with LDL-C levels above 1.0 mmol/L [41]. This underscores the importance of PCSK9 monoclonal antibodies in reshaping the landscape of cardiovascular risk management through the ability to lower LDL-C targets across guidelines.
Comparisons with trials of other LLT shed light on the nuanced dynamics of cholesterol and inflammation in lowering the risk of MACE. In all the included trials, patients were maximised on existing lipid-lowering agents, particularly statins, emphasising their continued importance in the management of ASCVD. While the landmark statin trials demonstrated significant reductions in LDL-C and a correlated 21% relative risk reduction in MACE, their effects in the first 12 months were modest, with only a 9% relative risk reduction in MACE [42]. However, statins have additional benefits beyond their ability to lower lipid levels, such as the anti-inflammatory effects, as supported by lower high-sensitivity C-reactive protein (hsCRP) levels. These have been observed in statin trials and are thought to contribute to the early reduction in mortality. Furthermore, statins also offer added benefits in stabilising atherosclerotic plaque, improving endothelial function, and reducing oxidative stress [43]. These additional pleiotropic effects of statins highlight the value and ongoing importance of statins as first-line lipid-lowering agents [44].
Interestingly, the PCSK9 monoclonal antibodies have also been noted to reduce lipoprotein(a) levels, an independent risk factor of ASCVD and another modulator of inflammation with prothrombotic and pro-atherogenic properties [45]. The role of lipoprotein(a) in promoting ASCVD has been supported by genetic and prospective cohort studies, leading to increasing recognition of lipoprotein(a) as a target in the management of ASCVD [3,46]. Modest reductions in the level of lipoprotein(a) were observed with PCSK9 monoclonal antibodies, and a pre-specified analysis of ODYSSEY OUTCOMES suggested that reductions in lipoprotein(a) after alirocumab treatment were associated with the risk of MACE, particularly MI and cardiovascular death, independent of LDL-C lowering [47]. Moderate benefits in lowering triglycerides, increasing HDL-C concentrations, and plaque stabilisation have also been reported with PCSK9 monoclonal antibodies [48,49]. Thus, as in the case of statin therapy, it is also necessary to consider the additional benefits of mechanisms separate from LDL-C lowering when evaluating and comparing lipid-lowering therapies. While most of the included trials in this study had a 12-month follow-up, greater improvements in MACE may emerge with data on the use of PCSK9 monoclonal antibodies over longer durations.
It is clear that assessing the full extent of benefits from PCSK9 monoclonal antibodies will require data across longer follow-up periods, as both absolute lipid levels and lipid-lowering have a cumulative effect. Further studies with extended follow-up are now open-label extensions that do not directly compare PCSK9 monoclonal antibodies with the current standard of care, although benefits beyond what has been identified in this meta-analysis are expected. The findings from the FOURIER-OLE trial, offering the most extensive long-term data with a median follow-up of 5 years, reinforce the advantages associated with LDL-C lowering in the long term [50]. Significant reductions were observed across cardiovascular death, myocardial infarction, stroke, and hospitalisation for unstable angina for patients who received early initiation of evolocumab compared with delayed treatment initiation [50]. These results suggest that the benefits of PCSK9 monoclonal antibodies encompass mortality outcomes and a broader range of cardiovascular events than those observed in this review. Current research is focused on investigating other methods for targeting PCSK9, with outcome trials underway for inclisiran, a small interfering RNA that inhibits PCSK9 [51]. Additional methods of targeting PCSK9 and therapeutics that specifically target lipoprotein(a) are also in development [52,53].
Despite their clinical efficacy, the uptake of PCSK9i remains constrained by costs, and early cost-effectiveness analyses have raised affordability concerns. These concerns were initially raised because there was insufficient information about their long-term benefits and the practicality of their use in primary prevention populations. Early economic evaluations estimated their incremental cost-effectiveness ratios exceeded commonly accepted thresholds (>$300,000 per QALY) [54,55]. Although subsequent price reductions and emerging long-term outcomes data has improved their economic profile, uncertainties around lifetime adherence and potential adverse effects persist [56]. Their greatest theoretical benefit is in patients with familial hypercholesterolemia, and further comparative studies assessing their relative efficacy in these populations would strengthen the rationale for their targeted use. Consequently, PCKS9i use has been prioritised in secondary prevention and familial hypercholesterolemia patients who fail to achieve lipid targets despite maximal statin and ezetimibe therapy.
Non-adherence significantly constrains the real-world effectiveness of PCSK9 inhibitors, highlighting the gap between efficacy in controlled trials and routine practice. Practical barriers include injectable administration, cost, schedule, and low perceived necessity in asymptomatic patients [57,58]. These contribute to discontinuation and suboptimal dosing, which attenuate sustained LDL-C reduction [58]. Addressing these challenges through targeted adherence strategies is critical to translating trial-based results into population-level outcomes.
Across the included studies, the overall incidence of adverse events was similar between the PCSK9 inhibitor and placebo groups. An exception was seen in the ODYSSEY Japan Trial, where adverse events were reported more frequently (90.9%) in patients receiving alirocumab in comparison to the placebo group (83.3%). The proportion of patients who experienced a serious adverse event in the included studies was comparable between the intervention and placebo groups, except in the ODYSSEY trial, where 7.0% of patients receiving alirocumab had a serious adverse event, compared with 12.5% in the placebo group. Injection-site reactions were consistently more frequent in patients receiving a PCSK9 inhibitor than in those receiving a placebo.
The strengths of this systematic review and meta-analysis emerge from a clear research question, focused on a high-risk population. The meta-analysis evaluated individual outcomes rather than composites to provide clearer comparisons between PCSK9 inhibitors and placebo. The meta-analytical methodology, particularly the use of Bayesian methods, adds robustness to the reported findings. Trial sequential analysis also assessed the risk of random findings and whether an adequate quantity of evidence supported the findings. This paper included high-quality studies, as evaluated by the Joanna Briggs Institute Critical Appraisal tool, and mostly multinational studies, which reduces potential bias and suggests these results can be applied to a wider population. Combining these studies through meta-analytic methods allows for the synthesis of results with a larger population and a greater number of events. Heterogeneity and publication bias were also not significant across the included studies, thereby improving the quality of the results.
There are also several sources of limitations. The included studies had varied trial designs with differences in criteria for patient inclusion and variations in the initial LDL-C levels. These factors may have contributed to population bias, especially in studies focused on populations with genetic predispositions to higher LDL-C who may stand to gain unique benefits from PCSK9 therapy. Whilst most studies had patients who were on baseline statins as tolerated, there was variation in the intensity of statin therapy and the use of other lipid-lowering therapy, which should ideally be optimised prior to use of PCSK9 monoclonal antibodies. The results of this review may also underestimate the effects, given the relatively short follow-up durations in the included studies, whereas previous lipid-lowering trials used five-year follow-up periods. This study could also have been improved with a specific analysis comparing outcomes in different populations, such as patients with familial hypercholesterolemia compared to those with established ASCVD, and further specific papers may allow such a comparison for subgroup analysis. Finally, the results were also largely influenced by study size bias from the two largest trials, FOURIER and ODYSSEY OUTCOMES, which represent over 85% of the total sample size. Hence, the conclusions drawn from this meta-analysis may be heavily influenced by these studies rather than accurately reflect the broader body of evidence, although excluding their results did not change the overall direction or conclusions.
5. Conclusions
In conclusion, the findings of this systematic review and meta-analysis contribute to the evolving landscape of cardiovascular risk management, highlighting the benefits associated with targeting PCSK9. The observed reductions in myocardial infarction, coronary revascularisation, and ischemic stroke establish the role of PCSK9 monoclonal antibodies as a transformative strategy in the prevention of cardiovascular disease. The complex interplay between its mechanisms in achieving lower LDL-C levels, lipoprotein(a) lowering, and the longer-term benefits of the PCSK9 monoclonal antibodies provides an optimistic future for the role of PCSK9 monoclonal antibodies in the ongoing management of ASCVD in clinical practice.
Supplementary Materials
The following supporting information can be found at: https://www.sciepublish.com/article/pii/1058, Figure S1: Trial Sequential Analysis for Myocardial Infarction; Figure S2: Trial Sequential Analysis for Coronary Revascularisation; Figure S3: Trial Sequential Analysis for Ischemic Stroke; Figure S4: Trial Sequential Analysis for All-cause Mortality; Figure S5: Trial Sequential Analysis for Cardiovascular Death; Figure S6: Funnel Plot for Myocardial Infarction; Figure S7: Funnel Plot for Coronary Revascularisation; Figure S8: Funnel Plot for Ischaemic Stroke; Figure S9: Funnel Plot for All-cause Mortality; Figure S10: Funnel Plot for Cardiovascular Death; Figure S11: Funnel Plot for Hospitalisation for Heart Failure; Figure S12: Funnel Plot for Hospitalisation for Unstable Angina; Figure S13: Leave one out Analysis for Myocardial Infarction; Figure S14: Leave one out Analysis for Coronary Revascularisation; Figure S15: Leave one out Analysis for Ischemic Stroke; Figure S16: Leave one out Analysis for All-cause Mortality; Figure S17: Leave one out Analysis for Cardiovascular Death; Table S1: Search Strategy; Table S2: Summary of studies that met inclusion criteria; Table S3: Risk of Bias—Joanna Briggs Institute Tool for Randomised Controlled Trials; Table S4: Bayesian Meta-analysis Results for Myocardial Infarction; Table S5: Bayesian Meta-analysis Results for Coronary Revascularisation; Table S6: Bayesian Meta-analysis Results for Ischemic Stroke; Table S7: Bayesian Meta-analysis Results for All-cause Mortality; Table S8: Bayesian Meta-analysis Results for Cardiovascular Death.
Author Contributions
Conceptualization, J.G. and T.T.; Methodology, J.G., W.Y., A.A. and P.S.; Software, D.T.; Validation, P.S.; Formal Analysis, J.G. and D.T.; Investigation, J.G., W.Y., A.A., A.L. and P.S.; Data Curation, J.G., W.Y. and A.L.; Writing—Original Draft Preparation, J.G.; Writing—Review & Editing, J.G., R.J., D.T. and T.T.; Visualization, J.G., R.J. and D.T.; Supervision, T.T.; Project Administration, J.G. and T.T.
Ethics Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that supports the findings of this study are available with the corresponding author, [T.T.], upon reasonable request.
Funding
This research received no external funding.
Declaration of Competing Interest
T.T. received grant funding for an investigator-led and -designed research project from Amgen. He has also received honoraria from Bayer, Novartis, GSK, and Amgen for speaker and advisory board engagements unrelated to this project. All other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
Vaduganathan M, Mensah GA, Turco JV, Fuster V, Roth GA. The Global Burden of Cardiovascular Diseases and Risk. J. Am. Coll. Cardiol. 2022, 80, 2361–2371. DOI:10.1016/j.jacc.2022.11.005 [Google Scholar]
-
Tokgözoğlu L, Libby P. The dawn of a new era of targeted lipid-lowering therapies. Eur. Heart J. 2022, 43, 3198–3208. DOI:10.1093/eurheartj/ehab841 [Google Scholar]
-
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2019, 41, 111–188. DOI:10.1093/eurheartj/ehz455 [Google Scholar]
-
Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, 25. DOI:10.1161/CIR.0000000000000625 [Google Scholar]
-
Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278. DOI:10.1016/S0140-6736(05)67394-1 [Google Scholar]
-
Ray KK, Molemans B, Schoonen WM, Giovas P, Bray S, Kiru G, et al. EU-Wide Cross-Sectional Observational Study of Lipid-Modifying Therapy Use in Secondary and Primary Care: The DA VINCI study. Eur. J. Prev. Cardiol. 2020, 28, 1279–1289. DOI:10.1093/eurjpc/zwaa047 [Google Scholar]
-
Alsadat N, Hyun K, Boroumand F, Juergens C, Kritharides L, Brieger DB. Achieving lipid targets within 12 months of an acute coronary syndrome: An observational analysis. Med. J. Aust. 2022, 216, 463–468. DOI:10.5694/mja2.51442 [Google Scholar]
-
Vallejo-Vaz AJ, Stevens CAT, Lyons ARM, Dharmayat KI, Freiberger T, Hovingh GK, et al. Global perspective of familial hypercholesterolaemia: A cross-sectional study from the EAS Familial Hypercholesterolaemia Studies Collaboration (FHSC). Lancet 2021, 398, 1713–1725. DOI:10.1016/S0140-6736(21)01122-3 [Google Scholar]
-
Talic S, Marquina C, Ofori-Asenso R, Petrova M, Liew D, Owen AJ, et al. Switching, Persistence and Adherence to Statin Therapy: A Retrospective Cohort Study Using the Australian National Pharmacy Data. Cardiovasc. Drugs Ther. 2022, 36, 867–877. DOI:10.1007/s10557-021-07199-7 [Google Scholar]
-
Seidah NG, Awan Z, Chrétien M, Mbikay M. PCSK9. Circ. Res. 2014, 114, 1022–1036. DOI:10.1161/CIRCRESAHA.114.301621 [Google Scholar]
-
Sabatine MS. PCSK9 inhibitors: Clinical evidence and implementation. Nat. Rev. Cardiol. 2019, 16, 155–165. DOI:10.1038/s41569-018-0107-8 [Google Scholar]
-
Stoekenbroek RM, Lambert G, Cariou B, Hovingh GK. Inhibiting PCSK9—Biology beyond LDL control. Nat. Rev. Endocrinol. 2019, 15, 52–62. DOI:10.1038/s41574-018-0110-5 [Google Scholar]
-
Rosenson Robert S, Hegele Robert A, Fazio S, Cannon Christopher P. The Evolving Future of PCSK9 Inhibitors. J. Am. Coll. Cardiol. 2018, 72, 314–329. DOI:10.1016/j.jacc.2018.04.054 [Google Scholar]
-
Karatasakis A, Danek BA, Karacsonyi J, Rangan BV, Roesle MK, Knickelbine T, et al. Effect of PCSK9 Inhibitors on Clinical Outcomes in Patients with Hypercholesterolemia: A Meta-Analysis of 35 Randomized Controlled Trials. J. Am. Heart Assoc. 2017, 6, e006910. DOI:10.1161/JAHA.117.006910 [Google Scholar]
-
Sabatine MS, Giugliano RP, Keech AC, Narimon H, Wiviott SD, Murphy SA, et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. DOI:10.1056/NEJMoa1615664 [Google Scholar]
-
Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. DOI:10.1056/NEJMoa1801174 [Google Scholar]
-
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. DOI:10.1136/bmj.n160 [Google Scholar]
-
Barker TH, Stone JC, Sears K, Klugar M, Tufanaru C, Leonardi-Bee J, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid. Synth. 2023, 21, 494–506. DOI:10.11124/JBIES-22-00430 [Google Scholar]
-
Blom DJ, Hala T, Bolognese M, Lillestol MJ, Toth PD, Burgess L, et al. A 52-Week Placebo-Controlled Trial of Evolocumab in Hyperlipidemia. N. Engl. J. Med. 2014, 370, 1809–1819. DOI:10.1056/NEJMoa1316222 [Google Scholar]
-
Ginsberg HN, Rader DJ, Raal FJ, Guyton JR, Baccara-dinet MT, Lorenzato C, et al. Efficacy and Safety of Alirocumab in Patients with Heterozygous Familial Hypercholesterolemia and LDL-C of 160 mg/dl or Higher. Cardiovasc. Drugs Ther. 2016, 30, 473–483. DOI:10.1007/s10557-016-6685-y [Google Scholar]
-
Kastelein JJP, Ginsberg HN, Langslet G, Kees Hovingh G, Ceska R, Dufour R, et al. ODYSSEY FH I and FH II: 78 week results with alirocumab treatment in 735 patients with heterozygous familial hypercholesterolaemia. Eur. Heart J. 2015, 36, 2996–3003. DOI:10.1093/eurheartj/ehv370 [Google Scholar]
-
Kereiakes DJ, Robinson JG, Cannon CP, Lorenzato C, Pordy R, Chaudhari U, et al. Efficacy and safety of the proprotein convertase subtilisin/kexin type 9 inhibitor alirocumab among high cardiovascular risk patients on maximally tolerated statin therapy: The ODYSSEY COMBO I study. Am. Heart J. 2015, 169, 906–915.e13. DOI:10.1016/j.ahj.2015.03.004 [Google Scholar]
-
Robinson JG, Farnier M, Krempf M, Bergeron J, Luc G, Averna M, et al. Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events. N. Engl. J. Med. 2015, 372, 1489–1499. DOI:10.1056/NEJMoa1501031 [Google Scholar]
-
Nicholls SJ, Puri R, Anderson TJ, Ballantyne CM, Cho L, Kastelein JJP, et al. Effect of Evolocumab on Progression of Coronary Disease in Statin-Treated Patients: The GLAGOV Randomized Clinical Trial. JAMA 2016, 316, 2373–2384. DOI:10.1001/jama.2016.16951 [Google Scholar]
-
Räber L, Ueki Y, Otsuka T, Losdat S, Häner JD, Lonborg J, et al. Effect of Alirocumab Added to High-Intensity Statin Therapy on Coronary Atherosclerosis in Patients with Acute Myocardial Infarction: The PACMAN-AMI Randomized Clinical Trial. JAMA 2022, 327, 1771–1781. DOI:10.1001/jama.2022.5218 [Google Scholar]
-
Teramoto T, Kobayashi M, Uno K, Takagi Y, Matsuoka O, Sugimoto M, et al. Efficacy and Safety of Alirocumab in Japanese Subjects (Phase 1 and 2 Studies). Am. J. Cardiol. 2016, 118, 56–63. DOI:10.1016/j.amjcard.2016.04.011 [Google Scholar]
-
Wang H-F, Mao Y-C, Xu X-Y, Zhao S-Y, Han D-D, Ge S-Y, et al. Effect of alirocumab and evolocumab on all-cause mortality and major cardiovascular events: A meta-analysis focusing on the number needed to treat. Front. Cardiovasc. Med. 2022, 9, 1016802. DOI:10.3389/fcvm.2022.1016802 [Google Scholar]
-
Wang X, Wen D, Chen Y, Ma L, You C. PCSK9 inhibitors for secondary prevention in patients with cardiovascular diseases: A bayesian network meta-analysis. Cardiovasc. Diabetol. 2022, 21, 107. DOI:10.1186/s12933-022-01542-4 [Google Scholar]
-
Bai J, Gong LL, Li QF, Wang ZH. Long-term efficacy and safety of proprotein convertase subtilisin/kexin 9 monoclonal antibodies: A meta-analysis of 11 randomized controlled trials. J. Clin. Lipidol. 2018, 12, 277–291.e3. DOI:10.1016/j.jacl.2018.01.004 [Google Scholar]
-
Schmidt AF, Carter J-PL, Pearce LS, Wilkins JT, Overington JP, Hingorani AD, et al. PCSK9 monoclonal antibodies for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2020, 2020, CD011748. DOI:10.1002/14651858.CD011748.pub3 [Google Scholar]
-
Khan SU, Yedlapati SH, Lone AN, Hao Q, Guyatt G, Delvaux N, et al. PCSK9 inhibitors and ezetimibe with or without statin therapy for cardiovascular risk reduction: A systematic review and network meta-analysis. BMJ 2022, 377, e069116. DOI:10.1136/bmj-2021-069116 [Google Scholar]
-
Cohen JC, Boerwinkle E, Mosley TH, Hobbs HH. Sequence Variations in PCSK9, Low LDL, and Protection against Coronary Heart Disease. N. Engl. J. Med. 2006, 354, 1264–1272. DOI:10.1056/NEJMoa054013 [Google Scholar]
-
Kent ST, Rosenson RS, Avery CL, Chen Y-DI, Correa A, Cummings SR, et al. PCSK9 Loss-of-Function Variants, Low-Density Lipoprotein Cholesterol, and Risk of Coronary Heart Disease and Stroke. Circ. Cardiovasc. Genet. 2017, 10, e001632. DOI:10.1161/CIRCGENETICS.116.001632 [Google Scholar]
-
Huang C-C, Fornage M, Lloyd-Jones DM, Wei GS, Boerwinkle E, Liu K. Longitudinal Association of PCSK9 Sequence Variations with Low-Density Lipoprotein Cholesterol Levels. Circ. Cardiovasc. Genet. 2009, 2, 354–361. DOI:10.1161/CIRCGENETICS.108.828467 [Google Scholar]
-
Giugliano RP, Wiviott SD, Blazing MA, De Ferrari GM, Park J-G, Murphy SA, et al. Long-term Safety and Efficacy of Achieving Very Low Levels of Low-Density Lipoprotein Cholesterol: A Prespecified Analysis of the IMPROVE-IT Trial. JAMA Cardiol. 2017, 2, 547–555. DOI:10.1001/jamacardio.2017.0083 [Google Scholar]
-
Giugliano RP, Pedersen TR, Park J-G, De Ferrari GM, Gaciong ZA, Ceska R, et al. Clinical efficacy and safety of achieving very low LDL-cholesterol concentrations with the PCSK9 inhibitor evolocumab: A prespecified secondary analysis of the FOURIER trial. Lancet 2017, 390, 1962–1971. DOI:10.1016/S0140-6736(17)32290-0 [Google Scholar]
-
Schwartz GG, Gabriel Steg P, Bhatt DL, Bittner VA, Diaz R, Goodman SG, et al. Clinical Efficacy and Safety of Alirocumab After Acute Coronary Syndrome According to Achieved Level of Low-Density Lipoprotein Cholesterol: A Propensity Score–Matched Analysis of the ODYSSEY OUTCOMES Trial. Circulation 2021, 143, 1109–1122. DOI:10.1161/CIRCULATIONAHA.120.049447 [Google Scholar]
-
Gaba P, O’Donoghue ML, Park J-G, Wiviott SD, Atar D, Kuder JF, et al. Association Between Achieved Low-Density Lipoprotein Cholesterol Levels and Long-Term Cardiovascular and Safety Outcomes: An Analysis of FOURIER-OLE. Circulation 2023, 147, 1192–1203. DOI:10.1161/CIRCULATIONAHA.122.063399 [Google Scholar]
-
Giugliano RP, Mach F, Zavitz K, Kurtz C, Im K, Kanevsky E, et al. Cognitive Function in a Randomized Trial of Evolocumab. N. Engl. J. Med. 2017, 377, 633–643. DOI:10.1056/NEJMoa1701131 [Google Scholar]
-
Janik MJ, Urbach DV, van Nieuwenhuizen E, Zhao J, Yellin O, Baccara-Dinet MT, et al. Alirocumab treatment and neurocognitive function according to the CANTAB scale in patients at increased cardiovascular risk: A prospective, randomized, placebo-controlled study. Atherosclerosis 2021, 331, 20–27. DOI:10.1016/j.atherosclerosis.2021.06.913 [Google Scholar]
-
Patti G, Spinoni EG, Grisafi L, Mehran R, Mennuni M. Safety and efficacy of very low LDL-cholesterol intensive lowering: A meta-analysis and meta-regression of randomized trials. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 9, 138–147. DOI:10.1093/ehjcvp/pvac049 [Google Scholar]
-
Brandts J, Ray KK. Low Density Lipoprotein Cholesterol–Lowering Strategies and Population Health. Circulation 2020, 141, 873–876. DOI:10.1161/CIRCULATIONAHA.119.043406 [Google Scholar]
-
Robinson JG. Starting Primary Prevention Earlier with Statins. Am. J. Cardiol. 2014, 114, 1437–1442. DOI:10.1016/j.amjcard.2014.07.076 [Google Scholar]
-
Bohula EA, Giugliano RP, Leiter LA, Verma S, Park J-G, Sever PS, et al. Inflammatory and Cholesterol Risk in the FOURIER Trial. Circulation 2018, 138, 131–140. DOI:10.1161/CIRCULATIONAHA.118.034032 [Google Scholar]
-
Simantiris S, Antonopoulos AS, Papastamos C, Benetos G, Koumallos N, Tsioufis K, et al. Lipoprotein(a) and inflammation- pathophysiological links and clinical implications for cardiovascular disease. J. Clin. Lipidol. 2023, 17, 55–63. DOI:10.1016/j.jacl.2022.10.004 [Google Scholar]
-
Nordestgaard BG, Langsted A. Lipoprotein(a) as a cause of cardiovascular disease: Insights from epidemiology, genetics, and biology. J. Lipid Res. 2016, 57, 1953–1975. DOI:10.1194/jlr.R071233 [Google Scholar]
-
Bittner VA, Szarek M, Aylward PE, Bhatt DL, Diaz R, Edelberg JM, et al. Effect of Alirocumab on Lipoprotein(a) and Cardiovascular Risk After Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2020, 75, 133–144. DOI:10.1016/j.jacc.2019.10.057 [Google Scholar]
-
Filippatos TD, Kei A, Rizos CV, Elisaf MS. Effects of PCSK9 Inhibitors on Other Than Low-Density Lipoprotein Cholesterol Lipid Variables. J. Cardiovasc. Pharmacol. Ther. 2018, 23, 3–12. DOI:10.1177/1074248417724868 [Google Scholar]
-
Pérez de Isla L, Díaz-Díaz JL, Romero MJ, Muñiz-Grijalvo O, Mediavilla JD, Argüeso R, et al. Alirocumab and Coronary Atherosclerosis in Asymptomatic Patients with Familial Hypercholesterolemia: The ARCHITECT Study. Circulation 2023, 147, 1436–1443. DOI:10.1161/CIRCULATIONAHA.122.062557 [Google Scholar]
-
O’Donoghue ML, Giugliano RP, Wiviott SD, Atar D, Keech A, Kuder JF, et al. Long-Term Evolocumab in Patients with Established Atherosclerotic Cardiovascular Disease. Circulation 2022, 146, 1109–1119. DOI:10.1161/CIRCULATIONAHA.122.061620 [Google Scholar]
-
Ray KK, Wright RS, Kallend D, Koenig W, Leiter LA, Raal FJ, et al. Two Phase 3 Trials of Inclisiran in Patients with Elevated LDL Cholesterol. N. Engl. J. Med. 2020, 382, 1507–1519. DOI:10.1056/NEJMoa1912387 [Google Scholar]
-
O’Donoghue ML, Rosenson RS, Gencer B, López JAG, Lepor NE, Baum SJ, et al. Small Interfering RNA to Reduce Lipoprotein(a) in Cardiovascular Disease. N. Engl. J. Med. 2022, 387, 1855–1864. DOI:10.1056/NEJMoa2211023 [Google Scholar]
-
Liu C, Chen J, Chen H, Zhang T, He D, Luo Q, et al. PCSK9 Inhibition: From Current Advances to Evolving Future. Cells 2022, 11, 2972. DOI:10.3390/cells11192972 [Google Scholar]
-
Kazi DS, Moran AE, Coxson PG, Penko J, Ollendorf DA, Pearson S, et al. Cost-effectiveness of PCSK9 Inhibitor Therapy in Patients with Heterozygous Familial Hypercholesterolemia or Atherosclerotic Cardiovascular Disease. JAMA 2016, 316, 743–753. DOI:10.1001/jama.2016.11004 [Google Scholar]
-
Arrieta A, Hong JC, Khera R, Virani SS, Krumholz HM, Nasir K. Updated Cost-effectiveness Assessments of PCSK9 Inhibitors from the Perspectives of the Health System and Private Payers: Insights Derived from the FOURIER Trial. JAMA Cardiol. 2017, 2, 1369–1374. DOI:10.1001/jamacardio.2017.3655 [Google Scholar]
-
Mercep I, Strikic D, Hrabac P, Pecin I, Reiner Ž. PCSK9 inhibition: From effectiveness to cost-effectiveness. Front. Cardiovasc. Med. 2024, 11, 1339487. DOI:10.3389/fcvm.2024.1339487 [Google Scholar]
-
Muntner P, Ghazi L, Jones J, Dhalwani N, Poudel B, Wen Y, et al. Persistence and Adherence to PCSK9 Inhibitor Monoclonal Antibodies Versus Ezetimibe in Real-World Settings. Adv. Ther. 2024, 41, 2399–2413. DOI:10.1007/s12325-024-02868-z [Google Scholar]
-
Ye X, Zhang S, Zhong X, Li M, Liu M, Zhuang X, et al. Real-World Assessment of the Association Between PCSK9i Adherence and LDL Reduction and Variability in a Chinese Clinical Practice. Clin. Epidemiol. 2025, 17, 537–546. DOI:10.2147/CLEP.S507761 [Google Scholar]