2.1. Early Trials Demonstrating Symptomatic and Functional Benefits
MUSTIC (1990s) trial: provided initial evidence that CRT significantly improved exercise capacity, quality of life (QOL), and oxygen consumption in patients with severe heart failure and conduction delay. In the MUSTIC study, there was a 23% improvement in six-minute walk distance (6MWD), and QOL scores were observed when the left ventricular (LV) lead was active compared to periods when the LV lead was present but deactivated [
5]. MIRACLE trial (2002): included a larger cohort of 453 patients with moderate-to-severe left ventricular systolic dysfunction (LVSD) and reinforced CRT’s clinical value, showing a 18-point increase in QOL scores (MLHFQ) and 39-m improvement in 6MWD [
6,
7].
2.2. CRT Impact on Survival and Hospitalisation
COMPANION (2004–2005) addressed the gap in its impact on survival. In this trial of 1520 patients with NYHA class III or class IV heart failure, CRT with or without a defibrillator significantly reduced all-cause mortality and heart failure hospitalisation. Specifically, CRT-D reduced mortality by 36%, and Cardiac resynchronisation therapy pacemaker (CRT-P) reduced hospitalisation by 21%, establishing CRT as a critical intervention in advanced heart failure [
8].
CARE-HF (2005) further cemented CRT’s survival benefit in patients with more severe heart failure (NYHA class III/IV and LVEF ≤ 35%), showing a 36% reduction in all-cause mortality and 32% reduction in heart failure hospitalisation, solidifying CRT as a key therapy in reducing morbidity and mortality [
9].
2.3. Expanding CRT to Milder Symptoms and Broader Populations
MADIT-CRT (2009): expanded CRT’s utility to those with milder symptoms (NYHA class I/II). In this study, CRT-D reduced heart failure events by 41% and improved cardiac remodelling, showing CRT’s preventive benefit even in less symptomatic patients [
10].
RAFT (2009): extended these findings by demonstrating significant reductions in both mortality and hospitalisations in patients with mild-to-moderate heart failure, supporting the broader use of CRT in diverse heart failure populations [
11].
2.4. Special Populations and Contemporary Trials
BLOCK HF trial (2013) further extended CRT’s application by exploring its benefit in patients with heart failure and atrioventricular (AV) block. The trial randomised patients to receive either standard right ventricular (RV) pacing or biventricular pacing (CRT-P). The results showed that CRT-P significantly reduced the risk of death or heart failure-related urgent care compared to RV pacing. This trial highlighted CRT’s advantage over traditional pacing in patients with AV block, further broadening its therapeutic scope in managing heart failure, particularly for those who require ventricular pacing over a 2-year follow-up period.
The APAF-CRT trial addressed the gap in evidence for patients with symptomatic permanent atrial fibrillation (AF) that persisted for more than 6 months, narrow QRS complex, and recent heart failure hospitalisation. This multicentre, prospective, randomised study explored the use of atrioventricular AV nodal ablation in combination with CRT to improve outcomes [
12]. The trial was divided into two overlapping phases to evaluate morbidity and mortality outcomes. In the morbidity phase, 102 patients with symptomatic permanent AF were randomised to either pharmacological rate control (heart rate < 110 bpm) or AV nodal ablation followed by biventricular pacing. Both groups received optimal heart failure therapy. After a median follow-up of 16 months, the ablation plus CRT group had a significantly lower rate of the primary composite outcome of death due to heart failure, heart failure hospitalisation, or worsening heart failure compared to the drug treatment group. The ablation plus CRT group also showed a notable reduction in the combined endpoint of death from any cause or heart failure hospitalisation and a 36% reduction in AF symptoms at one-year follow-up. In the mortality phase, 133 patients were followed for a median of 29 months. The primary endpoint of all-cause mortality occurred in 11% of patients in the ablation plus CRT group compared to 29% in the drug treatment group. At two years, mortality rates were 5% in the ablation plus CRT group versus 21% in the drug group, with corresponding four-year rates of 14% and 41%. The secondary endpoint, which combined all-cause mortality or heart failure hospitalisation, was also significantly lower in the ablation plus CRT group. These benefits extended across patients with both preserved and reduced ejection fractions, highlighting the broader applicability of CRT beyond traditional selection criteria. Importantly, the trial demonstrated that the improvement in outcomes was not solely due to ventricular rate control, which was present in both arms, but rather the ‘regularisation’ of ventricular rhythm achieved by AV node ablation. This ‘regularisation’ promotes more effective synchronisation between atrial and ventricular contractions, leading to enhanced haemodynamic stability and clinical benefits. This finding is clinically relevant because for patients admitted with heart failure and no clear additional rate or rhythm control strategies, such as AF ablation, AV nodal ablation may be considered a viable option. In this context, a CRT device should be offered upfront rather than standard RV pacing, regardless of baseline left ventricular function [
12].
BUDAPEST-CRT trial addressed patients with reduced ejection fraction (HFrEF < 35%) and a high burden of right ventricular pacing (>20%) [
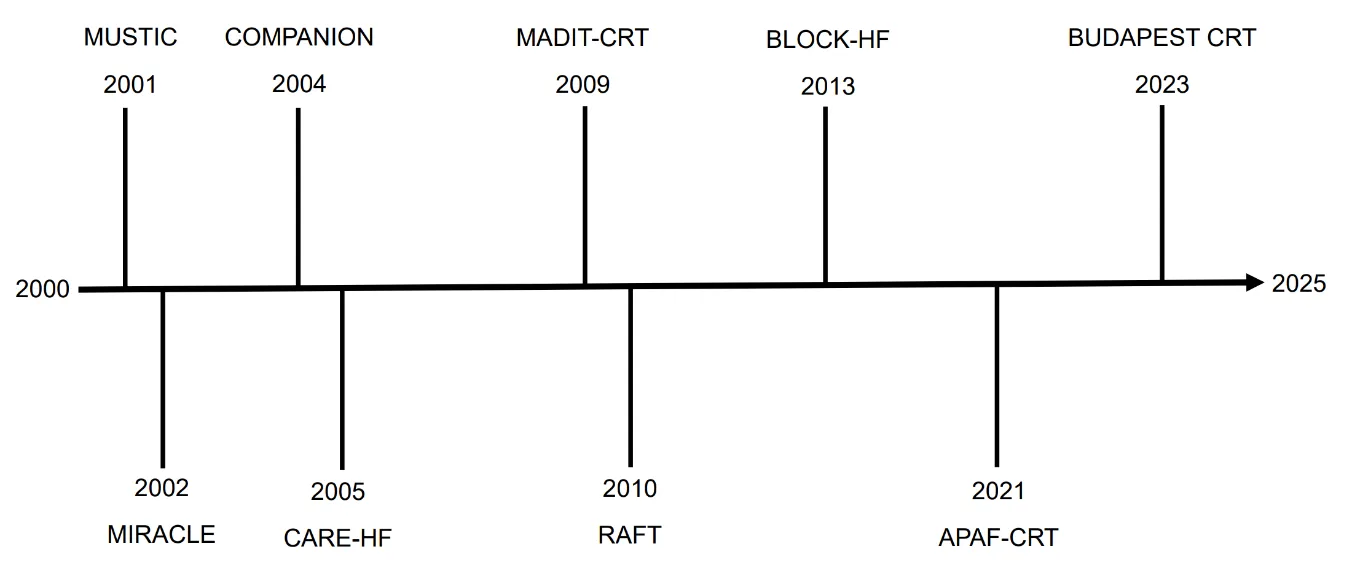
13]. This multicenter, prospective, randomised controlled trial enrolled 360 patients with an implanted pacemaker (PPM) or implantable cardioverter-defibrillator (ICD) for over six months and a wide QRS complex (>150 ms). Patients were randomised to either continue ICD therapy or undergo an upgrade to CRT-D. The composite primary outcome, which included all-cause death, heart failure hospitalisation, or less than a 15% decrease in end-systolic volume, occurred in 32.4% of the CRT-D arm compared to 78.9% in the ICD arm. The summary of trials are shown below in and a timeline of the trial data is illustrated in .
.
Table illustrating the contemporary trials related to CRT therapy, highlighting the number of patients, main endpoints measured and outcomes and conclusions.
| Trial |
Year |
Patients (n) |
Population |
Endpoints |
Outcomes & Conclusions |
| MUSTIC |
1990s |
100+ |
Severe HF, conduction delay |
6MWD, QOL |
+23% 6MWD, improved QOL |
| MIRACLE |
2002 |
453 |
Moderate-severe HF |
6MWD, MLHFQ QOL scores |
+39m 6MWD, +18 QOL score |
| COMPANION |
2004 |
1520 |
NYHA III–IV HF |
Mortality, HF hospitalisation |
−36% mortality (CRT-D), −21% hospitalisations (CRT-P) |
| CARE-HF |
2005 |
813 |
NYHA III–IV, LVEF ≤ 35% |
Mortality, HF hospitalisation |
−36% mortality, −32% hospitalisations |
| MADIT-CRT |
2009 |
1820 |
NYHA I–II, LVEF ≤ 30% |
HF events, remodelling |
−41% HF events, improved remodelling |
| RAFT |
2009 |
1798 |
NYHA II–III, LVEF ≤ 30% |
Mortality, HF hospitalisation |
Significant reduction in both |
| BLOCK-HF |
2013 |
691 |
AV block, HF |
Death, HF urgent care |
CRT-P superior to RV pacing |
| APAF-CRT |
2023 |
133 |
Permanent AF, narrow QRS |
Mortality, HF hospitalisation |
−16% mortality at 2 years |
| BUDAPEST-CRT |
2023 |
360 |
HFrEF < 35%, RV pacing > 20% |
Composite: mortality, HF events |
CRT-D superior to ICD therapy |
The CRT-D group showed marked improvement in heart failure symptoms, as quantified by a significant reduction in NYHA functional class compared to the ICD group. A greater proportion of patients in the CRT-D group shifted to a lower NYHA class, indicating a significant reduction in heart failure symptoms and improvement in exercise tolerance. This trial confirmed that upgrading to CRT-D is highly beneficial for patients with high RV pacing burdens and severe heart failure, reducing clinical events and improving quality of life.
Additionally, the CRT-D group showed an improvement in left ventricular end-diastolic volume, further supporting the benefits of upgrading to CRT-D in this patient population.
Despite the positive results, several caveats should be considered. The primary composite outcome included both hard endpoints (such as death and hospitalisations) and a soft endpoint (LV end-systolic volume reduction), raising the question of whether a change in LV volume is clinically meaningful if patients do not experience symptom relief. Moreover, the follow-up period was relatively short at 12 months, limiting the understanding of long-term outcomes. Additionally, neither clinicians nor patients were blinded to the treatment arms, introducing potential bias in the assessment of clinical outcomes.
From a clinical standpoint, the findings suggest that patients with PPM-induced cardiomyopathy should be considered for an immediate upgrade to CRT-D rather than deferring until device replacement. Although adverse event rates were similar between the CRT-D and ICD groups during the study period, long-term data, especially on risks like infection, are lacking and should be considered when making treatment decisions.
. Timeline of pivotal and contemporary trials related to cardiac resynchronisation therapy.
2.4.1. CRT in Specific Situations
CRT is indicated primarily for patients with HFrEF and evidence of electrical dyssynchrony, particularly those with left bundle branch block (LBBB) and a QRS duration of 150 ms or more. Current guidelines recommend CRT for patients with NYHA class II–IV symptoms, an LVEF of 35% or less, and sinus rhythm with wide QRS [
8,
9]. Additional indications include patients with atrial fibrillation (AF) requiring atrioventricular (AV) nodal ablation and those with high-burden right ventricular pacing, where CRT can prevent pacing-induced cardiomyopathy. Despite these well-defined indications, CRT response varies significantly, with up to 30% of patients classified as “non-responders” [
12]. Therefore, optimising patient selection requires consideration of additional predictive factors beyond QRS duration alone [
13].
Electrically, QRS morphology plays a crucial role in CRT response, with LBBB associated with the greatest benefit, while non-LBBB patterns, such as right bundle branch block (RBBB) and intraventricular conduction delay (IVCD), are linked to diminished outcomes [
14,
15]. The aetiology of heart failure also plays a role in CRT response, with non-ischaemic cardiomyopathy (NICM) patients generally responding better than those with ischaemic cardiomyopathy (ICM), likely due to lower scar burden and greater myocardial viability. Furthermore, functional mitral regurgitation (MR) severity has been linked to CRT outcomes, with patients exhibiting moderate MR showing the most significant improvements due to LV reverse remodelling. In patients with atrial fibrillation, CRT is particularly beneficial when AV nodal ablation is performed, ensuring a high percentage of effective biventricular pacing [
16,
17].
2.4.2. Adult Congenital Heart Disease
Heart failure remains the leading cause of death in adults with congenital heart disease (ACHD).. As experience with CRT improves, it has been considered for subgroups such as ACHD, which may not meet conventional indication criteria. However, this comes with additional challenges, including selection of appropriate patients, likelihood of response in those with unusual anatomy and procedural difficulties. Evidence for CRT in the ACHD population is limited to small observational studies of a heterogenous population with varying anatomy and physiology. CRT was first applied to the population with congenital heart disease in the early 2000’s, as small studies of predominantly children with congenital heart disease emerged, suggesting improvement in ejection fraction and functional status [
15,
16]. Potential efficacy of CRT in ACHD was demonstrated in a study comparing CRT in this population versus patients with ischaemic and non-ischaemic cardiomyopathy. Similar heart failure hospitalisation and mortality rates were demonstrated between these groups [
17]. Further small retrospective observational studies have reiterated this optimism. In a study of 54 ACHD patients undergoing CRT, with a mean age of 46-years, 65% responded to CRT, defined as ≥5% absolute increase in LVEF or right ventricular fractional area of change. CRT was associated with significant improvement in QRS duration and NYHA functional class, and improvement in NHYA class persisted at late follow-up. Baseline QRS duration was the only predictor of CRT response (OR: 1.38 per 10-millisecond increase of QRS duration) [
18]. These were corroborated with findings in a similar group of ACHD patients (median age 47 years), demonstrating a 77% positive response rate to CRT, in terms of NYHA functional class or systemic ventricular ejection fraction over a median follow-up period of 2.6 years [
19]. Similar response rates were also identified by investigating adults with purely structural ACHD. No factors that predicted response to CRT were identified, including site of lead placement or whether conduction delay was in the failing ventricle. Surprisingly, QRS duration appeared to shorten more in non-responders to CRT, suggesting that the electromechanical association in this group is more complex [
20].
The largest multi-centre study investigating CRT in the systemic right ventricle (sRV) (
n = 80), predominantly in those with congenitally corrected transposition of the great arteries (ccTGA), showed that following insertion of CRT, NYHA functional class improved significantly, but with marginal improvement in sRV function pre- and post-CRT (30%
vs. 31%) in those already paced pre-CRT and hence undergoing device upgrade. QRS duration reduced significantly in those who were paced pre-CRT (176 ± 27
vs. 150 ± 24 ms after CRT). In contrast, there was no improvement in NYHA class or sRV ejection fraction in those undergoing
de novo CRT implantation. QRS duration in those undergoing
de novo CRT implants increased significantly following CRT. Mortality was high, 21.3%, at a median follow-up of 4.1 years. This suggests that upgrading to CRT is most beneficial in ACHD patients who are already paced and hence at risk of pacemaker-induced cardiomyopathy, but evidence for
de novo CRT in this group is limited [
21]. A recent meta-analysis of 14 observational studies confirmed good response rates to CRT in ACHD (68%,
n = 334) in terms of improvement in ejection fraction or NYHA functional class. Response rates were greater in patients with a systemic left ventricle (80%) compared with those with sRV (58%) and univentricular anatomy (67%) [
17,
22], It is important to note that all studies were small (largest study
n = 80), many included paediatric populations, and the cohort was heterogenous, with different criteria for inclusion and varying definitions of clinical response. Nevertheless, most of the literature suggests that CRT may be a useful adjunct strategy for heart failure management in the ACHD population.
The factors that predict response to CRT in the ACHD population, as in the population without congenital heart disease, are largely unknown, making selection of appropriate patients for CRT difficult. Most recommendations for CRT in ACHD are extrapolated from the non-ACHD population, for example, systemic LVEF < 35%, LBBB and QRS > 150 ms (Class I ESC recommendation) [
23]. There are, however, some ACHD specific criteria; these include recommendations for CRT in those with a sRV EF < 35% and RBBB/QRS > 150 ms (Class IIa), single ventricle anatomy with EF < 35% and QRS > 150 ms regardless of QRS morphology (Class IIa) and in patients with intrinsically narrow QRS if they are undergoing a new device or device replacement with anticipated requirement for significant (>40%) ventricular pacing (Class IIa), although, in clinical practice, this threshold is generally lowered to 20% [
23,
24].
CRT device implantation is technically challenging in patients with distorted coronary sinus anatomy because of congenital heart disease. It may be more difficult to implant the CRT lead at the desired site of the latest activation. Implantation of CRT devices in this complex group should be done at experienced tertiary centres. It should also be considered that most patients undergoing device implantation who have congenital heart disease are often younger than the usual population undergoing CRT encountered in the non-ACHD population. These younger patients will be subject to multiple box changes in their lifetime and the cumulative risk of lead or generator infection and associated sequelae is not insignificant [
25].
There are limitations to applying CRT recommendations from adults without congenital heart disease to the ACHD population. Conduction disease is complex in ACHD, who may have unusual anatomy and multiple previous surgical interventions. For instance, surgically induced RBBB almost certainly differs from native RBBB and the prognosis in this context is unknown. Similarly, the level of recommendation for CRT often depends on baseline QRS duration. Change in QRS duration has shown to be a poor indicator of CRT response in studies of ACHD, with some studies even demonstrating prolongation of QRS duration post-CRT, even in responders [
20,
26]. Pre-procedure imaging with tissue doppler echocardiography and magnetic resonance imaging (MRI) have shown promise in better evaluating mechanical desynchrony in the non-ACHD population and may aid patient selection in the ACHD population where electromechanical association is more complex. The assessment of response to CRT is further confounded by difficulties with echocardiographic assessment of geometry and function, particularly in those with a sRV or univentricular anatomy, and there is likely to be high inter-observer variability even in the hands of the most experienced echocardiographers. Ultimately, larger high-quality studies of CRT in ACHD are needed to develop future ACHD-specific guidelines.
2.4.3. Diastolic Dysfunction
During RV apical pacing, the electrical wave front propagates more slowly and heterogeneously as it is conducted directly via myocardium rather than through the specialised His-Purkinje system, resulting in a left bundle branch block (LBBB) like pattern. Similarly, mechanical activation pattern is also altered, and in animal model studies, RV pacing resulted in diminished rate of change in left ventricular pressure (dP/dt) and impaired shortening in septal to lateral plane [
27]. They concluded that alternations of the normal activation sequence produced by ventricular pacing depress left ventricular pumping function independent of loading conditions, as indicated by a rightward shift of the left ventricular end-systolic pressure-volume relation. The extent of this shift appears to be in proportion to the degree of dyssynchronous activation. The decreased stroke volume during ventricular pacing is due both to a decreased end-diastolic volume (decreased preload) and the rightward shift of the end-systolic pressure-volume relation (decreased pump function).
Over time, this leads to altered coronary perfusion, myocyte disarray and changes in both atrial and ventricular geometry. If this progresses to overt diastolic and/or systolic dysfunction, clinical features consistent with heart failure may be present. However, CRT in the context of diastolic dysfunction is a relatively unexplored area. In one prospective study, 119 patients were followed up for 4 months post CRT implantation. They had non-invasive echocardiographic measures (E/A waves, deceleration time, early diastolic mitral annulus velocity (E′), E/E′ ratio and 2-D speckle tracking strain rate during isovolumetric relaxation) to assess for improvement in diastolic dysfunction. The study found that despite the fact that CRT did not significantly affect the relaxation phase or filling pressures, left ventricular reverse modelling was noted, which resulted in a smaller ventricle with improved filling characteristics. This was corroborated by a further study demonstrating that CRT implantation resulted in no significant change in relaxation properties. In situations where there is anticipation of a high burden of RV pacing and co-existing diastolic dysfunction, CRT may be preferred over conventional pacing to improve LV haemodynamics; however, more studies are needed.
2.4.4. Predicting Response to Therapy
Several key factors influence the likelihood of a positive response to cardiac resynchronisation therapy (CRT), extending beyond QRS duration alone. Electrical predictors play a crucial role, with QRS morphology being one of the strongest determinants of response. Patients with left bundle branch block (LBBB) derive the greatest benefit, while those with right bundle branch block (RBBB) or intraventricular conduction delay (IVCD) tend to experience less improvement. More advanced electrical markers, such as QRS area derived from vectorcardiography (VCG), have demonstrated superior predictive value, with larger QRS areas (>100 µVs) correlating with improved CRT outcomes, even in non-LBBB patients [
28].
Similarly, ultra-high frequency ECG (UHF-ECG) parameters, particularly the e-DYS index, offer a more precise evaluation of ventricular dyssynchrony, helping to identify candidates most likely to benefit from CRT [
29,
30]. Beyond electrical factors, mechanical predictors derived from imaging techniques further refine patient selection. CRT success is significantly influenced by lead placement at the site of the latest LV mechanical activation, as identified through speckle-tracking echocardiography or cardiac MRI [
29]. Additionally, the extent of myocardial fibrosis, as assessed via cardiac MRI, impacts response, with greater scar burden associated with poorer outcomes [
30]. The presence of LV contractile reserve, evaluated through dobutamine stress echocardiography, has also been linked to a higher likelihood of CRT response, suggesting that myocardial viability plays an important role in treatment efficacy.
Haemodynamic and clinical factors further contribute to CRT success. Patients with non-ischaemic cardiomyopathy (NICM) typically exhibit better outcomes than those with ischaemic cardiomyopathy (ICM), likely due to less myocardial scarring and greater contractile reserve [
30]. The presence of moderate functional mitral regurgitation (MR) has also been associated with enhanced CRT efficacy, as improved ventricular synchrony leads to LV reverse remodelling and MR reduction [
31]. In patients with atrial fibrillation (AF), particularly those undergoing AV nodal ablation, CRT is highly beneficial as it ensures a consistently high percentage of effective biventricular pacing, which is critical for achieving optimal outcomes. Finally, device-related factors, particularly LV lead positioning, play a pivotal role in CRT response. Lead placement in a lateral or posterolateral coronary sinus vein is associated with superior resynchronisation, while apical lead positioning, although capable of narrowing QRS duration, may provide suboptimal haemodynamic benefit due to spatial dispersion of depolarisation [
31].
2.4.5. Novel Methods to Assess Electrical Dyssynchrony
Various novel techniques have been developed to assess electrical dyssynchrony, including ECG-imaging (ECGi), body surface potential mapping (BSPM), vectorcardiography (VCG) and ultra-high frequency ECG (UHFECG). QRSd and LBBB form the basis of patient selection for CRT and are proven to predict therapy response [
28,
29]. These features are determined from a 12 lead, surface ECG, which depicts electrical conduction in a single dimension [
30]. Dyssynchrony can, however, be present in the absence of these features, suggesting that 12 lead ECG parameters may not comprise enough detail to appropriately describe dyssynchrony [
31,
32]. Modern techniques can assess electrical dyssynchrony non-invasively with greater resolution than that of the 12 lead ECG. This may allow both a better selection of patients for CRT, but also the ability to optimise lead positioning or device programming.
BSPM utilises multiple body surface electrodes, usually between 50–100 electrodes, to measure epicardial electrical activation. SDAT (standard deviation of activation time) is a measure derived from the recordings. A reduction in SDAT has correlated with a change in LVESV (
p = 0.007) when compared with QRSd alone and has been able to predict acute haemodynamic response [
33,
34]. Although data on prediction of response has been encouraging, a recent randomised controlled trial assessing optimisation of programming with SDAT, compared to conventional programming, failed to demonstrate a significant difference [
35].
ECGi reconstructs epicardial activation maps from 200+ body surface electrodes combined with CT/MRI imaging [
36,
37]. It provides detailed dyssynchrony markers, such as ventricular electrical uncoupling (VEU) and total activation times (LVTAT, RVTAT), which better predict CRT response than QRSd alone [
38,
39]. Despite its potential, the requirement for advanced imaging limits its accessibility [
40].
VCG derives 3D electrical activation loops using orthogonal leads (X, Y, Z), either from a Frank VCG system or a digitally transformed 12-lead ECG [
41,
42]. QRS area, calculated from these loops, predicts CRT response more accurately than QRSd or morphology [
43,
44]. While retrospective data strongly supports its predictive value, real-time clinical application remains limited, primarily because VCG can only be performed using data from an ECG, rather than producing real-time data [
45,
46,
47].
UHFECG utilizes a 14-lead, 5 kHz recording to detect late potentials in the QRS complex [
48]. The e-DYS index (measure of electrical dyssynchrony), representing maximal depolarisation delay, has shown significant predictive value for LV remodelling and CRT response [
49,
50,
51,
52]. The UHFECG technique shows significant potential in both selecting patients for CRT but also optimising the delivery or programming of CRT or CSP. However, the evidence to date is limited to small observational studies. These novel techniques have shown significant potential to better assess and define electrical activation and dyssynchrony [
53]. In small studies, they have all enhanced prediction of CRT response in comparison to QRSd and QRS morphology; however, more work is needed to fully comprehend application and utility in real world practice. It also differentiates pacing strategies, including conduction system pacing (CSP) [
54]. However, current evidence remains observational, warranting further validation.
As CRT continues to evolve, a more individualised approach incorporating electrical, mechanical, haemodynamic, and anatomical factors is essential to maximise treatment response and improve patient outcomes.
2.5. Optimal Device Programming
Maximal benefit from CRT is derived from a high percentage of effective, biventricular pacing [
55,
56]. It is evident that sub-optimal biventricular pacing worsens outcomes and limits response [
57]. Optimal programming includes an appropriate selection of modes, rates (both lower and upper), and effective timing cycles with AV or VV delays [
57,
58]. Sub-optimal programming is a major factor which influences the percentage and quality of biventricular pacing [
59]. Synchronous AV pacing with optimisation of AV and VV delays has been shown to deliver acute haemodynamic benefit [
60,
61,
62]. Modern practice suggests that parameters require careful consideration and patient tailored options, rather than a “one size fits all” approach [
63,
64]. This optimisation of programming has been considered extensively using a variety of techniques. A practical, simplistic approach is key.
A key determinant of CRT response is the location and positioning of the LV lead. Successful CRT depends not only on narrowing the QRS complex but also on ensuring optimal resynchronisation by targeting the site of the latest LV activation. The coronary sinus (CS) tributary vein anatomy plays a pivotal role in determining where the LV lead can be placed, and its selection is crucial for achieving the desired resynchronisation. Studies suggest that placing the LV lead in a posterior or apical vein may result in a more significant QRS narrowing, whereas placement in a lateral vein might not achieve the same effect due to spatial dispersion of depolarisation. Therefore, ECG and QRS narrowing alone should not be used as the sole predictor of CRT response, but rather in combination with lead placement considerations and haemodynamic improvements [
60]
Echocardiography for many years has been considered as the gold standard for optimisation, with support from various observational trials [
62,
65,
66]. This would involve measuring mitral inflow pressures and aortic velocities to fine tune AV and VV delays [
67]. However, more recent data from randomised controlled trials is contradictory [
68,
69,
70]. The 12 lead ECG optimisation techniques have also been posed, targeting a reduction in QRSd, which is indicative of the electrical treatment strategy [
71]. These methods are also yet to yield a significant advantage. A key disadvantage of these clinical optimisation techniques is contemptuous measurement at rest. More recently, device manufacturers have developed dynamic algorithms built into implanted devices. The specificities of the algorithm vary from manufacturer to manufacturer. The algorithms dynamically alter AV and VV timings based on various electrical intracardiac measures.
Smart AV
TM (Boston Scientific, Hong Kong, China) and QuickOpt
TM (Abbott Medical, formerly St. Jude Medical, Hong Kong, China) have not shown a benefit over empirical AV delay programming [
68,
69].
AdaptiveCRT
TM (Medtronic, Dublin, Ireland) and SonR
TM (Microport, formerly Sorin, Hong Kong, China) have demonstrated non-inferiority to echocardiographic optimisation methods. Fusion-based pacing strategies, such as AdaptiveCRT
TM, aim to fuse left ventricular pacing with intrinsic right ventricular activation, which has been associated with improved clinical outcomes, including reduced heart failure hospitalisations and mortality (HR 0.49) [
72].
SyncAV
TM (Abbott Medical, Hong Kong, China) has been linked to reduced HF hospitalisations in a large propensity score-matched study of 3630 patients [
73].
Additional algorithms that dynamically optimise timings to fuse LV pacing with intrinsic RV activation have yielded some benefits. A higher degree of LV synchronised pacing using the AdaptiveCRT
TM (Medtronic) algorithm was associated with superior clinical outcomes, including mortality and hospitalisation, compared to conventional adaptive biventricular pacing (HR 0.49) [
72]. SyncAV
TM (Abbott Medical, formerly St Jude Medical) has also demonstrated a benefit in reducing HF hospitalisations in a propensity score-matched study involving 3630 patients. [
73]. More recently, long-term outcomes of the AdaptiveCRT
TM (Medtronic) algorithm have been examined using a composite of all-cause mortality and HF hospitalisation. However, recent long-term data from AdaptiveCRT
TM trials [
74] have not confirmed a significant benefit over conventional CRT programming, suggesting that not all patients may require routine optimisation. Instead, device-based optimisation may be most beneficial in patients classified as “non-responders” to standard CRT [
75,
76].
2.5.1. Advanced Pacing Strategies
The anatomical positioning of the left ventricular (LV) lead is a crucial determinant of CRT response, extending beyond QRS duration and morphology. While QRS narrowing is often used as a surrogate for effective resynchronisation, lead placement within the coronary venous system significantly impacts CRT efficacy. Optimal lead positioning aims to target the site of the latest mechanical activation, typically in the lateral or posterolateral tributaries of the coronary sinus (CS), as this has been associated with superior left ventricular reverse remodelling and clinical outcomes [
75]. However, placing the LV lead in a posterior or apical vein can also achieve QRS narrowing, albeit without necessarily improving synchrony, due to spatial dispersion of depolarisation, which can limit haemodynamic improvement. Studies have demonstrated that LV lead positioning over areas of myocardial scar, particularly in patients with ischaemic cardiomyopathy, is associated with worse outcomes, whereas placement in viable myocardium improves CRT response. Additionally, apical lead positioning has been linked to poorer haemodynamic response, as it results in longer LV activation times and less effective synchronisation. Advanced imaging modalities, including cardiac MRI and speckle-tracking echocardiography, are increasingly being used to guide lead placement, ensuring alignment with the region of maximal mechanical delay. Future CRT strategies should incorporate patient-specific anatomical and functional mapping to optimise lead positioning and enhance CRT response rates [
75].
Multi-point pacing (MPP), His Bundle pacing (HBP) and left bundle branch area pacing (LBBAP) have furthered CRT’s ability to deliver advanced pacing strategies. MPP enables pacing from multiple LV sites on a quadripolar lead, theoretically improving resynchronisation. Small studies have shown haemodynamic improvements and better long-term outcomes with MPP [
75,
76,
77]. However, larger randomised trials have not replicated these benefits, and concerns remain regarding reduced battery longevity due to increased energy consumption [
78,
79].
HBP and left bundle branch area pacing LBBAP seek to restore physiological ventricular activation via the native His-Purkinje system [
80]. Though HBP emerged as the first interventional option in clinical studies, there have been concerns regarding rise in capture thresholds over short-term follow up requiring re-intervention [
81,
82]. More recently, LBBAP has emerged as an alternative strategy to provide near physiologic CSP, by pacing the left bundle branch network. LBBAP has been shown to be technically more feasible due to a wider target area, which enables greater lead stability and lower capture thresholds compared to HBP [
83]. A recent meta-analysis revealed that LBBAP was superior to HBP when comparing implant success rates and pacing metrics as an initial pacing strategy [
84].
CSP has shown encouraging clinical outcomes, particularly in the MELOS registry- the largest cohort study on LBBAP to date, which enrolled over 1000 patients to assess its safety and efficacy in pacing-dependent and heart failure populations. The study reported a lead implantation success rate of 92% for bradyarrhythmia indications and 82% for heart failure indications, with 70% of cases achieving left bundle fascicular capture, as well as demonstrating significant clinical improvements across domains, including reduced NYHA functional class, increased LVEF and enhanced exercise capacity. LBBAP was also associated with fewer heart failure hospitalisations and lower overall symptom burden, supporting its potential to improve functional status and quality of life [
82,
83,
84]. These findings suggest that LBBAP could be a viable alternative to conventional CRT in suitable candidates, with ongoing trials expected to validate its long-term benefits further. Despite these positive findings, the registry reported an overall complication rate of 11.7% for LBBAP, which included both acute and late complications. The most frequent complications were lead-related issues, such as acute septal perforation (3.7%) and late lead dislodgements (1.5%). Additionally, complications specific to the ventricular transseptal route occurred in 8.3% of patients [
85]. This registry highlighted the safety and feasibility of LBBAP but underscored the need for ongoing refinement to reduce complication rates further. Additionally, LBBAP procedures were associated with longer procedure times and increased radiation exposure compared to conventional CRT, emphasising the need for optimisation in technique and equipment. Further research is required to refine CSP methods, improve patient selection, and compare long-term outcomes with traditional pacing approaches.
Recent studies highlight the need for further research to refine CSP methods and improve patient selection, especially in comparison to traditional pacing techniques. CSP and biventricular pacing (BiVP) have emerged as alternatives to right ventricular pacing (RVP), which is linked to pacing-induced cardiomyopathy [
84,
86]. While BiVP has demonstrated benefits in patients with wider QRS complexes, it presents challenges like phrenic nerve stimulation and complex optimisation. In the Block HF trial, BiVP showed a 45.8% primary composite outcome of death, heart failure hospitalisation, or increased left ventricular end-systolic volume index compared to 55.6% with RVP [
86].
The LEVEL-AT trial established CSP as non-inferior to conventional CRT in heart failure patients with a wide QRS. However, debate remains regarding its role in patients with narrow QRS complexes and reduced ejection fraction [
87]. Although CSP shows promise in improving left ventricular ejection fraction and reducing heart failure hospitalisations, robust evidence from large-scale trials and longer follow-up studies is still needed. Consequently, CSP should not yet be considered first-line therapy in these patient groups until further research supports its long-term efficacy and stability.
2.5.2. Future Directions
The future direction of CRT likely lies in more specific, patient-tailored approaches, including biventricular pacing, CSP, or HBP, in addition to the concepts outlined above. Novel methods are being explored to help stratify the ideal therapy delivery under the Umbridge of optimised patient selection. A treatment algorithm using interventricular conduction delays (IVCD) guided the choice between BiVP and CSP in CRT patients, shifting 25.6% to CSP. This approach resulted in a significant reduction in cardiovascular mortality and heart failure events compared to standard CRT selection (HR: 1.72,
p = 0.013) [
88]. In another study, computational modelling demonstrated that HBP with LV epicardial lear (His optimised CRT)-HOT-CRT (BIVAT-90: 87.6 ± 6.7 ms,
p < 0.05) and LBBB with LV epicardial lead (LBBB-optimised CRT)-LOT-CRT (BIVAT-90: 73.9 ± 7.6 ms,
p < 0.05)
, provided superior electrical synchrony, particularly in cases of severe LV His-Purkinje conduction disease [
89]. However, CSP was ineffective in the presence of septal scar, whereas CRT significantly improved synchrony (BIVAT-90: baseline 119.1 ± 10.8 ms
vs. CRT 85.1 ± 14.9 ms,
p < 0.01) [
89,
90]. In patients with HFrEF and LBBB, using intraoperative interventricular conduction delay (IVCD) assessment to guide the choice between BiVP or CSP, significantly improved CRT response rates. The study group had a higher proportion of CRT responders compared to the control group (echocardiographic response: 92.5%
vs. 69.8%,
p = 0.009; clinical response: 87.5%
vs. 62.8%,
p = 0.014) and showed greater improvements in ejection fraction and ventricular volumes post-implantation [
91].
2.5.3. Other Approaches for Delivering CRT
Endocardial LV pacing and epicardial surgical LV lead placement represent alternative strategies to conventional CRT, particularly in cases where coronary venous anatomy is unsuitable, or CRT response is suboptimal. Endocardial LV pacing, achieved via transseptal or transapical approaches, has been shown to provide more physiological activation by stimulating the Purkinje network directly, leading to improved ventricular synchrony and haemodynamics compared to conventional epicardial CS lead placement and finally offering a lower risk of phrenic nerve stimulation [
92]. It also potentially can allow for pacing anywhere in the LV, thereby not being restricted by CS anatomy [
93]. Studies have also shown endocardial pacing is less arrhythmogenic when compared to epicardial pacing [
94].
The ALTERNATIVE trial demonstrated that endocardial CRT resulted in greater LV reverse remodelling and symptomatic improvement compared to conventional CRT, particularly in patients with failed CS lead placement of suboptimal response to BiVP. However, endocardial pacing poses an increased risk of thromboembolism, necessitating long-term anticoagulation [
95].
The Wireless Stimulation Endocardially for Cardiac Resynchronisation (WiSE-CRT) system (EBR Systems, Sunnyvale, CA, USA) has recently received approval for use in Europe. Unlike conventional cardiac resynchronisation therapy (CRT), which relies on transvenous coronary sinus leads, the WiSE-CRT system utilises a percutaneously implanted endocardial receiver electrode within the left ventricle (LV). This receiver is wirelessly powered by an ultrasound pulse generator (transmitter), which is implanted subcutaneously—typically in the left pectoral region and connected to a pacing generator [
96,
97]. The transmitter emits ultrasound waves, which are then converted into electrical stimulation by the endocardial receiver. This stimulation is synchronised with right ventricular (RV) pacing, achieving near-simultaneous LV and RV endocardial activation (~2–5 ms delay), thereby delivering biventricular pacing [
97].
The SELECT-LV study demonstrated both the feasibility of the WiSE-CRT system and its clinical benefits for patients meeting CRT indications [
96]. Further supporting its efficacy, the SOLVE-CRT trial and a study by Sidhu et al. reported high procedural success rates, with comparable improvements in LV remodelling to conventional CRT [
97,
98]. Notably, recent studies have suggested that WiSE-CRT has the potential to achieve a narrower QRS duration and higher ejection fraction in patients who failed conventional CRT or were classified as CRT non-responders [
99].
A multicentre registry study (WiCS-LV Post Market Surveillance Registry) led by Sieniewicz et al. evaluated 90 patients who underwent WiSE-CRT implantation. Among these, 4 patients (4.4%) experienced acute complications (<24 h post-procedure), 17 patients (18.8%) had intermediate complications (24 h–1 month post-procedure), and 6 patients (6.7%) developed chronic complications (1–6 months post-procedure) [
99]. Notably, three patients died from procedure-related complications, highlighting the risk profile of the WiSE-CRT system. The most common complications were cardiac tamponade and vascular access-related issues. However, the registry also found that 76% of complications occurred within a centre’s first 10 cases, suggesting a learning curve with initial use of this technology. The study concluded that WiSE-CRT is an effective treatment option for high-risk heart failure patients who are ineligible for conventional CRT or have been classified as CRT non-responders. While complication rates remain significant, outcomes improve with operator experience, underscoring the importance of adequate training. Additionally, the observed risk of cardiac tamponade is consistent with other left-sided vascular procedures, such as left atrial appendage occlusion.
Recent advancements in CRT have broadened its therapeutic scope beyond severe heart failure and conduction delays, demonstrating benefits in patients with milder symptoms, atrial fibrillation, and high ventricular pacing burdens. Landmark trials such as MADIT-CRT and APAF-CRT have shown reductions in hospitalisations, improved cardiac remodeling, and enhanced survival. Emerging evidence in congenital heart disease (ACHD) and diastolic dysfunction suggests CRT’s potential in these complex populations, though larger studies are needed. Innovations like ECG-imaging, Body Surface Potential Mapping, and Ultra-High Frequency ECG are refining patient selection and procedural success. Advanced programming algorithms and novel techniques, such as AdaptiveCRTTM and multi-point pacing, are further optimising outcomes. However, approximately 30% of patients still do not respond, highlighting the need for ongoing patient selection and lead placement improvements. Continued research into CRT’s role in diastolic dysfunction, ACHD, and precision technologies will be crucial in expanding its use and achieving better clinical outcomes.
Conceptualisation, N.D., P.A.P.; Writing—original draft preparation, N.S., Z.Z.; Writing—reviewing and editing, H.K., S.T.; Section on Optimal device programming, J.W.; Visualisation and editing, T.N.
Not applicable.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
 Nihit Shah
2
Zafraan Zathar
3
Sophie Thompson
1
Jamie Walton
1
Harkaran Kalkat
1
Taaru Narayanan
1
Peysh A. Patel
1
Nihit Shah
2
Zafraan Zathar
3
Sophie Thompson
1
Jamie Walton
1
Harkaran Kalkat
1
Taaru Narayanan
1
Peysh A. Patel
1