1. Introduction
In recent years, probiotics, defined as live microorganisms that confer health benefits to the host when administered in adequate amounts, have garnered immense popularity. Marketed as miracle supplements capable of curing everything from digestive ailments to depression, probiotics have become a multi-billion-dollar industry. However, while compelling evidence supports their use in specific clinical contexts, the current scientific consensus does not support the notion that they are a panacea for all diseases. A methodology to guide this scientific opinion and so that we can discuss the pros and cons, clinical trials, possible mechanisms, and the lack of evidence for these mechanisms, we established some methodological criteria that consisted of selecting review manuscripts, systematic reviews, and meta-analyses published in the last five years, except two of them among the nineteen published in the previous decade.
2. The Promises: Evidence-Based Benefits
The strongest clinical evidence for probiotic efficacy lies in gastrointestinal (GI) disorders. Randomized controlled trials (RCTs) have demonstrated that certain strains, such as
Lactobacillus rhamnosus and
Saccharomyces boulardii, can reduce the duration of infectious diarrhea and prevent antibiotic-associated diarrhea, including
Clostridioides difficile infection [
1]. These effects are likely mediated through mechanisms such as pathogen inhibition via antimicrobial production, immune modulation, and restoration of gut microbiota balance [
2].
Emerging research also suggests potential benefits in irritable bowel syndrome (IBS), where some multispecies probiotic formulations show modest symptom improvement [
3]. Additionally, early studies indicate possible roles in managing inflammatory bowel disease (IBD), particularly ulcerative colitis, though results remain mixed and strain-specific [
4].
Beyond the gut, preliminary findings suggest that certain probiotics may influence systemic immunity, with some studies reporting reduced incidence and duration of upper respiratory tract infections [
5]. There is also intriguing but limited evidence linking probiotic use to mental health improvements via the gut-brain axis, an area known as psychobiotics [
6]. However, these findings are largely observational or derived from small trials and require further validation.
summarizes currently understood evidence per condition.
. Evidence for probiotic efficacy across diseases, visualized using a traffic-light system with scaled bar lengths reflecting strength: strong (100%), moderate (65%), limited (40%), weak (20%). Conditions with insufficient evidence are marked with a

symbol. Icons represent organ systems: Green Heart = gut, Red Heart = metabolic, Lungs = respiratory, Pregnant Woman = pediatric, Brain = mental health. Probiotic benefits are largely confined to gastrointestinal applications, with little proven impact on metabolic or mental health. Source: Analysis of recent meta-analyses and Cochrane reviews [
1,
3,
4,
5,
7,
8,
9,
10,
11].
3. The Pitfalls: Overstated Claims and Lack of Standardization
Despite these promising areas, the enthusiasm surrounding probiotics often outpaces science. One major issue is the heterogeneity of probiotic products. Different strains exert different physiological effects, yet many commercial products contain undefined or poorly characterized bacterial mixtures [
12]. This lack of standardization makes it difficult to extrapolate findings from one study to another or real-world applications.
Moreover, the mechanisms underlying probiotic action are not fully understood. While proposed pathways include competitive exclusion of pathogens, immune system modulation, and production of bioactive metabolites like short-chain fatty acids, direct evidence linking these mechanisms to clinical outcomes remains sparse [
13]. In many cases, observed health benefits correlate weakly with measurable changes in gut microbiota composition, raising questions about causality versus association [
14].
4. Clinical Trials: Mixed Results and Methodological Limitations
A significant number of clinical trials on probiotics suffer from methodological flaws. Many are underpowered, lack placebo controls, or fail to account for confounding variables such as diet, medication use, and baseline microbiome composition. Furthermore, publication bias favors positive results, leading to overrepresentation of beneficial effects in the literature [
15,
16].
Meta-analyses and systematic reviews offer a more balanced perspective. For instance, a 2023 Cochrane review titled “Probiotics for the prevention of Clostridium difficile-associated diarrhoea in adults and children” concluded that while probiotics may reduce the risk of
C. difficile-associated diarrhea, the quality of evidence was low to moderate [
7]. Similarly, a meta-analysis published in TP (Transl Pediatr) in 2021 found only modest reductions in the duration of acute gastroenteritis among children treated with probiotics, effects that varied significantly by strain and dosage [
8].
The evidence is even weaker for conditions such as obesity, metabolic syndrome, and psychiatric disorders. Although animal models and pilot human studies suggest potential benefits, large-scale RCTs have consistently failed to replicate these findings [
9,
10]. As a result, regulatory bodies such as the European Food Safety Authority (EFSA) have rejected numerous probiotic health claims due to insufficient evidence [
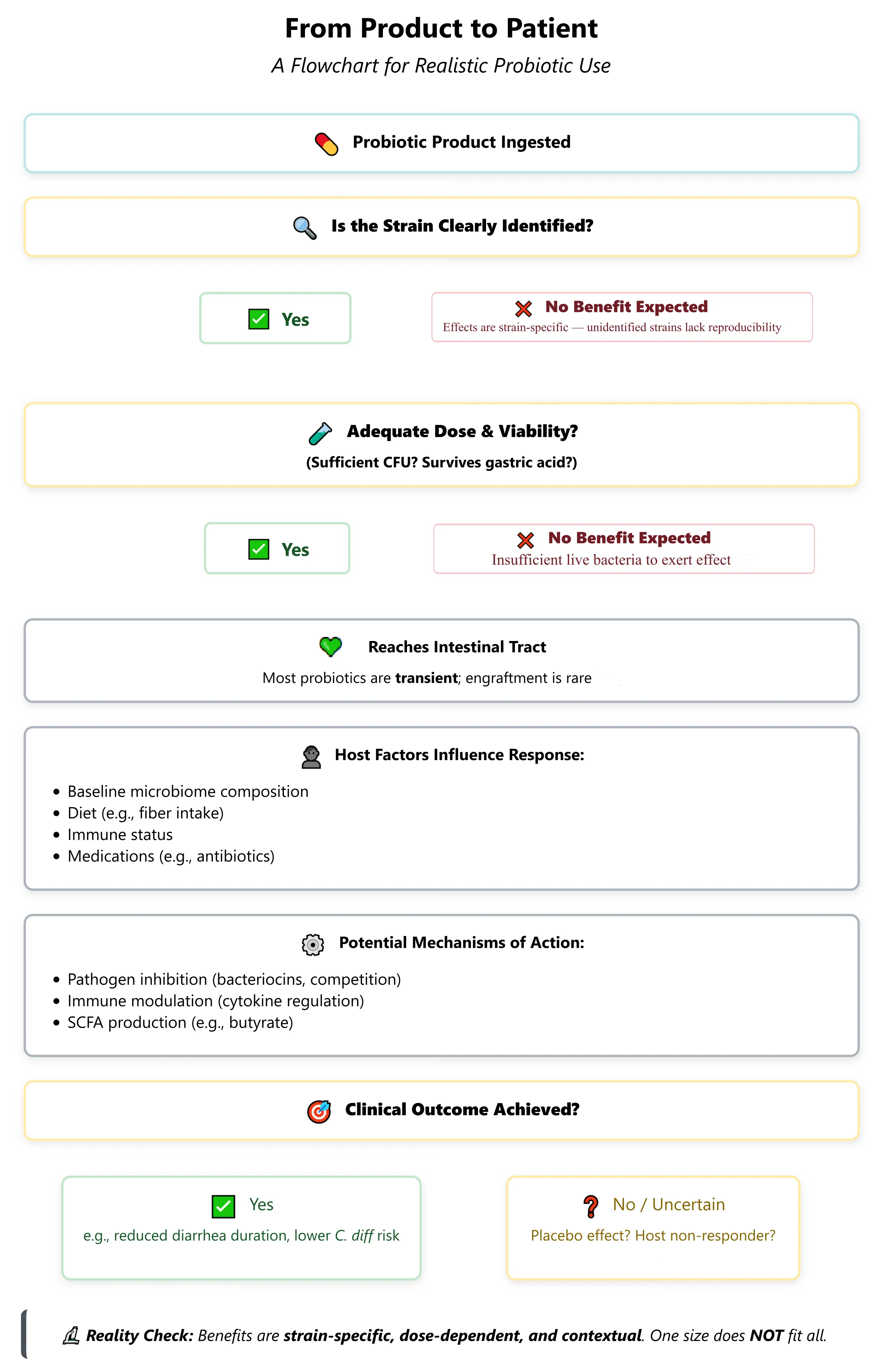
11]. contains a decision-making flowchart on whether or not a probiotic can be recommended based on the availability of clinical evidence of its action.
. A realistic probiotic action pathway illustrates the journey from product intake to clinical outcome. Critical checkpoints include strain identification, viability, host factors, and measurable mechanisms. Most probiotics do not engraft permanently [
17], and clinical benefits are modest and context-dependent. Outcomes are most consistent for gastrointestinal conditions such as antibiotic-associated diarrhea [
1,
12]. Source: Synthesis of clinical and mechanistic studies [
2,
7,
8,
18,
19].
5. The Placebo Effect and Consumer Misconceptions
Another often-overlooked factor is the placebo effect. Many individuals report subjective improvements after taking probiotics, which may be attributable to psychological expectations rather than biological mechanisms [
19]. This phenomenon is compounded by aggressive marketing campaigns that position probiotics as “natural” and inherently safe, despite documented fungemia and bacteremia associated with their use in immunocompromised individuals [
17].
Furthermore, the assumption that probiotics permanently colonize the gut and correct microbial imbalances is largely unfounded. Recent metagenomic studies indicate that most probiotic strains transiently pass through the GI tract without engrafting, suggesting that sustained benefits, if any, require continuous administration [
18].
6. Conclusions
It is not a Panacea but a Promising Tool. Probiotics are not a universal cure-all. Their effectiveness is context-dependent, strain-specific, and often modest in magnitude. While they hold promise in select clinical scenarios—particularly in preventing antibiotic-associated diarrhea and managing certain GI disorders—the evidence does not support their indiscriminate use across various diseases.
Future research must focus on identifying the right strains, dosages, and patient populations most likely to benefit from probiotics. Advances in personalized medicine, including microbiome profiling and biomarker discovery, may help tailor probiotic interventions to individual needs. Until then, clinicians and consumers alike should approach probiotics with cautious optimism, recognizing both their potential and limitations.
In sum, probiotics represent a valuable addition to the therapeutic arsenal but not a panacea. Scientific rigor, transparency, and critical evaluation are essential to ensure their use is guided by evidence, not hype.
Acknowledgments
We would like to thank CNPq for paying me a scientific productivity grant and for financing our work with probiotics with other agencies, such as FAPEMIG and CAPES.
Author Contributions
Conceptualization, C.R.G. and V.A.; Investigation, V.A.; Data Curation, C.R.G. and V.A.; Writing—Original Draft Preparation, V.A.; Writing—Review & Editing, C.R.G. and V.A.; Visualization, C.R.G.; Supervision, V.A.
Ethics Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting this opinion piece are available within the article, its references or upon request.
Funding
No direct funding to make this manuscript.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
1.
Goodman C, Keating G, Georgousopoulou E, Hespe C, Levett K, Tang MLK. Probiotics for the prevention of antibiotic-associated diarrhea: A systematic review and meta-analysis.
BMJ Open 2021,
11, e043054. doi:10.1136/bmjopen-2020-043054.
[Google Scholar]
-
2.
Zeng Q, Li P, Wu H, Zhuang Y, Zhang Y, Asemani S, et al. Probiotics and gastrointestinal disorders: an umbrella meta-analysis of therapeutic efficacy.
Eur. J. Med. Res. 2025,
30, 515. doi:10.1186/s40001-025-02788-w.
[Google Scholar]
-
3.
Ford AC, Moayyedi P, Chey WD, Harris LA, Lacy BE, Saito YA, et al. American College of Gastroenterology monograph on the management of irritable bowel syndrome.
Am. J. Gastroenterol. 2021,
116, 17–31. doi:10.1038/s41395-018-0084-x.
[Google Scholar]
-
4.
Chappell KD, Olayinka L, Sutton R, Seow C, Debruyn J, van Zanten S, et al. A framework for clinical care pathway renewal: An example from inflammatory bowel disease.
BMC Med. Res. Methodol. 2025,
25, 173. doi:10.1186/s12874-025-02616-z.
[Google Scholar]
-
5.
King S, Glanville J, Sanders ME, Fitzgerald A, Dicksved J. Effectiveness of probiotics on the duration of illness in healthy children and adults who develop common acute respiratory infectious conditions: Systematic review and meta-analysis.
Br. J. Nutr. 2021,
125, 523–534. doi:10.3390/nu16091352.
[Google Scholar]
-
6.
Mosquera FEC, Lizcano Martinez S, Liscano Y. Effectiveness of Psychobiotics in the Treatment of Psychiatric and Cognitive Disorders: A Systematic Review of Randomized Clinical Trials.
Nutrients 2024,
16, 1352. doi:10.3390/nu16091352.
[Google Scholar]
-
7.
Goldenberg JZ, Yap C, Lytvyn L, Lo CKF, Beardsley J, Mertz D, et al. Probiotics for the prevention of Clostridioides difficile-associated diarrhoea in adults and children.
Cochrane Database Syst. Rev. 2023,
4,
CD006095. doi:10.1002/14651858.CD006095.pub5.
[Google Scholar]
-
8.
Huang R, Xing HY, Liu HJ, Chen ZF, Tang BB. Efficacy of probiotics in the treatment of acute diarrhea in children: A systematic review and meta-analysis of clinical trials.
Transl. Pediatr. 2021,
10, 3248–3260. doi:10.21037/tp-21-511.
[Google Scholar]
-
9.
Everard A, Belzer C, Geurts L, Ouwerkerk JP, Druart C, Bindels LB, et al. Cross-talk between
Akkermansia muciniphila and intestinal epithelium controls diet-induced obesity.
Proc. Natl. Acad. Sci. USA 2013,
110, 9066–9071. doi:10.1073/pnas.1219451110.
[Google Scholar]
-
10.
Cocean A-M, Vodnar DC. Exploring the gut-brain Axis: Potential therapeutic impact of Psychobiotics on mental health.
Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2024,
134, 111073. doi:10.1016/j.pnpbp.2024.111073.
[Google Scholar]
-
11.
Slykerman RF, Davies N, Donohoe R. Evaluating the scientific evidence to support mental health and well-being claims made on probiotic products.
Nutr. Health 2025. doi:10.1177/02601060241305682.
[Google Scholar]
-
12.
Zawistowska-Rojek A, Zaręba T, Tyski S. Microbiological Testing of Probiotic Preparations.
Int. J. Environ. Res. Public. Health 2022,
19, 5701. doi:10.3390/ijerph19095701.
[Google Scholar]
-
13.
Vijayaganapathi A, Mohanasrinivasan V. A Review of Next-Generation Probiotics—As a Gateway to Biotherapeutics.
Probiotics Antimicrob. Prot. 2025. doi:10.1007/s12602-025-10606-2.
[Google Scholar]
-
14.
Zmora N, Suez J, Elinav E. You are what you eat: diet, health and the gut microbiota.
Nat. Rev. Gastroenterol. Hepatol. 2019,
16, 35–56. doi:10.1038/s41575-018-0061-2.
[Google Scholar]
-
15.
Khoruts A, Hoffmann D, Britton RA. Probiotics: Promise, Evidence, and Hope.
Gastroenterology 2020,
159, 409–413. doi:10.1053/j.gastro.2020.05.058.
[Google Scholar]
-
16.
Ruszkowski J, Majkutewicz K, Rybka E, Kutek M, Dębska-Ślizień A, Witkowski JM. The methodological quality and clinical applicability of meta-analyses on probiotics in 2020: A cross-sectional study.
Biomed. Pharmacother. 2021,
142, 112044. doi:10.1016/j.biopha.2021.112044.
[Google Scholar]
-
17.
Falzone L, Lavoro A, Candido S, Salmeri M, Zanghì A, Libra M. Benefits and concerns of probiotics: an overview of the potential genotoxicity of the colibactin-producing Escherichia coli Nissle 1917 strain.
Gut Microbes 2024,
16, 2397874. doi:10.1080/19490976.2024.2397874.
[Google Scholar]
-
18.
Ng KM, Aranda-Díaz A, Tropini C, Frankel MR, Van Treuren W, O’Loughlin CT, et al. Recovery of the Gut Microbiota after Antibiotics Depends on Host Diet, Community Context, and Environmental Reservoirs.
Cell Host Microbe 2019,
26, 650–665.e4; Erratum in Cell Host Microbe 2020, 28, 628. doi:10.1016/j.chom.2020.09.001.
[Google Scholar]
-
19.
Moayyedi P, Ford AC, Talley NJ, Cremonini F, Foxx-Orenstein AE, Brandt LJ, et al. The efficacy of probiotics in the treatment of irritable bowel syndrome: Systematic review and meta-analysis.
BMJ 2010,
340, c2609. doi:10.1136/gut.2008.167270.
[Google Scholar]