1. Introduction
1.1. Brief Overview of Fibrosis
Fibrosis is a pathological process characterized by the aberrant accumulation of collagen-enriched extracellular matrix (ECM) components within tissues [
1] and represents a significant challenge in the management of chronic diseases [
2]. This condition can arise as a consequence of chronic inflammation [
3], tissue injury [
4], or tumor development [
5]. Fibrosis affects a broad range of organs, including the kidneys, liver, lungs, heart, and skin, ultimately leading to progressive tissue and organ dysfunction and significantly compromising the patient’s quality of life [
6]. In severe cases, fibrosis can culminate in life-threatening complications or mortality [
7]. In many tissues (with the skin being an exception, as discussed later), fibrosis accumulation is an intrinsic aspect of aging, driven by repeated episodes of cellular and tissue degeneration. Aging and age-associated fibrosis are detrimental to tissue regeneration and are suppressed in animal models of enhanced longevity [
8,
9]. Consequently, the development of strategies for timely intervention is paramount in halting the progression of fibrosis, mitigating its deleterious consequences, and realizing the reversal of the fibrotic tissue microenvironment to facilitate the regeneration of healthy, functional tissues [
10].
1.2. Fibroblasts and Myofibroblasts
Fibroblasts are mesenchymal cells resident to connective tissues and play pivotal roles in maintaining tissue equilibrium, facilitating repair, and modulating disease processes. They are known for their capacity to synthesize and regulate the ECM, which offers crucial structural support to tissues and organs [
11]. Beyond ECM production, fibroblasts function as signaling hubs by releasing cytokines, growth factors, and other signaling molecules that influence neighboring cell behavior and tissue development [
12,
13]. They also exert mechanical forces through contractility, which has importance in processes such as wound healing and tissue remodeling [
14]. Moreover, fibroblasts regulate tissue metabolism, interact with metabolic pathways, and possess plasticity to differentiate into various mesenchymal cell types, contributing to tissue regeneration [
15]. They are vital in establishing and maintaining specialized niches within tissues, providing essential support for tissue-resident stem cells. Additionally, their secretion of positional cues helps guide cellular behavior and organize tissue structure [
16].
Myofibroblasts are specialized cells crucial for tissue repair but implicated in fibrosis. These cells exhibit key characteristics such as abundant extracellular matrix (ECM) and growth factor production whilst possessing α-smooth muscle actin (α-SMA)
+ cytoskeletal stress fibers, granting them superior contractile capabilities compared to fibroblasts and more akin to the contractility of smooth muscle cells. Increased production of collagen type I, hyaluronic acid synthase 2 (HAS2)-synthesized hyaluronan (HA), fibronectin, and the extra domain A variant of fibronectin (EDA-FN) are typical hallmarks of myofibroblast-synthesized matrices. Myofibroblasts play significant roles in wound healing by depositing a collagen-rich ECM, restoring mechanical strength to the tissue defect site and assisting in wound closure. However, their persistence in tissues is the central effector in driving organ fibrosis, wherein the accumulation of fibrous ECM extends beyond normal repair mechanisms [
17].
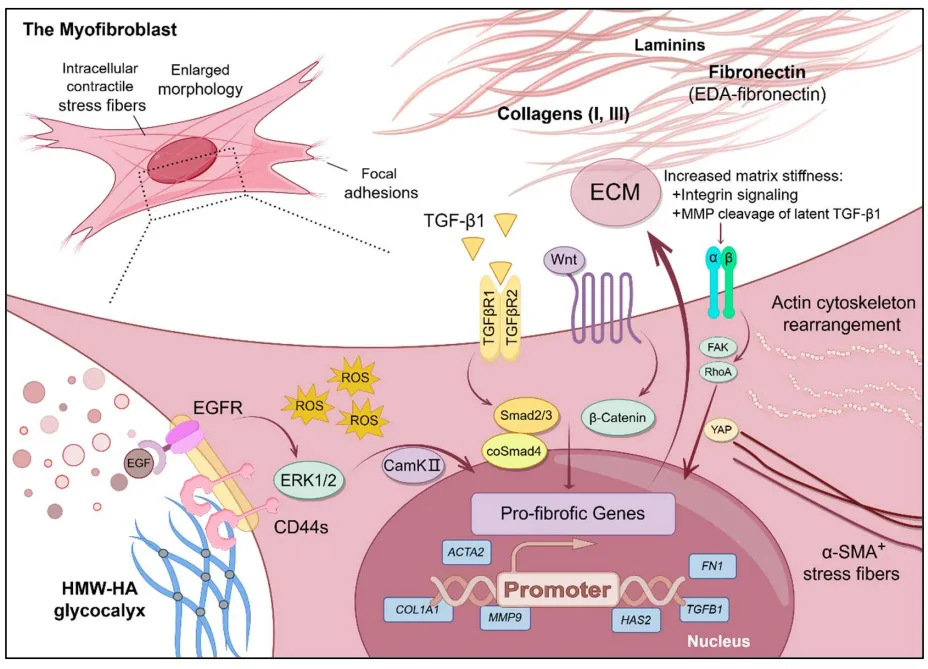
The transformation of fibroblasts into myofibroblasts is regulated by a complex network of signaling pathways. For instance, the canonical transforming growth factor-β (TGF-β)/Smad pathway is involved in stimulating ECM synthesis and inhibiting its degradation [
18]. In contrast, the non-canonical Wnt and epidermal growth factor receptor (EGFR)/CD44 pathways influence cell proliferation, differentiation, and migration [
19,
20]. Moreover, G protein-coupled receptor (GPCR) signaling, particularly in response to molecules like angiotensin II and endothelin-1, triggers proliferation, myofibroblast transdifferentiation, collagen synthesis, and cytoskeleton rearrangement enhancing cellular contractile ability [
21]. Additionally, mechanosensitive integrin and Ca
2+-dependent signaling pathways respond to changes in ECM stiffness and tension, crucially impacting focal adhesion kinase (FAK)/RhoA signaling, Yes-Associated Protein (YAP)/Engrailed-1 activity, cell activation, upregulated enzymatic cleavage of latent TGF-β1, and myofibroblast differentiation [
22]. This intricate interplay between signal transduction, mechanical forces, and cellular responses underscores the complexity of pro-fibrotic cell processes. It highlights the multifaceted nature of myofibroblast functions in tissue homeostasis and pathology ().
Figure 1. The myofibroblast phenotype is characterized by an enlarged morphology and the presence of intracellular contractile stress fibers and focal adhesion sites, the myofibroblast is the predominant scar-forming cell phenotype. Myofibroblast differentiation can be activated through different, but often intersecting, signaling pathways, including: the canonical TGF-β1/TGFBR/Smad2/3 pathway; the Wnt/β-catenin pathway; integrin mechanotransduction pathways involving FAK/RhoA and YAP/Engrailed-1; the HA-CD44/EGFR/ERK1/2/CamKII pathway; and dysregulated antioxidant pathways. The upregulation of profibrotic genes, ECM, and reorganization of the intracellular actin cytoskeleton to incorporate α-SMA<sup>+</sup> are hallmarks of fibroblast-to-myofibroblast differentiation.
Inflammation is an important step in the pathological occurrence of myofibroblasts and tissue fibrosis. For an overview of the roles that leukocytes, immunology, and inflammatory processes play in the promotion of fibrosis, we refer readers to a recent review that covers the subject matter in extensive detail [
23]. The cycle of inflammation and fibrosis may be, in part, provoked by an imbalance of intracellular oxidative stress regulators, leading to the activation of anti-apoptotic pathways, induction of inflammatory and fibrotic gene expression, and the overproduction of reactive oxygen species (ROS) [
24].
1.3. Other Sources of Pro-Fibrotic Cell Phenotypes
Whilst commonly differentiating from tissue-resident fibroblasts, myofibroblasts can emerge from a diversity of cell phenotypes in response to tissue injury and pathological inflammatory triggers. Identified cell phenotypes that may serve as myofibroblast precursor cells include epithelial, endothelial, other mesenchymal cells, circulating progenitor cells, and leukocytes. In this section, we briefly describe the types of cells contributing to myofibroblast tissue populations that continue to be the focus of recent research: epithelial cells, endothelial cells, and macrophages.
1.3.1. Epithelial-Mesenchymal Transition (EMT)
EMT denotes a biological phenomenon wherein epithelial cells relinquish their epithelial characteristics to adopt mesenchymal traits, undergoing a transformative process into fibroblast-like and myofibroblast-like cell phenotypes. Whilst EMT has been identified to serve important roles during tissue development [
25], in some tissues, EMT has emerged as a contributor to the pathogenesis of tissue fibrosis. For instance, epithelial cells undergo EMT processes during renal fibrosis [
26] and pulmonary fibrosis [
27]. Continuing to develop our understanding of the intricate molecular mechanisms governing EMT within the fibrotic milieu is important for devising targeted therapeutic interventions to mitigate fibrotic diseases, wherein EMT is a predominant process [
28,
29]. Early reports suggested that keratinocytes undergo EMT to migrate across the wound bed during dermal healing [
30]. Still, there has been a lack of recent studies on this phenomenon and the extent of its contribution to dermal scarring.
1.3.2. Endothelial to Mesenchymal Transition (EndMT)
EndMT constitutes a multifaceted process where endothelial cells acquire traits typical of fibroblast-like and myofibroblast-like cells. This transformation involves the loss of endothelial features and the adoption of mesenchymal characteristics, including altered morphology, loss of cell-cell junctions, heightened mobility, invasiveness, and contractility, accompanied by the expression of mesenchymal-specific proteins such as α-SMA, N-cadherin, vimentin, and fibronectin. Whilst partial EndMT plays a role in angiogenesis [
31], during fibrotic conditions, EndMT emerges as a significant player in the pathogenesis of various organ fibrotic diseases, such as those affecting the lungs, liver, heart, and kidneys. For instance, in cardiac and liver fibrosis, EndMT can be driven by the overactivation of the TGF-β1 signaling pathway in valve and sinusoidal endothelial cells, respectively. EndMT has been shown to promote the accumulation of fibroblasts within these tissues, leading to excessive ECM deposition and tissue restructuring [
32]. In the skin, it was recently reported that Sox9
+ endovascular progenitor cells undergo EndMT to contribute to dermal scarring [
33]. Understanding the distinction between mechanisms underlying resident fibroblast differentiation and EndMT may help to devise targeted therapeutic interventions to combat fibrotic diseases in the stages wherein EndMT is a substantial contributor to fibroblast populations.
1.3.3. Macrophage-to-Myofibroblast Transition (MMT)
MMT denotes a process wherein macrophages undergo transformation into myofibroblasts upon exposure to inflammatory stimuli, characterized by the simultaneous expression of macrophage markers such as CD68 and myofibroblast markers such as α-SMA. For example, in renal fibrosis, Inflammatory macrophages undergo MMT, which emerges as a pivotal contributor to fibrosis development by fostering collagen production and facilitating the formation of fibrotic tissue [
34]. Importantly, reports indicated that a substantial proportion of myofibroblasts observed in the exacerbation of renal fibrosis, including in unilateral ureteral obstruction (UUO) and renal allograft models, originated from the recruitment of circulating leukocytes,
i.e., bone marrow-derived macrophages [
35]. MMT as a source of myofibroblasts is a relatively recent discovery (MMT was coined in 2014), and there is limited information available in the literature on its role in contributing to dermal fibrosis. Nonetheless, MMT augments the intricacies of fibrotic processes, offering valuable insights into potential immunoregulatory therapeutic avenues for managing the development of progressive fibrosis.
2. Dermal Fibrosis
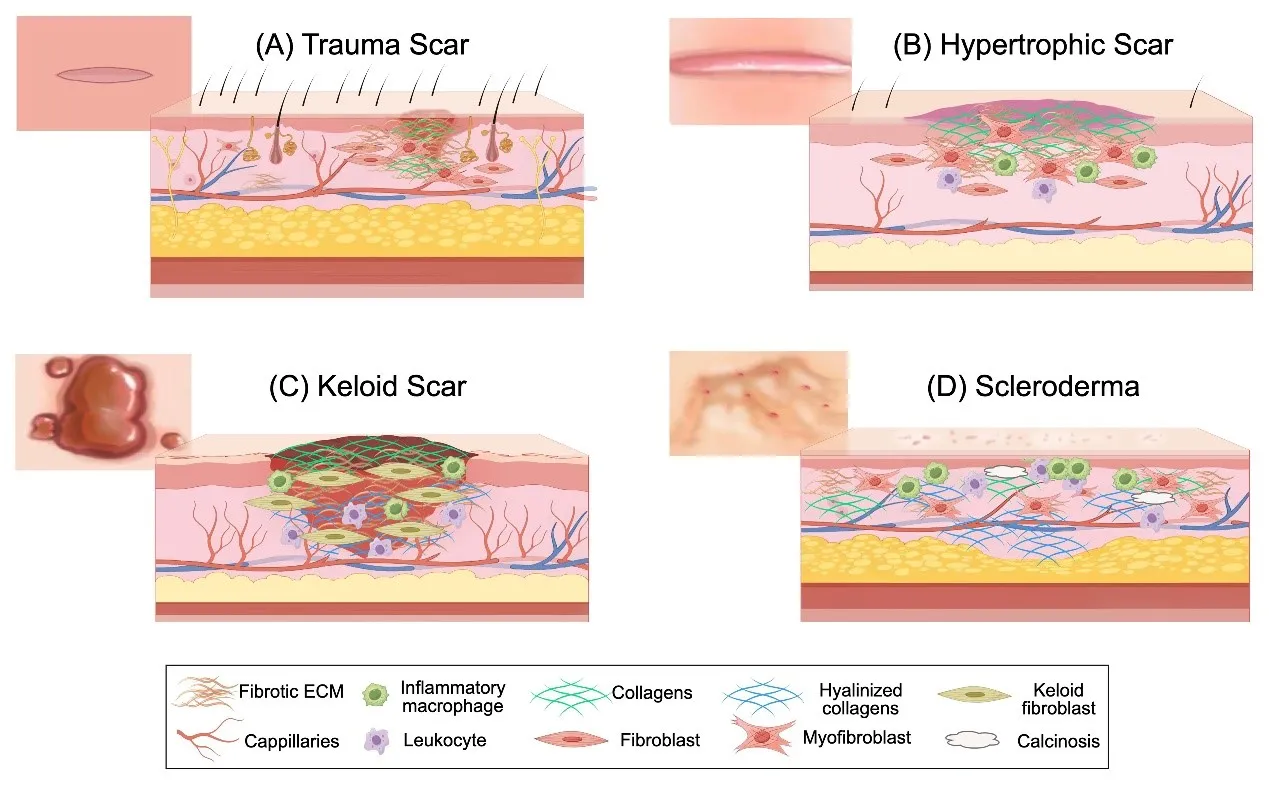
As the largest organ of the human body, the skin is in direct contact with the external environment. It has functions such as sensing external stimuli to regulate homeostasis and as a barrier against pathogens. Dermal wound healing has been extensively studied and occupies the majority of the literature on healing research. Scarring can be seen as an emergency healing response, where the wound is rapidly closed, and the skin's barrier function is restored. However, this process often results in a disorganized imbalance of matrix components and the loss of skin appendages (A). However, failure in the timely resolution of myofibroblast populations through apoptosis results in their prolonged presence in the tissue, which promotes excessive deposition of ECM, thereby exacerbating the pro-fibrotic tissue microenvironment through a positive feedback loop and resulting in aberrant scar tissue formation [
19,
36]. This process is central to the development of dermal fibrosis (or cicatrix) with complex etiologies, such as hypertrophic scarring, keloid scars, and chronic inflammation-induced scleroderma. The significant impact of dermal fibrosis on human health, both psychologically and physiologically, highlights the urgent need for further research to develop effective interventional strategies.
. (<b>A</b>) A typical scar presents as flat and smooth with a pink hue that pales over time. The scar is formed by elevated collagen production by activated fibroblasts and myofibroblasts. (<b>B</b>) Hypertrophic scars present as raised scars. During formation, these scars are enriched in collagens, driven by myofibroblasts under prolonged activation by inflammatory cells. Auxiliary skin structures, nerve endings, and capillaries may be lost due to their replacement by the collagen scar. (<b>C</b>) Keloid scars are produced by hyperproliferative and overactivated keloid fibroblasts that produce a scar resembling a tumor with a darkened hue. An abundance of capillaries, leukocytes, macrophages, and hyalinized collagen bundles surround the keloid scar. (<b>D</b>) In scleroderma, capillary rarefaction is accompanied by capillary enlargement and leakage, presenting red blemishes on the skin surface. Myofibroblasts, under chronic activation by leukocytes, produce excessive collagen and hyalinized collagen bundles that penetrate the intradermal fat layer. In some cases, calcinosis may occur in scleroderma plaques and lesions.
Hypertrophic scars are pronounced or raised scar tissue, significantly higher than the surrounding normal skin tissue, but still have the original wound shape (B). This type of scar tends to occur in high-tension areas such as at joints, on the chest, and in proximity to the shoulders [
37]. Hypertrophic scars are commonly caused by full thickness trauma, such as burns. However, unlike atrophic scars that have healed to leave a concave depression in the skin, hypertrophic scars arise from the overactivation of fibroblasts and myofibroblast differentiation as a consequence of prolonged inflammation at the deep reticular dermis layer [
38]. Autologous skin transplants using full-thickness or split-thickness skin grafts are often used to treat burn injuries but have varying degrees of success due to complications arising from early skin graft contracture during healing and the formation of hypertrophic scarring [
39]. Histological analysis of hypertrophic scars reveals the raised scar contains an abundance of α-SMA
+ myofibroblasts, elongated and thickened bundles of collagens that appear stretched in parallel to the surface of the epidermis, reduced numbers of capillaries, and an absence of auxiliary skin structures such as hair follicles, nerve endings, sweat glands, and sebaceous glands [
40,
41]. In addition, glycosaminoglycan deposits and clusters of inflammatory cells can be observed in the reticular dermis. The prevention of hypertrophic scars relies on intervention during wound healing, such as conservative treatment schemes using gel patches and compression dressings. Reversal of established hypertrophic scarring is more difficult to achieve, with current clinical options limited to multiple treatments such as scar resection surgery, radiation therapy, or laser therapy [
42].
2.2. Keloid Scars
A keloid is a tumor-like scar that is significantly raised compared to the surrounding tissue and extends beyond the border of the original wound site (C). Keloid scars appear to be unique to humans, making them a difficult pathology to mimic in pre-clinical studies. Keloids are characterized by rapid growth and high recurrence rates following resection. They tend to develop in areas frequently subjected to tension, such as the chest and shoulders, as well as in softer tissue regions like the earlobes and cheeks [
43]. The formation of keloids has been associated with chronic inflammation, and the immune system is believed to play a crucial role in the formation process. Keloid scars are genetically driven, appearing more commonly in Africans (5%–10% of the population) and less so in Asians (0.1%–1% of the population) [
37]. Although low in cellularity due to ECM abundance, keloid tissue contains elevated numbers of leukocytes, increased numbers of capillaries, and unique subpopulations of pathological fibroblasts, known as keloid fibroblasts. These cells are morphologically distinct from myofibroblasts and highly migratory. Keloid fibroblasts also synthesise excessive ECM but deposit thick and uniform hyalinized collagen type I and III bundles [
44]. The treatment methods for keloids depend on their quantity and size. The appearance of multiple or larger keloids in different parts of the body may indicate underlying genetic factors or the influence of systemic diseases, which should be carefully considered. Due to the continuous re-activation of the cycle of pro-inflammatory and pro-fibrotic cell processes, resection may aggravate keloid growth. Thus, multiple treatments are usually adopted.
2.3. Scleroderma
Dermal fibrosis can manifest as a consequence of chronic autoimmune skin diseases, such as psoriasis, vitiligo, and atopic dermatitis [
45]. Systemic sclerosis (SSc) is an autoimmune disease characterized by vascular lesions and progressive fibrosis of the skin (scleroderma) and internal organs. An ischemia-reperfusion type response, oxidative stress, vascular pathologies (rarefaction, endothelial cell activation, capillary enlargement, and capillary dilatation near the epidermis), abnormal perivascular infiltration of immune cells, and fibrinolysis contribute to scleroderma pathogenesis, with the transformation of fibroblasts into myofibroblasts and changes to the microstructure of ECM in the dermis driving fibrosis (D) [
46,
47,
48]. The thickening of the skin at scleroderma sites can lead to lesions and the loss of auxiliary skin structures and their peri-glandular adipose tissue. Biochemical and histological analysis of scleroderma lesions reveals that collagen type I and III abundance in the expanded fibrotic dermis is similar to that of normal tissues. However, there is an atypical presence of hyalinized tissue, densely crosslinked collagen, and type VII collagen. Collagen accumulation in the reticular dermis leads to the loss and replacement of sub-adjacent adipose tissue with more collagen. Calcinosis cutis (cutaneous calcium deposits) may occur at lesion sites. The incidence and clinical manifestations of scleroderma are geographically and pathologically heterogeneous, respectively. The population prevalence in Europe and America is much higher than in Asia. Although the incidence rate is relatively low, the mortality rate of SSc ranks first among rheumatic diseases [
49]. At present, the treatment of scleroderma mainly focuses on mitigating inflammation, immunosuppression, and pain management [
50].
2.4. Other Fibrosis-Associated Skin Pathologies
Dermatofibrosarcoma protuberans (DFSP) is a rare malignant fibrous tissue cell tumor that can undergo invasive growth. Due to similarities in histology, DFSP may be misdiagnosed as fibrosarcoma or keloid scars, leading to poor treatment effectiveness and high recurrence rates [
50]. The small tumors contain large numbers of flattened fused fibroblasts that exhibit a spiral-like arrangement. These cell formations lack nuclei and exhibit a characteristic honeycomb pattern that infiltrates the subcutaneous fat, leading to the loss of adipose tissue [
51]. DFSP is resistant to chemotherapy and radiation therapy, and surgical resection is currently the preferred treatment option [
52].
Desmoplastic malignant melanoma is associated with excessive exposure to sunlight. Under the microscope, tumors appear to be of varying sizes with unclear boundaries [
53]. Desmoplastic malignant melanoma mainly contains spindle-shaped melanocytes without melanin that infiltrate the collagen-enriched ECM. The pro-fibrotic tissue microenvironment promotes immune cell infiltration, creating challenges for achieving effective drug delivery [
54]. Current clinical treatment options are surgical resection, radiation therapy, and systemic immunotherapy [
55].
Graft versus host disease (GVHD) is the most common life-threatening complication of allogeneic hematopoietic cell transplantation. Clinically, it is divided into acute and chronic GVHD [
56]. Skin damage is an early clinical manifestation of GVHD (known as cutaneous GVHD) [
57]. Whilst commonly first presenting as a rash [
58], the damage to the underlying dermis by chronic inflammation results in the buildup of fibrotic tissue. At present, treatment of GVHD relies on topical anti-inflammatories and immunosuppressants [
59].
2.5. Age-Associated Fibrosis and Reduced Healing in the Aged Dermis
Notably, the skin differs from many other tissues in that advanced age does not result in the progressive accumulation of fibrotic tissue typically observed in the aging of other organs. In tissues such as the lungs and kidneys, aging has been associated with an impaired capacity to resolve fibrosis, partly due to the increased presence of apoptosis-resistant myofibroblast-like senescent cells. Skin aging leads to slower healing rates and reduced scar formation by dermal fibroblasts. This phenomenon is driven by shared cellular abnormalities observed in other tissues, wherein senescent cells release senescence-associated secretory phenotype (SASP) factors, driving chronic inflammation in a process known as inflammaging. However, in the skin, senescent dermal fibroblasts have diminished expression of a HA glycocalyx, reductions in EGFR cell surface presentation, resist TGF-β1 driven differentiation to myofibroblasts, and have reduced migratory and proliferative capabilities, resulting in reduced scarring or thinner scars [
60,
61,
62]. Thus, dermal fibroblast senescence has a stronger association with chronic non-healing wounds than dermal fibrosis. Although the precise mechanisms remain unclear, it has been suggested that age-associated loss of keratinocyte-secreted stromal-derived factor 1 (SDF1) plays a role in age-associated lack of scarring in the skin [
63]. Nevertheless, replicating the loss of myofibroblast differentiation observed in aged skin could serve as a promising strategy to inhibit myofibroblast formation and reduce dermal fibrosis.
3. Hydrogels
After over a century of advancements, hydrogels have emerged as a pivotal therapeutic approach in the field of biomedical materials and tissue engineering. Hydrogels are created through covalent and/or non-covalent cross-linking of polymeric materials, leading to the formation of complex three-dimensional (3D) network structures [
64,
65,
66]. Hydrogels typically exhibit high water absorption capabilities, excellent biocompatibility, flexibility, adhesiveness, and porosity. Due to their ability to retain moisture at wound sites, hydrogels are an appealing option for wound dressing applications. Furthermore, they can be tailored specifically to optimize their environmental responsiveness (to factors such as temperature, pH, and light) [
67,
68,
69,
70,
71,
72,
73]. Controlled release of incorporated bioactive substances and nanomaterials from hydrogels is an effective means to achieve a prolonged treatment effect, ideal for maintaining an anti-inflammatory, antibacterial, and antifibrotic wound site during healing [
74,
75,
76,
77], thereby having the potential to realize attenuated scar formation. For example, Chen et al. disrupted mechanotransduction signaling in activated fibroblasts and myofibroblasts to mitigate hypertrophic scarring in split-thickness skin graft-treated wounds. By loading 1 mg small-molecule FAK inhibitor VS-6062 into a pullulan hydrogel patch that covered the skin grafts, early graft contracture was avoided, and the activation of wound site fibroblasts was attenuated (>75% released within 24 h, 100% released by 96 h) [
78].
Hydrogels are made from both natural and synthetic materials. Natural polymers such as hyaluronic acid (HA), gelatin (Gel), alginate, and chitosan (CS) are commonly used, along with synthetic polymers like polyvinyl alcohol (PVA) and polyethylene glycol (PEG) [
79,
80,
81,
82,
83,
84,
85,
86,
87]. The choice of polymer or polymer blend depends on the desired outcome. Natural polymers typically provide bioactivity, while synthetic polymers contribute structural stability. The wide range of available polymers and advancements in hydrogel fabrication techniques have expanded their applications beyond topical wound dressings. Additionally, many polymer backbones can be easily modified to include cross-linkable side groups, such as thiol/sulfhydryl or photoinducible methacrylate (MA). These modifications provide a straightforward way to improve gelation and enhance structural properties. Owing to bioactive and biomimetic properties resembling ECM, polymeric hydrogels may function as effective cell carrier materials that are also suitable for culturing organoids and specialized cell phenotypes. Additionally, hydrogel materials have a wide range of applications (), including scaffold coatings, bioinks, biosensors, and more [
68,
88,
89,
90,
91,
92]. More recently, hydrogels have been utilized as sensors for physiological monitoring, further expanding their range of applications [
93,
94,
95,
96]. In the following sections of this review, we discuss recent advancements in hydrogel fabrication techniques and their applications in attenuating dermal scars. We classify hydrogels according to their construction principles. First, we summarize recent injectable hydrogels, then lyophilized hydrogel dressings/cryo-gels, spray-on/sprayable hydrogels, 3D printed hydrogels, and hydrogel-based microneedle patches.
. The versatility of hydrogel components facilitates their fabrication through multiple techniques, including the topically applied wound dressing style hydrogels (adhesive patches, cryo-gels, and spray-on/paste-on hydrogels); injectable hydrogels for <i>in situ</i> gelation and formation of subcutaneous bioactives reservoirs; anisotropic hydrogels that change shape or elicit functions dependent on stimuli responses; core-shell hybrid materials realizing mechanical support and granting inert polymers bioactivity through coatings; 3D printed hierarchical and cell-laden hydrogels to achieve complexity in design and the formation of microtissues; and microneedle patches that facilitate transdermal/subdermal delivery of bioactives when epidermal penetration is a pre-requisite for the intended function.
Subcutaneous injection of hydrogels aims to achieve gelation
in situ, forming a hydrogel network that regulates the surrounding tissue microenvironment and provides a reservoir for the controlled release of bioactive. Injectability enables therapeutic reach to deep tissues, and adhesive properties allow the filling of irregular wound spaces without the need for sutures, which traditional sheet-like hydrogels may struggle to achieve. Injectable hydrogels greatly reduce the need for invasive surgeries. Injectability requires certain key characteristics, such as self-healing and shear-thinning properties [
97]. A variety of chemical and physical crosslinking techniques have been employed to create injectable hydrogels that gel under certain conditions. Crosslinking between the polymers can be induced by physical stimuli through noncovalent interactions like hydrophobic and ionic bonds. Chemical crosslinking of polymers is achieved through covalent bonds formed via coupling processes such as photoirradiation, Schiff base crosslinking, Michael-type addition, thiol exchange/disulfide crosslinking, and click chemistry. In most applications, injectable hydrogels are initially prepared in the solution state and eventually transition into the semi-solid gel state upon injection into the host due to external stimuli, of which a popularized stimulus is fast gelation at body temperature (>37 °C). After mixing or crosslinking of injectable hydrogel components, based on their unique shear thinning and self-healing properties, the generation of high strain through high shear force during extrusion from the syringe temporarily fluidizes the hydrogel before it returns to a gel state again within a short time after injection [
98,
99,
100].
Selection of pre-gelling components is necessary to achieve the injectability of hydrogels with wet tissue adhesiveness, rapid gelling, and the capacity to achieve timely hemostasis. For example, Zhao et al. prepared injectable hydrogel adhesives by combining poly(citric acid-
co-polyethylene glycol)-
g-dopamine prepolymers and aminocapsule-terminated Pluronic F127 micelles loaded with astragaloside IV (<30% released within 24 h; sustained release reached 80% within 300 h). The researchers used an H₂O₂/horseradish peroxidase system to cross-link catechol groups in polydopamine (PDA)/dopamine (DA) via oxidative coupling. This system also facilitated the chemical crosslinking of catechol to the micelle amino groups. In a methicillin-resistant
Staphylococcus aureus (MRSA)-infected mouse model of full-thickness skin defects, the treatment group showed less inflammatory cell infiltration, a relatively mild inflammatory response, with low levels of TNF-α and high levels of IL-10. The regeneration of skin tissue by the injected hydrogel adhesives exhibited dense collagen I/III deposition with optimal directional alignment and timely revascularization of the wound site, thereby achieving scar-reduced wound repair. Notably, hydrogels containing astragaloside IV accelerated healing with minimal scarring, while also promoting the regeneration of functional skin appendages [
101]. In another study, Zhang et al. used an innovative approach wherein the imine-based photo-induced crosslinking of injectable hydrogels could be realized as a delayed or pulsatile drug release platform. HA/
o-nitrobenzene and HA/carbohydrazide were used as the pre-gelling polymers to deliver
o-nitrobenzene modified poly(lactic-co-glycolic) acid (PLGA) capsules loaded with 0.01%
w/
w TGF-β inhibitors. In a mouse model of full-thickness skin defect, wounds showed accelerated closure and the delayed release of TGF-β inhibitor from PLGA capsules (none released <6–8 days, 100% released <8–10 days depending on molecular weight). The result was significantly reduced collagen deposition, decreased inflammation levels, and inhibited tissue fibrosis, compared to a non-pulsatile HA hydrogel control. The team went on to demonstrate attenuated scar formation in a rabbit ear full-thickness wound model and a porcine full-thickness excision wound model [
102].
The inherent advantage of hydrogels is their capacity to serve as cytocompatible carrier materials. Zhang et al. prepared injectable microgels composed of aligned silk nanofibers that enhanced the paracrine secretion of beneficial factors from the loaded bone-marrow mesenchymal stromal cells (BMSCs; 4 × 10
6 cells/mL) to influence the surrounding tissue microenvironment. Scarless healing with accelerated hair follicle recovery was successfully achieved in a rat excisional wound model. Treatment promoted angiogenesis and regulated the inflammatory response to facilitate skin regeneration [
103]. A potential weakness of injectable hydrogels is their potentially rapid degradation
in vivo, accompanied by fast release of payloads. To address this issue, Griffin et al. prepared microporous annealed particle (MAP) microgel scaffolds composed of crosslinked L- and D-peptides to study the influence of chirality on material degradation. In murine wound models, there were no differences in wound closure time between mixed L/D-MAP, but MAP doped with D-chiral peptides showed anti-degradation properties. Interestingly, D-MAP promoted the formation of hair follicles and enhanced tissue tensile strength, akin to embryonic-like tissue regeneration. Furthermore, D-MAP was shown to trigger antigen-specific responses while enhancing bone marrow cell recruitment through adaptive humoral immunity, a mechanism that induced skin regeneration depends on [
65].
Endowing polymers with bioadhesion, such as by modification with PDA, remains a popular strategy to achieve hydrogel crosslinking and rapidly form stress-resistant wound seals. Deng et al. designed an injectable multifunctional hydrogel loaded with therapeutic PDA nanoparticles encapsulating 0.182 ± 0.043%
w/
w asiaticoside. By using dynamic Schiff base crosslinking between oxidized dextran and quaternary ammonium chitosan, reinforced by crosslinking between DA-modified oxidized dextran and DA-modified reduced graphene oxide, the researchers engineered a multifunctional hydrogel that exhibited tissue adhesion, self-healing, antibacterial and antioxidant properties. Furthermore, electrical conductivity granted by the incorporated graphene oxide promoted cell migration and proliferation. In a rat full-thickness skin defect model, the developed hydrogel effectively blocked fibrosis while stimulating collagen synthesis, and this antifibrotic effect was further enhanced by asiaticoside mitigation of myofibroblast activity. The combination of reduced oxidative stress, accelerated cell proliferation and neoangiogensis, and reduced inflammation, promoted scarless skin tissue with skin appendages [
104].
3.2. Cryo-Gels
Cryogels, formed by repeated freezing and thawing of polymer solutions or hydrogels, address the need for sponge-like polymer scaffolds with adjustable pore sizes and tailored porosity [
105]. Additionally, based on the appropriate selection of polymer base material, cryo-gels can have excellent compressibility, elasticity, and swelling, thereby meeting ideal properties for wound dressing materials [
106]. Liu et al. constructed a double network cryo-gel consisting of PVA and agarose loaded with 1%
w/
w hyperbranched polylysine and 0.8%
w/
w tannic acid, in which PVA formed a primary physical crosslinking network after repeated freezing and thawing, and agarose formed a secondary physical crosslinking network through hydrogen bonding. In a rabbit ear MRSA-infected wound repair model, the released components from cryo-gels (~50% hyperbranched polylysine within 24 h, total release <70%; ~30% tannic acid within 24 h, total release <50%) significantly reduced local tissue inflammation, reduced collagen deposition, modulated collagen type I:III ratios, down-regulated α-SMA production, and decreased scar thickness [
107]. Following their design of an antifibrotic peptide that competes with integrins to bind EDA-fibronectin and prevent mechanotransduction signaling [
108], Zhang et al. synthesized genipin-crosslinked hydrogel networks consisting of carboxymethyl CS, poly-γ-glutamic acid, and the antifibrotic peptide (~20 μg loaded per dressing). Lyophilization of the hydrogel resulted in a porous dressing biomaterial that exhibited ideal wound dressing properties such as hemostasis, antibacterial activity, and wound exudate absorption. Swelling and subsequent degradation of cryo-gel dressings achieved the controlled release of the antifibrotic peptide (~40% within 8 h; after which the release rate matched the dressing degradation rate) to mitigate hypertrophic scar formation and promote the regeneration of auxiliary skin structures in a rabbit ear model of full-thickness skin defects [
109]. Notably, the hydrogel components selected for their wound-healing properties also demonstrated a mild antifibrotic effect by disrupting integrin signaling. This effect was further enhanced by the synergistic inhibitory actions of the released peptide. Fan et al. constructed a hybrid fibrous scaffold with vertically aligned Gel-MA cryo-gel fibers and randomly aligned fibroin fibers, to which 1%
w/
w anti-inflammatory peptide 1 (AP-1) was coupled. In a mouse back wound model, the treated group had a reduced inflammatory state and epidermal thickness, whereas collagen composition and densities were similar to normal skin. Additionally, a higher number of regenerated hair follicles were present in the treatment groups [
110]. The base material of Gel-MA with fibroin also demonstrated an antifibrotic effect, offering potential routes of investigation into optimizing antifibrotic effects based on material design. fibers Ying et al. prepared a multifunctional aloin-arginine-alginate cryo-gel that transforms back into a hydrogel upon absorbance of wound exudate or blood for cutaneous regeneration. In a mouse model of
S. aureus infected dorsal wounds, the cryogel treatment group demonstrated antibacterial and anti-inflammatory properties, accelerated wound healing by promoting angiogenesis, and achieved scar-attenuated healing with evidence of skin appendage regeneration [
111].
3.3. Spray-on/Paste-on Hydrogels
Spray-on and paste-on hydrogels represent an innovative advancement, offering ease of use for treating wounds in challenging or hard-to-reach locations. Chen et al. constructed HA-modified and verteporfin (VP)-loaded polylactide nanogels (2 µg/mL VP per 4 mg/mL polylactide) to promote scarless wound healing after paste-on application to the wound site. The nanogel release of HA and lactic acid (within first 6 h) accelerated wound re-epithelialization, and the released VP (~28.3% within 12 h) inhibited YAP to suppress myofibroblast driven fibrosis without hindering the proliferation and migration potential of skin fibroblasts, which ultimately limited scar formation in a rabbit ear injury model [
112]. Spray-on hydrogels can be applied by syringe and/or jet devices to rapidly form
in situ protective layers on irregular and large deformation of wounds [
113]. Sprayable hydrogels have gained attention in the field of wound healing and anti-scarring due to their ease of application and potential therapeutic properties. One study successfully prepared a sprayable hydrogel containing approximately 128 μg/mL Ni
3(HITP)
2 nanorods with antioxidant and anti-inflammatory properties, accelerating wound healing [
114].
Spray-on hydrogels have shown promise in the field of anti-fibrosis topical therapies. Tan et al. developed a spray-on hydrogel containing 0.01%
w/
w insulin-like growth factor-1 (IGF1). The hydrogel was composed of caffeic acid-modified CS, hydroxypropyl CS, and oxidized dextran. Under the acidic conditions of the wound site, the pH responsive dynamic Schiff base network released IGF1 (~88% within 12 h, ~98% within 48 h) to achieve therapeutic effects. In a mouse model of bacterial infection with full-thickness skin defects, the treatment group exhibited a more mature collagen deposition and alignment, an abundance of hair follicle regeneration, reduced inflammation levels, and the promoted formation of new blood vessels, which convened to realize scar free healing [
115]. Chen et al. designed a HA combined with lyotropic liquid crystal (LLC)-based spray dressing loaded with the antifibrotic drug pirfenidone (PFD, 0.5%
w/
w). Based on the properties of LLC, after the spray comes into contact with the wound, a phase change is triggered, causing the spray to gel and prolonging the release time of PFD (~75% of total drug release over 48 h). In a mouse burn wound model, the treatment group showed decreases in inflammation and interleukin (IL)-6 expression, whereas increases in neovascularization and vascular endothelial growth factor (VEGF) expression, together with stimulated collagen synthesis at appropriate collagen ratios, cumulating in scar prevention [
116].
Spray-on hydrogels form thin, rapidly gelling layers, enabling the flexible application of multiple layered films to cover the wound site and provide distinct, targeted actions. Yang et al. were inspired by the structure and function of natural skin and prepared a sprayable biomimetic double mask (BDM) with rapid autophasing and hierarchical programming. The sprayable BDM consists of a bottom layer including hydrophilic Gel-MA hydrogel with calcium ion (Ca
2+) incorporation and a top layer of hydrophobic poly (lactide-co–propylene glycol–co-lactide) dimethacrylate incorporating the antimicrobial drug triclosan (5%
w/
w). Following spray-on application, the two layers rapidly autophase into bilayered structures and are then bonded and solidified by photocrosslinking. The bottom GelMA layer releases Ca
2+ to achieve hemostasis, while the top PLD layer maintains a wet, gas-permeable, and antimicrobial environment. In both full-thickness rat skin wound models and the full-thickness porcine skin wound models, the prolonged release of triclosan (over 14 days) promoted neovascularization, hair follicle regeneration, and modulated collagen deposition to enhance scar-free wound healing [
117]. Zhong et al. prepared a biodegradable combined multi-functional spray-on hydrogel from select raw materials: a CS-MA (antibacterial) and 0.8%
w/
v ferulic acid (adhesive) layer, and an oxidized
Bletilla striata polysaccharide (hemostasis, anti-inflammatory) layer. The spray-on hydrogel was prepared by dynamic Schiff bond cross-linking and cured by UV-photocrosslinking. Although the extent of dermal fibrosis quality was not assessed in detail, in both a rat model of
S. aureus infected skin defect and miniature pig trauma wound model, the spray-on hydrogel system released ~50% ferulic acid over 24 h to achieve improved wound closure, reduced inflammation levels, and enhanced regeneration of skin appendages [
118].
3.4. 3D Bioprinting of Hydrogels
In addition to the aforementioned methods of composition and use, hydrogels still have many possibilities. Attempts to combine hydrogels with unconventional construction methods such as 3D printing or microneedles have breathed new life into them. 3D printing technology enables the precise fabrication of various materials to meet diverse needs, fulfilling the high demands for geometric complexity in tissue engineering and clinical customization. Appropriate hydrogel materials can be produced through different 3D printing techniques (extrusion, photopolymerization, ultrasound,
etc.) and applied as bionic/artificial skin, hierarchical wound dressings, tissue bonding adhesives, bioelectronic interfaces, and cell-laden scaffold materials, or used to study microtissue/organoid formation or disease model construction [
89,
119,
120,
121,
122,
123,
124,
125].
Taking advantage of the capacity of 3D bioprinting to produce hierarchical and multilayered structural hydrogels, Chen et al. developed a 3D-printed bilayer hydrogel using a dermal ECM-mimicking upper layer of Gel-MA and SF-MA doped with 100 μg/mL copper-epigallocatechin gallate as a lower layer and an epidermal-mimicking Gel-MA/HA-MA upper layer seeded with keratinocytes (1 × 10
6 cells/mL). In a rat model of burn injury, copper-epigallocatechin gallate release from the 3D printed hydrogels (~55% within 3 days, ~75% within 6 days) attenuated the inflammatory response, and in combination with the seeded keratinocytes, improved regenerated dermal thickness with a type I:III collagen ratio resembling healthy skin after 2 weeks [
126]. Liang et al. used 3D printing to develop antibacterial and piezoelectric scaffolds comprising zinc oxide (ZnO, 5%
w/
w) nanoparticle-modified polyvinylidene fluoride (PVDF)/sodium alginate. The constructs offered piezoelectric release models from both vertical swelling and horizontal friction, facilitating bioelectrical stimulation signals that enhanced cell migration, neovascularization, collagen alignment, and growth factor release that promoted scarless healing in a rat model of full thickness skin dorsal defects [
127]. Notably, PVDF/sodium alginate control hydrogels also exhibited scar-reduced wound healing, suggesting that such a polymer blend may influence pro-fibrotic cell phenotypes.
3.5. Microneedle Patch Hydrogels
Microneedle patches, consisting of arrays of microneedles typically ranging from 100 to 2000 μm in length, serve as effective tools for dermal or in vivo drug delivery and monitoring. For dermal treatment, as an emerging tool for painless penetration of the stratum corneum, microneedles are non-invasive with diverse loading capabilities. They can be widely used in a variety of applications such as transdermal drug delivery, stimuli-triggered degradation, disease monitoring, physiological sensing, tissue fluid sampling, and vaccination [
128,
129,
130,
131,
132]. Microneedles patches that use hydrogels as the main body have emerged as a popular strategy for topical pathologies. Hydrogel compositions allow for diversity in terms of preparation materials, microneedle structural design (core-shell structure, bilayer structure, bio-inspired,
etc.), and payload release choices, with the focus on suiting the needs of the corresponding applications [
133,
134,
135]. For example, Yang et al. sought to improve the controlled release of drugs with poor bioavailability into the hypertrophic scar tissue microenvironment to promote its remodeling. They synthesized microneedle patches from Gel-MA and 100 mM 5-Fluorouracil acetic acid (5-FuA) precursors that responded to high levels of reactive oxygen species (ROS) and matrix metalloproteinase (MMP)-2/9 overexpression associated with activated fibroblasts in the wound and scar sites to achieve the controlled release of approximately 75% 5-FuA within 24 h of patch application [
136]. In a rabbit ear model of an established hypertrophic scar, 5-FuA delivery promoted the apoptosis of activated fibroblasts and myofibroblasts, while promoting inflammatory and keratinocyte associated pathways and their interactions with fibroblasts, which controlled excessive collagen deposition during remodeling of the dermal scar.
Targeting of YAP in fibroblast activation and differentiation into myofibroblasts has been demonstrated to be a promising strategy in the temporal control over scar development. Zhang et al. prepared microneedles with a core-shell structure consisting of a ROS-sensitive PVA shell loaded with 3 μg/mL VP and a crosslinked heparin core in combination with photodynamic therapy for inhibition of YAP and promoting scar-free healing and scar repair of back wounds in mice. The release of ~90% VP within the first 24 h resulted in a decreased dermal thickness, reduced collagen deposition, and a lower proportion of type I/III collagen in the tissue [
137]. Liu and colleagues developed a reactive oxygen species (ROS)-responsive, oxygen-generating microneedle patch using a glucose-sensitive sericin/hyaluronic acid (HA) hydrogel loaded with VP. In the highly oxidative infected wound site microenvironment, dopamine functionalized sericin depletes ROS to generate oxygen to alleviate hypoxia, promote angiogenesis, and attenuate the expression of proinflammatory cytokines. Additionally, total VP release within the first 20 h provided sustained inhibition of the YAP/Engrailed-1 axis to assist in the enhanced scarless re-epithelization of diabetic wound models [
138].
Other groups capitalized on the incorporation of cell-inspired therapeutic strategies into their fabricated microneedle patch materials. Li et al. developed a novel microneedle patch from 5%
w/
w adipose-derived stem cell (ADSC) secretome conditioned medium cross-linked with keratin and loaded with 1.5%
w/
w triamcinolone acetonide (TA). The differential and dual release of ADSC secretome (50% over 5 days) and TA (80% in the first 16 h) synergistically reduced inflammation and ROS while regulating myofibroblast and hyperplastic scar fibroblast behavior. In a rabbit ear scar model, the microneedle patches effectively reduced scar formation and facilitated the regeneration of healthy skin [
139]. Liu et al. loaded CAR-TREM2-macrophages targeting DPP4
+ fibroblasts (1 × 10
7 cells/mL) into microporous PLGA/PEG-DA/CaCO
3 hydrogel microneedle patches. Detailed analysis revealed that the microneedle patches attenuated EndMT processes by suppressing leucine-rich-α2-glycoprotein 1 (LRG1). Additionally, CAR-TREM2-macrophages phagocytosed DPP4
+ fibroblasts and suppressed TGF-β secretion, demonstrating effective scar therapy in microneedle patch-treated mouse dorsal scars [
140].
4. Progress towards Clinical Translation
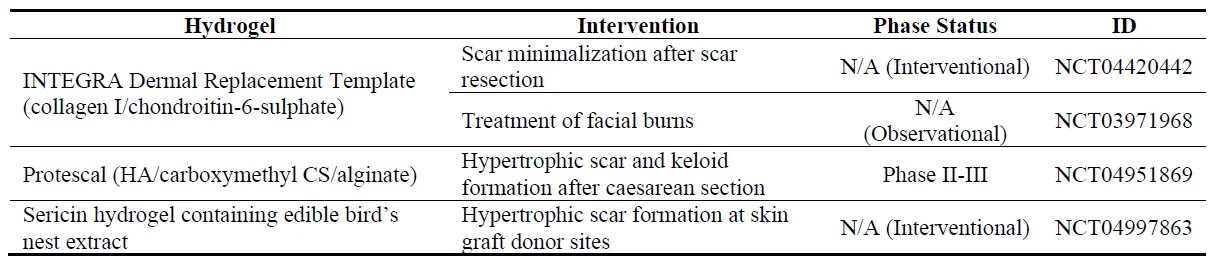
Clinically utilized and over-the-counter products for scar management predominantly consist of silicone-based gel products, ointments, and creams with or without loaded phytomedicines, traditional medicines, or various pharmacological factors. Silicone-based gel sheets, widely used since the 1980s, have proven to be as effective in reducing hypertrophic scar formation as traditional methods such as onion juice application, pressure garments, and compression/massage therapy. The scar-reducing effects of silicone gel sheets remain debated; however, their role as a physical barrier to regulate wound moisture and prevent infection are well-recognized advantages. While many hydrogel-based products have been clinically approved for improving the cosmetic appearance of skin or for use as wound healing dressings, few have been specifically evaluated for the treatment or mitigation of dermal fibrosis. The clinical studies database, https://clinicaltrials.gov (terms Fibrosis OR Cicatrix OR Hypertrophic Scar; Skin; Gel OR Hydrogel, searched 16 November 2024), showed just 4 registered clinical trials that can be considered to involve the assessment of hydrogel therapies ().
. Recently registered clinical trials for hydrogel interventions for dermal fibrosis (N/A, not applicable).
Two of the registered studies aim to assess the effects of INTEGRA Dermal Replacement Template on scar minimalization after scar resection (NCT04420442) and the long-term outcomes following the treatment of third-degree full-thickness facial burns (NCT03971968). The INTEGRA Dermal Replacement Template was clinically approved in the mid-1990s for the clinical treatment of severe burns and can be considered a type of natural polymer cryo-gel scaffold, as it consists of an ECM-like lyophilized layer of bovine collagen type I mixed with chondroitin-6-sulfate. An external polysiloxane/silicone gel sheet layer retains the moist wound environment during healing. Other registered trials include a Phase II-III trial on an injectable or paste-on hydrogel, Protescal (blended HA, carboxymethyl CS, and alginate), to prevent hypertrophic scar and keloid formation after caesarean section (NCT04951869); and an efficacy and safety assessment of a silk-derived sericin-based hydrogel dressing loaded with edible bird’s nest extract (major components include linoleic acid, sialic acid, and essential amino acids) in the mitigation of hypertrophic scar formation at split-thickness skin graft donor sites (NCT04997863). The results of these studies have not yet been published.
The hydrogels used in these clinical trials do not incorporate the loading and release of specific antifibrotic factors or biologics, instead, the focus is on the capacity of the natural polymer components themselves to promote an antifibrotic response. The rationale behind this is likely that it may be easier to meet regulatory requirements by using biomaterials that are already approved by the US FDA. Ultimately, stringent regulatory requirements can pose a significant barrier to the clinical translation of antifibrotic biologic-loaded hydrogel therapies. The lack of clinical trials registered for studying hydrogel application in dermal fibrosis treatment may otherwise be attributed to the complexity of dermal fibrosis types, leading to difficulty in recruiting specific patient populations. Additionally, many of the registered clinical trials evaluating dermal fibrosis tend to utilize intradermal injection, topical gels, or lotion formulations, with an inclination to evaluate the effects of a single pharmacological substance rather than the synergy achieved with hydrogel choice and delivery mode, thus contributing to a gap in registered trials focused on hydrogel applications in the treatment of dermal fibrosis.
There are several challenges and unresolved technical issues that could hinder the clinical translation of hydrogel therapies for dermal fibrosis. These limitations include but are not limited to (i) potential adverse outcomes and reduced efficacy in applications requiring long-term therapy; (ii) a lack of comprehensive understanding of hydrogel base materials, their bioactivity, inherent antifibrotic actions, metabolism, and their synergism with encapsulated payloads; (iii) the need for extensive evaluations of dose-dependent and minimum effective dosages–most of the summarized studies tended to evaluate a single dose and release rate determined from
in vitro observations; and (iv) potential unexpected effects on other cells populating the dermis, thereby potentially obstructing functional skin regeneration.
5. Conclusions
The complex pathogenesis and multiple etiologies that give rise to the various types of dermal fibrosis necessitate developing therapies that address the distinct causes and spatiotemporal processes of wound healing and scar formation. The achievement of different treatment modalities using hydrogel-based strategies has realized effective tools for the mitigation of dermal fibrosis during wound healing, but also offers insights into means to remodel established scar tissue. The majority of studies have evaluated hydrogel therapies in the treatment of trauma scars and hypertrophic scar formation. Keloid scars remain challenging to model effectively in animals, and only a few preclinical scleroderma models can replicate the disease's pathogenesis, such as humanized systemic sclerosis (SSc) models and subcutaneous bleomycin-induced models. Thus, evaluating the effects of hydrogels on keloid fibroblast behavior and in chronic inflammatory skin microenvironments would help to determine the broader applicability of anti-scarring hydrogels.
Here, we summarized recently developed hydrogels that have been applied to mitigate dermal fibrosis. Cryo-gel dressings remain prevalent in topical treatment of wounds, given their capability to absorb wound exudate and maintain a wet wound microenvironment while releasing bioactive to regulate the wound healing process. However, the rapid degradation of cryogels necessitates frequent dressing changes and requires securing the cryogel to the wound site, which may impact patient compliance. Spray-on hydrogels are inherently adhesive, excel at wound coverage, and create a waterproof barrier with prolonged application time, but may be limited in the reservoir of bioactive that can be supplied in a single treatment. In contrast, injectable hydrogels undergo in situ gelation, forming a depot that enables the extended release of bioactives into the surrounding microenvironment. Microneedle patches offer an alternative mode of adhesion that is easy for patients to self-administer, promoting compliance. They also provide a solution for the extended release of bioactives from the microneedle reservoirs. The non-invasiveness, depth of bioactive delivery, and relative ease of manufacture have propelled microneedle patches to the forefront of dermal fibrosis therapies. Besides the advancements in hydrogel strategies summarized here, there remains the prospect of utilizing other hydrogel strategies to target the plethora of mechanisms involved in scar formation during dermal wound repair by selecting appropriate hydrogel components and optimizing their structural arrangement. For example, gradated and hierarchical 3D printed hydrogels for spatiotemporal control of scarless healing; anisotropic hydrogels that exploit the mechanosensitive myofibroblast behavior formation; and combining degradable scaffold-hydrogel hybrid constructs for wound healing of tissues under tension have yet to be fully explored.
Statement of the Use of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this manuscript, Microsoft Word’s built-in Microsoft Translator and Office 365 Copilot tools were used to translate certain sections originally drafted in Chinese into English. All translated content was thoroughly reviewed, edited, and verified by the authors to ensure accuracy, consistency, and alignment with the review’s original intent. The authors take full responsibility for the final content of the article.
Acknowledgments
The figures in this manuscript were initially designed using Figdraw (www.figdraw.com) before further adaption and customization. The authors would also like to thank colleagues Yifan Tai and Junwu Liu (Nankai University) for their helpful suggestions.
Author Contributions
Conceptualization, Y.W., Z.L. and A.C.M.; Methodology, Y.W. and Z.L.; Writing—Original Draft Preparation, Y.W., Z.L., C.Z. and Z.J.; Writing—Review & Editing, A.C.M.; Software, C.Z. and Z.J.; Visualization, C.Z., Z.J. and A.C.M.; Supervision, A.C.M.; Project Administration, A.C.M.; Funding Acquisition, A.C.M.
Ethics Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Funding
The authors are supported and funded by the National Natural Science Foundation of China (NSFC) grant number 82250610231 and the Nankai University Hundred Young Academic Leaders Program.
Declaration of Competing Interest
The author declares no conflicts of interest.
References
-
1.
Bonnans C, Chou J, Werb Z. Remodelling
the
extracellular
matrix
in
development
and
disease.
Nat. Rev. Mol. Cell Biol. 2014,
15, 786–801.
[Google Scholar]
-
2.
Ruiz-Ortega M, Rayego-Mateos S, Lamas S, Ortiz A, Rodrigues-Diez RR. Targeting
the
progression
of
chronic
kidney
disease.
Nat. Rev. Nephrol. 2020,
16, 269–288.
[Google Scholar]
-
3.
Peiseler M, Schwabe R, Hampe J, Kubes P, Heikenwälder M, Tacke F. Immune
mechanisms
linking
metabolic
injury
to
inflammation
and
fibrosis
in
fatty
liver
disease
—Novel
insights
into
cellular
communication
circuits.
J. Hepatol. 2022,
77, 1136–1160.
[Google Scholar]
-
4.
Foster DS, Januszyk M, Yost KE, Chinta MS, Gulati GS, Nguyen AT, et al. Integrated
spatial
multiomics
reveals
fibroblast
fate
during
tissue
repair.
Proc. Natl. Acad. Sci. USA 2021,
118, e2110025118.
[Google Scholar]
-
5.
Liu M, Xu J, Deng H. Tangled
fibroblasts
in
tumor-stroma
interactions.
Int. J. Cancer 2011,
129, 1795–1805.
[Google Scholar]
-
6.
Rockey DC, Bell PD, Hill JA. Fibrosis
—A
Common
Pathway
to
Organ
Injury
and
Failure.
N. Engl. J. Med. 2015,
372, 1138–1149.
[Google Scholar]
-
7.
Bergeron C, Cantin AM.
Cystic
Fibrosis:
Pathophysiology
of
Lung
Disease.
Semin. Respir. Crit. Care Med. 2019,
40, 715–726.
[Google Scholar]
-
8.
Yanai H, Toren D, Vierlinger K, Hofner M, Nöhammer C, Chilosi M, et al. Wound
healing
and
longevity:
Lessons
from
long-lived
αMUPA
mice.
Aging 2015,
7, 167–176.
[Google Scholar]
-
9.
Alkhaleq HA, Karram T, Fokra A, Hamoud S, Kabala A, Abassi Z. The
Protective
Pathways
Activated
in
Kidneys
of
αMUPA
Transgenic
Mice
Following
Ischemia\Reperfusion-Induced
Acute
Kidney
Injury.
Cells 2023,
12, 2497.
[Google Scholar]
-
10.
Henderson NC, Rieder F, Wynn TA. Fibrosis:
From
mechanisms
to
medicines.
Nature 2020,
587, 555–566.
[Google Scholar]
-
11.
Talbott HE, Mascharak S, Griffin M, Wan DC, Longaker MT. Wound
healing,
fibroblast
heterogeneity,
and
fibrosis.
Cell Stem Cell 2022,
29, 1161–1180.
[Google Scholar]
-
12.
Xu Z, Chen D, Hu Y, Jiang K, Huang H, Du Y, et al. Anatomically
distinct
fibroblast
subsets
determine
skin
autoimmune
patterns.
Nature 2022,
601, 118–124.
[Google Scholar]
-
13.
Jacob M, Chang L, Pure E. Fibroblast
Activation
Protein
in
Remodeling
Tissues.
Curr. Mol. Med. 2012,
12, 1220–1243.
[Google Scholar]
-
14.
Huang X, Yang N, Fiore VF, Barker TH, Sun Y, Morris SW, et al. Matrix
Stiffness
–Induced
Myofibroblast
Differentiation
Is
Mediated
by
Intrinsic
Mechanotransduction.
Am. J. Respir. Cell Mol. Biol. 2012,
47, 340–348.
[Google Scholar]
-
15.
Demircioglu F, Wang J, Candido J, Costa ASH, Casado P, de Luxan Delgado B, et al. Cancer
associated
fibroblast
FAK
regulates
malignant
cell
metabolism.
Nat. Commun. 2020,
11, 1290.
[Google Scholar]
-
16.
Nabhan AN, Brownfield DG, Harbury PB, Krasnow MA, Desai TJ. Single-cell
Wnt
signaling
niches
maintain
stemness
of
alveolar
type
2
cells.
Science 2018,
359, 1118–1123.
[Google Scholar]
-
17.
Liu M, López de Juan Abad B, Cheng K. Cardiac
fibrosis:
Myofibroblast-mediated
pathological
regulation
and
d
rug
delivery
strategies.
Adv. Drug Del. Rev. 2021,
173, 504–519.
[Google Scholar]
-
18.
Tzavlaki K, Moustakas A.
TGF-β
Signaling.
Biomolecules 2020,
10, 487.
[Google Scholar]
-
19.
Griffin MF, Huber J, Evan FJ, Quarto N, Longaker MT.
The
role
of
Wnt
signaling
in
skin
fibrosis.
Med. Res. Rev. 2022,
42, 615–628.
[Google Scholar]
-
20.
Tai Y, Woods EL, Dally J, Kong D, Steadman R, Moseley R, et al.
Myofibroblasts:
Function,
Formation,
and
Scope
of
Molecular
Therapies
for
Skin
Fibrosis.
Biomolecules 2021,
11, 1095.
[Google Scholar]
-
21.
Swigris JJ, Brown KK.
The
Role
of
Endothelin-1
in
the
Pathogenesis
of
Idiopathic
Pulmonary
Fibrosis.
Biodrugs 2010,
24, 49–54.
[Google Scholar]
-
22.
Pesce M, Duda GN, Forte G, Girao H, Raya A, Roca-Cusachs P, et al.
Cardiac
fibroblasts
and
mechanosensation
in
heart
development,
health
and
disease.
Nat. Rev. Cardiol. 2023,
20, 309–324.
[Google Scholar]
-
23.
Bhattacharya M, Ramachandran P. Immunology
of
human
fibrosis.
Nat. Immunol. 2023,
24, 1423–1433.
[Google Scholar]
-
24.
Hecker L, Logsdon NJ, Kurundkar D, Kurundkar A, Bernard K, Hock T, et al. Reversal
of
Persistent
Fibrosis
in
Aging
by
Targeting
Nox4-Nrf2
Redox
Imbalance.
Sci. Transl. Med. 2014,
6, 231ra247.
[Google Scholar]
-
25.
Kim DH, Xing T, Yang Z, Dudek R, Lu Q, Chen Y-H. Epithelial
Mesenchymal
Transition
in
Embryonic
Development,
Tissue
Repair
and
Cancer:
A
Comprehensive
Overview.
J. Clin. Med. 2018,
7, 1.
[Google Scholar]
-
26.
Lovisa S, LeBleu VS, Tampe B, Sugimoto H, Vadnagara K, Carstens JL, et al.
Epithelial-to-mesenchymal
transition
induces
cell
cycle
arrest
and
parenchymal
damage
in
renal
fibrosis.
Nat. Med. 2015,
21, 998–1009.
[Google Scholar]
-
27.
Ni H, Chen M, Dong D, Zhou Y, Cao Y, Ge R, et al. CYLD/HDAC6
signaling
regulates
the
interplay
between
epithelial-mesenchymal
transition
and
ciliary
homeostasis
during
pulmonary
fibrosis.
Cell Death Dis. 2024,
15, 581.
[Google Scholar]
-
28.
Lamouille S, Xu J, Derynck R.
Molecular
mechanisms
of
epithelial
–mesenchymal
transition.
Nat. Rev. Mol. Cell Biol. 2014,
15, 178–196.
[Google Scholar]
-
29.
Marconi GD, Fonticoli L, Rajan TS, Pierdomenico SD, Trubiani O, Pizzicannella J, et al. Epithelial-Mesenchymal
Transition
(EMT):
The
Type-2
EMT
in
Wound
Healing,
Tissue
Regeneration
and
Organ
Fibrosis.
Cells 2021,
10, 1587.
[Google Scholar]
-
30.
Yan C, Grimm WA, Garner WL, Qin L, Travis T, Tan N, et al. Epithelial
to
mesenchymal
transition
in
human
skin
wound
healing
is
induced
by
tumor
necrosis
factor-alpha
through
bone
morphogenic
protein-2.
Am. J. Pathol. 2010,
176, 2247–2258.
[Google Scholar]
-
31.
Welch-Reardon KM, Wu N, Hughes CCW. A
Role
for
Partial
Endothelial
–Mesenchymal
Transitions
in
Angiogenesis?
Arterioscler. Thromb. Vasc. Biol. 2015,
35, 303–308.
[Google Scholar]
-
32.
Xu Y, Kovacic JC. Endothelial
to
Mesenchymal
Transition
in
Health
and
Disease.
Annu. Rev. Physiol. 2023,
85, 245–267.
[Google Scholar]
-
33.
Zhao J, Patel J, Kaur S, Sim S-L, Wong HY, Styke C, et al. Sox9
and
Rbpj
differentially
regulate
endothelial
to
mesenchymal
transition
and
wound
scarring
in
murine
endovascular
progenitors.
Nat. Commun. 2021,
12, 2564.
[Google Scholar]
-
34.
Meng X-M, Wang S, Huang X-R, Yang C, Xiao J, Zhang Y, et al.
Inflammatory
macrophages
can
transdifferentiate
into
myofibroblasts
during
renal
fibrosis.
Cell Death Dis. 2016,
7, e2495.
[Google Scholar]
-
35.
Wei J, Xu Z, Yan X. The
role
of
the
macrophage-to-myofibroblast
transition
in
renal
fibrosis.
Front. Immunol. 2022,
13, 934377.
[Google Scholar]
-
36.
Zhu L, Liu L, Wang A, Liu J, Huang X, Zan T. Positive
feedback
loops
between
fibroblasts
and
the
mechanical
environment
contribute
to
dermal
fibrosis.
Matrix Biol. 2023,
121, 1–21.
[Google Scholar]
-
37.
Gauglitz GG, Korting HC, Pavicic T, Ruzicka T, Jeschke MG. Hypertrophic
Scarring
and
Keloids:
Pathomechanisms
and
Current
and
Emerging
Treatment
Strategies.
Mol. Med. 2011,
17, 113–125.
[Google Scholar]
-
38.
Ogawa R. The
Most
Current
Algorithms
for
the
Treatment
and
Prevention
of
Hypertrophic
Scars
and
Keloids:
A
2020
Update
of
the
Algorithms
Published
10
Years
Ago.
Plast. Reconstr. Surg. 2022,
149, 79e–94e.
[Google Scholar]
-
39.
Rose LF, Wu JC, Carlsson AH, Tucker DI, Leung KP, Chan RK. Recipient
wound
bed
characteristics
affect
scarring
and
skin
graft
contraction.
Wound Repair. Regen. 2015,
23, 287–296.
[Google Scholar]
-
40.
Slemp AE, Kirschner RE. Keloids
and
scars:
A
review
of
keloids
and
scars,
their
pathogenesis,
risk
factors,
and
management.
Curr. Opin. Pediatr. 2006,
18, 396–402.
[Google Scholar]
-
41.
Sephel G, Woodward SC. Repair, Regeneration, and Fibrosis. In Rubin's Pathology: Clinicopathologic Foundations of Medicine, 5th ed.; Chapter 3: Repair, Regeneration, and Fibrosis; Wolters Kluwer: Philadelphia, PA, USA, 2008; pp. 84–116.
-
42.
Stekelenburg CM, Marck RE, Tuinebreijer WE, de Vet HCW, Ogawa R, van Zuijlen PPM. A
systematic
review
on
burn
scar
contracture
treatment:
Searching
for
evidence.
J. Burn. Care Res. 2015,
36, e153–e161.
[Google Scholar]
-
43.
Andrews JP, Marttala J, Macarak E, Rosenbloom J, Uitto J. Keloids:
The
paradigm
of
skin
fibrosis
—Pathomechanisms
and
treatment.
Matrix Biol. 2016,
51, 37–46.
[Google Scholar]
-
44.
Ehrlich HP, Desmoulière A, Diegelmann RF, Cohen IK, Compton CC, Garner WL, et al. Morphological
and
immunochemical
differences
between
keloid
and
hypert
rophic
scar.
Am. J. Pathol. 1994,
145, 105–113.
[Google Scholar]
-
45.
Shi Z, Liu Z, Wei Y, Zhang R, Deng Y, Li D. The
role
of
dermal
fibroblasts
in
autoimmune
skin
diseases.
Front. Immunol. 2024,
15, 1379490.
[Google Scholar]
-
46.
Varrica C, Dias HS, Reis C, Carvalheiro M, Simões S. Targeted
delivery
in
scleroderma
fibrosis.
Autoimmun. Rev. 2021,
20, 102730.
[Google Scholar]
-
47.
Barriga M, Benitez R, Robledo G, Caro M, O’Valle F, Campos-Salinas J, et al.
Neuropeptide
Cortistatin
Regulates
Dermal
and
Pulmonary
Fibrosis
in
an
Experimental
Model
of
Systemic
Sclerosis.
Neuroendocrinology 2021,
112, 784–795.
[Google Scholar]
-
48.
Tabib T, Huang M, Morse N, Papazoglou A, Behera R, Jia M, et al.
Myofibroblast
transcriptome
indicates
SFRP2hi
fibroblast
progenitors
in
systemic
sclerosis
skin.
Nat. Commun. 2021,
12, 4384.
[Google Scholar]
-
49.
Zhao M, Wu J, Wu H, Sawalha AH, Lu Q. Clinical
Treatment
Options
in
Scleroderma:
Recommendations
and
Comprehensive
Review.
Clin. Rev. Allergy Immunol. 2022,
62, 273–291.
[Google Scholar]
-
50.
Frech FS, Hernandez L, Urbonas R, Zaken GA, Dreyfuss I, Nouri K. Hypertrophic
Scars
and
Keloids:
Advances
in
Treatment
and
Review
of
Established
Therapies.
Am. J. Clin. Dermatol. 2023,
24, 225–245.
[Google Scholar]
-
51.
Voth H, Landsberg J, Hinz T, Wenzel J, Bieber T, Reinhard G, et al. Management
of
dermatofibrosarcoma
protuberans
with
fibrosarcomatous
transformation:
An
evidence-based
review
of
the
literature.
J. Eur. Acad. Dermatol. Venereol. 2011,
25, 1385–1391.
[Google Scholar]
-
52.
Sabater-Marco V, Pérez-Vallés A, Berzal-Cantalejo F, Rodriguez-Serna M, Martinez-Diaz F, Martorell-Cebollada M.
Sclerosing
dermatofibrosarcoma
protuberans
(DFSP):
An
unusual
variant
with
focus
on
the
histopathologic
differential
diagnosis.
Int. J. Dermatol. 2006,
45, 59–62.
[Google Scholar]
-
53.
Lens MB, Newton-Bishop JA, Boon AP. Desmoplastic
malignant
melanoma:
A
systematic
review.
Br. J. Dermatol. 2005,
152, 673–678.
[Google Scholar]
-
54.
Zhu H, Liu Q, Miao L, Musetti S, Huo M, Huang L. Remodeling
the
fibrotic
tumor
microenvironment
of
desmoplastic
melanoma
to
facilitate
vaccine
immunotherapy.
Nanoscale 2020,
12, 3400–3410.
[Google Scholar]
-
55.
Boada Garcia A, Quer Pi-Sunyer A, Richarz N, Jaka-Moreno A. Actualización
en
el
diagnóstico
y
manejo
del
melanoma
desmoplásico.
Actas Dermosifiliogr. 2022,
113, 47–57.
[Google Scholar]
-
56.
Zeiser R, Blazar BR. Acute
Graft-versus-Host
Disease
—Biologic
Process,
Prevention,
and
Therapy.
N. Engl. J. Med. 2017,
377, 2167–2179.
[Google Scholar]
-
57.
Baumrin E, Loren AW, Falk SJ, Mays JW, Cowen EW. Chronic
graft-versus-host
disease.
Part
I:
Epidemiology,
pathogenesis,
and
clinical
manifestations.
J. Am. Acad. Dermatol. 2024,
90, 1–16.
[Google Scholar]
-
58.
Strong Rodrigues K, Oliveira-Ribeiro C, de Abreu Fiuza Gomes S, Knobler R.
Cutaneous
Graft-Versus-Host
Disease:
Diagnosis
and
Treatment.
Am. J. Clin. Dermatol. 2018,
19, 33–50.
[Google Scholar]
-
59.
Chakraverty R, Teshima T.
Graft-versus-host
disease:
A
disorder
of
tissue
regeneration
and
repair.
Blood 2021,
138, 1657–1665.
[Google Scholar]
-
60.
Zhang J, Yu H, Man M-Q, Hu L. Aging
in
the
dermis:
Fibroblast
senescence
and
its
significance.
Aging Cell 2024,
23, e14054.
[Google Scholar]
-
61.
Midgley AC, Bowen T, Phillips AO, Steadman R. MicroRNA-7
inhibition
rescues
age-associated
loss
of
epidermal
growth
factor
receptor
and
hyaluronan-dependent
differentiation
in
fibroblasts.
Aging Cell 2014,
13, 235–244.
[Google Scholar]
-
62.
Midgley AC, Morris G, Phillips AO, Steadman R. 17β-estradiol
ameliorates
age-associated
loss
of
fibroblast
function
by
attenuating
IFN-γ/STAT1-dependent
miR-7
upregulation.
Aging Cell 2016,
15, 531–541.
[Google Scholar]
-
63.
Nishiguchi MA, Spencer CA, Leung DH, Leung TH. Aging
Suppresses
Skin-Derived
Circulating
SDF1
to
Promote
Full-Thickness
Tissue
Regeneration.
Cell Rep. 2018,
24, 3383–3392.e3385.
[Google Scholar]
-
64.
Fu Z, Sun H, Wu Y, Li C, Wang Y, Liu Y, et al.
A
cyclic
heptapeptide-based
hydrogel
boosts
the
healing
of
chronic
skin
wounds
in
diabetic
mice
and
patients.
NPG Asia Mater. 2022,
14, 99.
[Google Scholar]
-
65.
Griffin DR, Archang MM, Kuan C-H, Weaver WM, Weinstein JS, Feng AC, et al.
Activating
an
adaptive
immune
response
from
a
hydrogel
scaffold
imparts
regenerative
wound
healing.
Nat. Mater. 2021,
20, 560–569.
[Google Scholar]
-
66.
Xu L, Gao S, Guo Q, Wang C, Qiao Y, Qiu D. A
Solvent-Exchange
Strategy
to
Regulate
Noncovalent
Interactions
for
Strong
and
Antiswelling
Hydrogels.
Adv. Mater. 2020,
32, 2004579.
[Google Scholar]
-
67.
Li C, He X, Li Q, Lv M, Shen J, Jin L, et al. A
photothermal-response
oxygen
release
platform
based
on
a
hydrogel
for
accelerating
wound
healing.
NPG Asia Mater. 2023,
15, 3.
[Google Scholar]
-
68.
Liu W, Gao R, Yang C, Feng Z, Ou-Yang W, Pan X, et al. ECM-mimetic
immunomodulatory
hydrogel
for
methicillin-resistant
Staphylococcus aureus–infected
chronic
skin
wound
healing.
Sci. Adv. 2022,
8, eabn7006.
[Google Scholar]
-
69.
Park GR, Gwak MA, Choi YH, Park WH. pH-sensitive
gallol-rich
chitosan
hydrogel
beads
for
on-off
controlled
drug
delivery.
Int. J. Biol. Macromol. 2023,
240, 124346.
[Google Scholar]
-
70.
Chen Y, Wang X, Tao S, Wang Q, Ma P-Q, Li Z-B, et al. Research
advances
in
smart
responsive-hydrogel
dressings
with
potential
clinical
diabetic
wound
healing
properties.
Mil. Med. Res. 2023,
10, 37.
[Google Scholar]
-
71.
Santhamoorthy M, Thirupathi K, Kumar SSD, Pandiaraj S, Rahaman M, Phan TTV, et al. k-Carrageenan
based
magnetic@polyelectrolyte
complex
composite
hydrogel
for
pH
and
temperature-responsive
curcumin
delivery.
Int. J. Biol. Macromol. 2023,
244, 125467.
[Google Scholar]
-
72.
Peng X, Peng Q, Wu M, Wang W, Gao Y, Liu X, et al. A
pH
and
Temperature
Dual-Responsive
Microgel-Embedded,
Adhesive,
and
Tough
Hydrogel
for
Drug
Delivery
and
Wound
Healing.
ACS Appl. Mater. Interfaces 2023,
15, 19560–19573.
[Google Scholar]
-
73.
Zha K, Xiong Y, Zhang W, Tan M, Hu W, Lin Z, et al. Waste
to
Wealth:
Near-Infrared/pH
Dual-Responsive
Copper-Humic
Acid
Hydrogel
Films
for
Bacteria-Infected
Cutaneous
Wound
Healing.
ACS Nano 2023,
17, 17199–17216.
[Google Scholar]
-
74.
Kang Y, Xu L, Dong J, Yuan X, Ye J, Fan Y, et al. Programmed
microalgae-gel
promotes
chronic
wound
healing
in
diabetes.
Nat. Commun. 2024,
15, 1042.
[Google Scholar]
-
75.
Chen G, Wang F, Zhang X, Shang Y, Zhao Y. Living
microecological
hydrogels
for
wound
healing.
Sci. Adv. 2023,
9, eadg3478.
[Google Scholar]
-
76.
Zhao M, Kang M, Wang J, Yang R, Zhong X, Xie Q, et al. Stem
Cell-Derived
Nanovesicles
Embedded
in
Dual-Layered
Hydrogel
for
Programmed
ROS
Regulation
and
Comprehensive
Tissue
Regeneration
in
Burn
Wound
Healing.
Adv. Mater. 2024,
36, 2401369.
[Google Scholar]
-
77.
Deng X, Wu Y, Tan Y, Ge Z, Wang D, Zheng C, et al. Microenvironment-responsive smart hydrogels with antibacterial activity and immune regulation for accelerating chronic wound healing.
J. Con. Release. 2024,
368, 518–532.
[Google Scholar]
-
78.
Chen K, Henn D, Januszyk M, Barrera JA, Noishiki C, Bonham CA, et al.
Disrupting
mechanotransduction
decreases
fibrosis
and
contracture
in
split-thickness
skin
grafting.
Sci. Transl. Med. 2022,
14, eabj9152.
[Google Scholar]
-
79.
Li L, Liu C, Fu J, Wang Y, Yang D, Peng B, et al. CD44
targeted
indirubin
nanocrystal-loaded
hyaluronic
acid
hydrogel
for
the
treatment
of
psoriasis.
Int. J. Biol. Macromol. 2023,
243, 125239.
[Google Scholar]
-
80.
Wei G, Liu Q, Wang X, Zhou Z, Zhao X, Zhou W, et al. A
probiotic
nanozyme
hydrogel
regulates
vaginal
microenvironment
for
Candida vaginitis
therapy.
Sci. Adv. 2023,
9, eadg0949.
[Google Scholar]
-
81.
Palaoro AV, Dalosto MM, Coutinho C, Santos S. Assessing
the
importance
of
burrows
through
behavioral
observations
of
Parastacus
brasiliensis,
a
Neotropical
burrowing
crayfish
(Crustacea),
in
laboratory
conditions.
Zool. Stud. 2013,
52, 4.
[Google Scholar]
-
82.
Zhang Y, Fang M, Xie W, Zhang Y-a, Jiang C, Li N, et al. Sprayable
alginate
hydrogel
dressings
with
oxygen
production
and
exosome
loading
for
the
treatment
of
diabetic
wounds.
Int. J. Biol. Macromol. 2023,
242, 125081.
[Google Scholar]
-
83.
Xu X, Zeng Y, Chen Z, Yu Y, Wang H, Lu X, et al. Chitosan-based
multifunctional
hydrogel
for
sequential
wound
inflammation
elimination,
infection
inhibition,
and
wound
healing.
Int. J. Biol. Macromol. 2023,
235, 123847.
[Google Scholar]
-
84.
Zhang X, Gan J, Fan L, Luo Z, Zhao Y. Bioinspired
Adaptable
Indwelling
Microneedles
for
Treatment
of
Diabetic
Ulcers.
Adv. Mater. 2023,
35, 2210903.
[Google Scholar]
-
85.
Zhou H, Zhang S, Lei M, Cai Y, Wang H, Sun J, et al. A
suture-free,
shape
self-adaptive
and
bioactive
PEG-Lysozyme
implant
for
Corneal
stroma
defect
repair
and
rapid
vision
restoration.
Bioact. Mater. 2023,
29, 1–15.
[Google Scholar]
-
86.
Zhou C, Wang C, Xu K, Niu Z, Zou S, Zhang D, et al. Hydrogel
platform
with
tunable
stiffness
based
on
magnetic
nanoparticles
cross-linked
GelMA
for
cartilage
regeneration
and
its
intrinsic
biomechanism.
Bioact. Mater. 2023,
25, 615–628.
[Google Scholar]
-
87.
Chen M, Lu Y, Liu Y, Liu Q, Deng S, Liu Y, et al. Injectable
Microgels
with
Hybrid
Exosomes
of
Chondrocyte-Targeted
FGF18
Gene-Editing
and
Self-Renewable
Lubrication
for
Osteoarthritis
Therapy.
Adv. Mater. 2024,
36, 2312559.
[Google Scholar]
-
88.
Pranantyo D, Yeo CK, Wu Y, Fan C, Xu X, Yip YS, et al. Hydrogel
dressings
with
intrinsic
antibiofilm
and
antioxidative
dual
functionalities
accelerate
infected
diabetic
wound
healing.
Nat. Commun. 2024,
15, 954.
[Google Scholar]
-
89.
Laurén I, Farzan A, Teotia A, Lindfors NC, Seppälä J.
Direct
ink
writing
of
biocompatible
chitosan/non-isocyanate
polyurethane/cellulose
nanofiber
hydrogels
for
wound-healing
applications.
Int. J. Biol. Macromol. 2024,
259, 129321.
[Google Scholar]
-
90.
Xiao L, Xie P, Ma J, Shi K, Dai Y, Pang M, et al. A
Bioinspired
Injectable,
Adhesive,
and
Self-Healing
Hydrogel
with
Dual
Hybrid
Network
for
Neural
Regeneration
after
Spinal
Cord
Injury.
Adv. Mater. 2023,
35, 2304896.
[Google Scholar]
-
91.
Luo X, Fong ELS, Zhu C, Lin QXX, Xiong M, Li A, et al.
Hydrogel-based
colorectal
cancer
organoid
co-culture
models.
Acta Biomater. 2021,
132, 461–472.
[Google Scholar]
-
92.
Tian G, Yang D, Liang C, Liu Y, Chen J, Zhao Q, et al. A
Nonswelling
Hydrogel
with
Regenerable
High
Wet
Tissue
Adhesion
for
Bioelectronics.
Adv. Mater. 2023,
35, 2212302.
[Google Scholar]
-
93.
Cohen-Gerassi D, Messer O, Finkelstein-Zuta G, Aviv M, Favelukis B, Shacham-Diamand Y, et al. Conductive
Peptide-Based
MXene
Hydrogel
as
a
Piezoresistive
Sensor.
Adv. Healthc. Mater. 2024,
13, 2303632.
[Google Scholar]
-
94.
Lin Z, Fan D, Li G, He L, Qin X, Zhao B, et al.
Antibacterial,
Adhesive,
and
Conductive
Hydrogel
for
Diabetic
Wound
Healing.
Macromol. Biosci. 2023,
23, 2200349.
[Google Scholar]
-
95.
Sun A, Hu D, He X, Ji X, Li T, Wei X, et al. Mussel-inspired
hydrogel
with
injectable
self-healing
and
antibacterial
properties
promotes
wound
healing
in
burn
wound
infection.
NPG Asia Mater. 2022,
14, 86.
[Google Scholar]
-
96.
Yang L, Gao Y, Liu Q, Li W, Li Z, Zhang D, et al. A
Bacterial
Responsive
Microneedle
Dressing
with
Hydrogel
Backing
Layer
for
Chronic
Wound
Treatment.
Small 2024,
20, 2307104.
[Google Scholar]
-
97.
Du X, Liu Y, Wang X, Yan H, Wang L, Qu L, et al.
Injectable
hydrogel
composed
of
hydrophobically
modified
chitosan/oxidized-dextran
for
wound
healing.
Mater. Sci. Eng. C 2019,
104, 109930.
[Google Scholar]
-
98.
Shen J, Jiao W, Chen Z, Wang C, Song X, Ma L, et al. Injectable
multifunctional
chitosan/dextran-based
hydrogel
accelerates
wound
healing
in
combined
radiation
and
burn
injury.
Carbohydr. Polym. 2023,
316, 121024.
[Google Scholar]
-
99.
Yang C, Zhang Y, Zhang X, Tang P, Zheng T, Ran R, et al.
An
injectable,
self-healing,
and
antioxidant
collagen-
and
hyaluronic
acid-based
hydrogel
mediated
with
gallic
acid
and
dopamine
for
wound
repair.
Carbohydr. Polym. 2023,
320, 121231.
[Google Scholar]
-
100.
Hu Y, Jia Y, Wang S, Ma Y, Huang G, Ding T, et al. An
ECM-Mimicking,
Injectable,
Viscoelastic
Hydrogel
for
Treatment
of
Brain
Lesions.
Adv. Healthc. Mater. 2023,
12, 2201594.
[Google Scholar]
-
101.
Zhao X, Luo J, Huang Y, Mu L, Chen J, Liang Z, et al. Injectable
Antiswelling
and
High-Strength
Bioactive
Hydrogels
with
a
Wet
Adhesion
and
Rapid
Gelling
Process
to
Promote
Sutureless
Wound
Closure
and
Scar-free
Repair
of
Infectious
Wounds.
ACS Nano 2023,
17, 22015–22034.
[Google Scholar]
-
102.
Zhang J, Zheng Y, Lee J, Hua J, Li S, Panchamukhi A, et al. A
pulsatile
release
platform
based
on
photo-induced
imine-crosslinking
hydrogel
promotes
scarless
wound
healing.
Nat. Commun. 2021,
12, 1670.
[Google Scholar]
-
103.
Zheng X, Ding Z, Cheng W, Lu Q, Kong X, Zhou X, et al. Microskin-Inspired
Injectable
MSC-Laden
Hydrogels
for
Scarless
Wound
Healing
with
Hair
Follicles.
Adv. Healthc. Mater. 2020,
9, 2000041.
[Google Scholar]
-
104.
Deng J, Li J, Yan L, Guo W, Ding X, Ding P, et al. Accelerated,
injectable,
self-healing,
scarless
wound
dressings
using
rGO
reinforced
dextran/chitosan
hydrogels
incorporated
with
PDA-loaded
asiaticoside.
Int. J. Biol. Macromol. 2024,
278, 134424.
[Google Scholar]
-
105.
Zhang L, Tan X, Dong C, Zou L, Zhao H, Zhang X, et al. In
vitro
differentiation
of
human
umbilical
cord
mesenchymal
stem
cells
(hUCMSCs),
derived
from
Wharton’s
jelly,
into
choline
acetyltransferase
(ChAT)-positive
cells.
Int. J. Dev. Neurosci. 2012,
30, 471–477.
[Google Scholar]
-
106.
Razavi M, Primavera R, Kevadiya BD, Wang J, Buchwald P, Thakor AS. A
Collagen
Based
Cryogel
Bioscaffold
that
Generates
Oxygen
for
Islet
Transplantation.
Adv. Funct. Mater. 2020,
30, 1902463.
[Google Scholar]
-
107.
Liu X, Sun Y, Wang J, Kang Y, Wang Z, Cao W, et al. A
tough,
antibacterial
and
antioxidant
hydrogel
dressing
accelerates
wound
healing
and
suppresses
hypertrophic
scar
formation
in
infected
wounds.
Bioact. Mater. 2024,
34, 269–281.
[Google Scholar]
-
108.
Zhang L, Yan H, Tai Y, Xue Y, Wei Y, Wang K, et al. Design
and
Evaluation
of
a
Polypeptide
that
Mimics
the
Integrin
Binding
Site
for
EDA
Fibronectin
to
Block
Profibrotic
Cell
Activity.
Int. J. Mol. Sci. 2021,
22, 1575.
[Google Scholar]
-
109.
Zhang L, Tai Y, Liu X, Liu Y, Dong Y, Liu Y, et al. Natural
polymeric
and
peptide-loaded
composite
wound
dressings
for
scar
prevention.
Appl. Mater. Today 2021,
25, 101186.
[Google Scholar]
-
110.
Fan R, Zhao J, Yi L, Yuan J, McCarthy A, Li B, et al. Anti-Inflammatory
Peptide-Conjugated
Silk
Fibroin/Cryogel
Hybrid
Dual
Fiber
Scaffold
with
Hierarchical
Structure
Promotes
Healing
of
Chronic
Wounds.
Adv. Mater. 2024,
36, 2307328.
[Google Scholar]
-
111.
Ying X, Yu C, Yang W, Ye L, Sun R, Gu T, et al. The
transformation
of
multifunctional
bio-patch
to
hydrogel
on
skin
wounds
for
efficient
scarless
wound
healing.
Mater. Today Bio 2024,
24, 100901.
[Google Scholar]
-
112.
Chen K, Liu Y, Liu X, Guo Y, Liu J, Ding J, et al. Hyaluronic
acid-modified
and
verteporfin-loaded
polylactic
acid
nanogels
promote
scarless
wound
healing
by
accelerating
wound
re-epithelialization
and
controlling
scar
formation.
J. Nanobiotechnol. 2023,
21, 241.
[Google Scholar]
-
113.
Liao Y, Xie L, Ye J, Chen T, Huang T, Shi L, et al. Sprayable
hydrogel
for
biomedical
applications.
Biomater. Sci. 2022,
10, 2759–2771.
[Google Scholar]
-
114.
Zhang W, Dai X, Jin X, Huang M, Shan J, Chen X, et al. Promotion
of
wound
healing
by
a
thermosensitive
and
sprayable
hydrogel
with
nanozyme
activity
and
anti-inflammatory
properties.
Smart Mater. Med. 2023,
4, 134–145.
[Google Scholar]
-
115.
Tan Y, Xu C, Liu Y, Bai Y, Li X, Wang X. Sprayable
and
self-healing
chitosan-based
hydrogels
for
promoting
healing
of
infected
wound
via
anti-bacteria,
anti-inflammation
and
angiogenesis.
Carbohydr. Polym. 2024,
337, 122147.
[Google Scholar]
-
116.
Chen J, Wang H, Mei L, Wang B, Huang Y, Quan G, et al. A
pirfenidone
loaded
spray
dressing
based
on
lyotropic
liquid
crystals
for
deep
partial
thickness
burn
treatment:
Healing
promotion
and
scar
prophylaxis.
J. Mater. Chem. B 2020,
8, 2573–2588.
[Google Scholar]
-
117.
Yang Y, Suo D, Xu T, Zhao S, Xu X, Bei H-P, et al. Sprayable
biomimetic
double
mask
with
rapid
autophasing
and
hierarchical
programming
for
scarless
wound
healing.
Sci. Adv. 2024,
10, eado9479.
[Google Scholar]
-
118.
Zhong G, Lei P, Guo P, Yang Q, Duan Y, Zhang J, et al. A
Photo-induced
Cross-Linking
Enhanced
A
and
B
Combined
Multi-Functional
Spray
Hydrogel
Instantly
Protects
and
Promotes
of
Irregular
Dynamic
Wound
Healing.
Small 2024,
20, 2309568.
[Google Scholar]
-
119.
Wang R, Yuan C, Cheng J, He X, Ye H, Jian B, et al. Direct
4D
printing
of
ceramics
driven
by
hydrogel
dehydration.
Nat. Commun. 2024,
15, 758.
[Google Scholar]
-
120.
Kuang X, Rong Q, Belal S, Vu T, López López AM, Wang N, et al. Self-enhancing
sono-inks
enable
deep-penetration
acoustic
volumetric
printing.
Science 2023,
382, 1148–1155.
[Google Scholar]
-
121.
Chen Y, Lu W, Zhou Y, Hu Z, Wu H, Gao Q, et al. A
Spatiotemporal
Controllable
Biomimetic
Skin
for
Accelerating
Wound
Repair.
Small 2024,
20, 2310556.
[Google Scholar]
-
122.
Wu SJ, Wu J, Kaser SJ, Roh H, Shiferaw RD, Yuk H, et al. A
3D
printable
tissue
adhesive.
Nat. Commun. 2024,
15, 1215.
[Google Scholar]
-
123.
Zhou T, Yuk H, Hu F, Wu J, Tian F, Roh H, et al. 3D
printable
high-performance
conducting
polymer
hydrogel
for
all-hydrogel
bioelectronic
interfaces.
Nat. Mater. 2023,
22, 895–902.
[Google Scholar]
-
124.
Liu B, Li H, Meng F, Xu Z, Hao L, Yao Y, et al. 4D
printed
hydrogel
scaffold
with
swelling-stiffening
properties
and
programmable
deformation
for
minimally
invasive
implantation.
Nat. Commun. 2024,
15, 1587.
[Google Scholar]
-
125.
Hull SM, Lou J, Lindsay CD, Navarro RS, Cai B, Brunel LG, et al. 3D
bioprinting
of
dynamic
hydrogel
bioinks
enabled
by
small
molecule
modulators.
Sci. Adv. 2023,
9, eade7880.
[Google Scholar]
-
126.
Chen S, Xiong Y, Yang F, Hu Y, Feng J, Zhou F, et al. Approaches
to
scarless
burn
wound
healing:
Application
of
3D
printed
skin
substitutes
with
dual
properties
of
anti-infection
and
balancing
wound
hydration
levels.
eBioMedicine 2024,
106, 105258.
[Google Scholar]
-
127.
Liang J, Zeng H, Qiao L, Jiang H, Ye Q, Wang Z, et al. 3D
Printed
Piezoelectric
Wound
Dressing
with
Dual
Piezoelectric
Response
Models
for
Scar-Prevention
Wound
Healing.
ACS Appl. Mater. Interfaces 2022,
14, 30507–30522.
[Google Scholar]
-
128.
Wu D, Shou X, Yu Y, Wang X, Chen G, Zhao Y, et al. Biologics-Loaded
Photothermally
Dissolvable
Hyaluronic
Acid
Microneedle
Patch
for
Psoriasis
Treatment.
Adv. Funct. Mater. 2022,
32, 2205847.
[Google Scholar]
-
129.
Zhang X, Chen G, Wang Y, Zhao Y. Spatial
tumor
biopsy
with
fluorescence
PCR
microneedle
array.
Innovation 2024,
5, 100538.
[Google Scholar]
-
130.
Kim H, Lee J, Heo U, Jayashankar DK, Agno K-C, Kim Y, et al. Skin
preparation
–free,
stretchable
microneedle
adhesive
patches
for
reliable
electrophysiological
sensing
and
exoskeleton
robot
control.
Sci. Adv. 2024,
10, eadk5260.
[Google Scholar]
-
131.
Samant PP, Niedzwiecki MM, Raviele N, Tran V, Mena-Lapaix J, Walker DI, et al.
Sampling
interstitial
fluid
from
human
skin
using
a
microneedle
patch.
Sci. Transl. Med. 2020,
12, eaaw0285.
[Google Scholar]
-
132.
Li M, Yang L, Wang C, Cui M, Wen Z, Liao Z, et al. Rapid
Induction
of
Long-Lasting
Systemic
and
Mucosal
Immunity
via
Thermostable
Microneedle-Mediated
Chitosan
Oligosaccharide-Encapsulated
DNA
Nanoparticles.
ACS Nano 2023,
17, 24200–24217.
[Google Scholar]
-
133.
Zhang A, Zeng Y, Xiong B, Jiang X, Jin Y, Wang S, et al. A
pH-Responsive
Core-Shell
Microneedle
Patch
with
Self-Monitoring
Capability
for
Local
Long-Lasting
Analgesia.
Adv. Funct. Mater. 2024,
34, 2314048.
[Google Scholar]
-
134.
Shao J, Li X, Li Y, Lin J, Huang P. Self-Heating
Multistage
Microneedle
Patch
for
Topical
Therapy
of
Skin
Cancer.
Adv. Mater. 2024,
36, 2308217.
[Google Scholar]
-
135.
Zhu Z, Wang J, Pei X, Chen J, Wei X, Liu Y, et al. Blue-ringed
octopus-inspired
microneedle
patch
for
robust
tissue
surface
adhesion
and
active
injection
drug
delivery.
Sci. Adv. 2023,
9, eadh2213.
[Google Scholar]
-
136.
Yang Z-R, Suo H, Fan J-W, Lv N, Du K, Ma T, et al. Endogenous
stimuli-responsive
separating
microneedles
to
inhibit
hypertrophic
scar
through
remodeling
the
pathological
microenvironment.
Nat. Commun. 2024,
15, 2038.
[Google Scholar]
-
137.
Zhang Y, Wang S, Yang Y, Zhao S, You J, Wang J, et al. Scarless
wound
healing
programmed
by
core-shell
microneedles.
Nat. Commun. 2023,
14, 3431.
[Google Scholar]
-
138.
Liu H, Qin S, Zhang H, Chen Z, Zhao Y, Liu J, et al. Silk Sericin-based ROS-Responsive Oxygen Generating Microneedle Platform Promotes Angiogenesis and Decreases Inflammation for Scarless Diabetic Wound Healing. Adv. Funct. Mater. 2024, 2404461. doi:10.1002/adfm.202404461.
-
139.
Li C, Yi B, Xu Q, Ma J, Yuan L, Liu Y, et al. ADSCC-CM-Induced
Keratin
Hydrogel-Based
Bioactive
Microneedle
Patch
Containing
Triamcinolone
Acetonide
for
the
Treatment
of
Pathological
Scar.
Adv. Funct. Mater. 2024,
34, 2400457.
[Google Scholar]
-
140.
Liu M, Zhou X, Wang Y, Zhao W, Zhao X, Li L, et al. A Strategy Involving Microporous Microneedles Integrated with CAR-TREM2-Macrophages for Scar Management by Regulating Fibrotic Microenvironment. Adv. Mater. 2024, 2406153. doi:10.1002/adma.202406153.