1. Introduction
Energy drinks (EDs) are beverages that usually contain high levels of caffeine, sugar, and other stimulants such as taurine, guarana, and ginseng [
1]. They are marketed to increase energy and improve performance, particularly during fatigue or stress [
2]. With over 500 brands, they are widely used for several reasons, including improvement of physical activity and endurance, promoting wakefulness, maintaining alertness, and enhancing cognition, mood, and intellectual function [
2,
3]. Energy drinks are popular among athletes, students, and people who work long hours or have a demanding lifestyle [
4,
5]. Athletes in gyms often use these drinks, and students in schools, clubs, bars, and restaurants [
6]. While energy drinks may offer a short-term energy stimulation, some potential risks are associated with excessive or regular consumption [
1]. These risks include (i) caffeine overdose, which can cause heart palpitations, nausea, vomiting, tremors, and heightened anxiety [
7], (ii) dehydration due to their diuretic effect, potentially causing headaches, fatigue, dizziness, and dry mouth [
8], (iii) sleep disturbance, such as insomnia or reduced sleep quality and duration [
8,
9], (iv) cardiovascular effects, including increased heart rate and blood pressure [
10] and (v) addiction or dependence on caffeine and other stimulants, where habitual use may result in caffeine addiction and withdrawal symptoms like irritability, headaches, and impaired concentration [
11]. Additionally, the high sugar content of many energy drinks can contribute to an increased risk of metabolic disturbances, including obesity [
12], insulin resistance, and type 2 diabetes [
13]. Frequent ED consumption has also been associated with poor dental health, particularly due to their acidity and sugar concentration, which can promote tooth erosion and cavities [
14]. From a neurological perspective, EDs may exacerbate anxiety and panic disorders and have been linked to symptoms of agitation, restlessness, and, in some cases, seizures in young individuals, especially when consumed in combination with alcohol or other stimulants [
15,
16].
Despite the recommendation of the American Academy of Pediatrics that children and adolescents should avoid EDs, as the potential risks may outweigh any potential benefits [
17], reports showed high ED use among them [
18]. Since adolescents need more sleep than adults, consuming EDs can interfere with healthy sleeping hours and quality [
19], leading to fatigue and difficulty concentrating during the day. Furthermore, adolescents are more susceptible to developing an addiction than adults and consuming energy drinks regularly may lead to dependence on caffeine and other stimulants. Numerous research have delved into the prevalence of energy drink consumption among adolescents [
18,
20,
21], consistently highlighting a significant proportion of young individuals openly acknowledging their use of these beverages. Furthermore, investigations have sought to elucidate the intricate link between energy drink consumption and risky behaviors in adolescents [
22,
23], leading to poor academic performance, depressive symptoms, increased risk-taking behaviors, and co-use of substances like tobacco, alcohol, or cannabis.
While not explicitly classified within the domain of a substance use disorder, empirical observations indicate that certain adolescents can exhibit behavioural patterns reminiscent of addiction to energy drinks [
24]. This is discernible through the manifestation of compulsive and problematic consumption, resulting in an inability to curtail intake despite encountering adverse consequences [
23]. Notably, individuals engaging in regular consumption of energy drinks, particularly those containing high levels of caffeine, may grapple with withdrawal symptoms like headaches, fatigue, irritability, and difficulty concentrating when attempting to reduce or cease their consumption [
25].
The intricate web of factors contributing to the problematic consumption of energy drinks among adolescents involves interconnected elements. Peer influence emerges as a pivotal determinant, with adolescents frequently swayed by the behaviours exhibited by their peers [
26]. Additionally, the impact of marketing strategies employed by energy drink companies, coupled with the widespread accessibility of these beverages and the prevailing perception that consumption enhances social status or performance, collectively contributes to the intricate landscape of energy drink-related issues within this demographic [
27,
28]. Comprehending these multifaceted factors is paramount for developing effective interventions and strategies to mitigate potential risks associated with energy drink consumption among adolescents. ED consumption in Lebanon is common among the youth [
24]. Although the Lebanese Ministries of Economy and Health had issued back in 2012 a policy obliging ED importers and producers to lower the caffeine level from 65 to 35 g, follow-up and control of this law were scarce, given that some marketed products contain up to 80 mg of caffeine [
29]. A pilot cross-sectional study tackling ED consumption prevalence was previously conducted in the capital Beirut and showed an overall prevalence of 63.6% among those aged between 13 and 30 [
26]. Nevertheless, little information exists about this consumption and the factors impacting ED use and adolescents’ addiction. Therefore, the primary objective of this study is to determine the prevalence of ED consumption among adolescents in Lebanon and to assess the predictors of ED use and addiction.
Three hypotheses were formulated: (1) A significant proportion of Lebanese adolescents consume energy drinks, despite known health risks. (2) ED consumption and dependence are associated with sociodemographic characteristics (e.g., age, gender), or behavioral factors (e.g., peer influence, physical activity). (3) Adolescents who consume EDs more frequently are more likely to exhibit signs of problematic or dependent use.
2. Materials and Methods
2.1. Study Design
An observational multi-center cross-sectional study was performed over eight months during the 2022/2023 academic year, targeting adolescents from 12 schools in Lebanon.
2.2. Study Sample and Sample Size
Participants were recruited without selection criteria based on sex, nationality, or ethnicity. The sample included adolescents between 13 and 18 years old attending the selected schools from grades 9 to 12. Those who refused to answer or deliver the survey were excluded. The sample size was determined using the Epi Info 7 software version 7.2.4.0. The calculation assumed that the probability of consumption of EDs was 63.6% based on findings from a previous pilot study conducted in Lebanon among both college and university students [
26]. A 95% confidence interval and a 5% acceptable margin of error were considered. We assumed a design effect of 5 to assess the variance of the sample estimate obtained from the variance of a simple random sample estimate of the same size. This yielded 1778 participants. Considering the values of skewness (0.117) and kurtosis (0.227), data were normally distributed and converged toward their expected values [
30]. Thirty potential private schools were contacted, of which only 12 agreed to take part in the study after reviewing the survey and protocol. The selected schools were in three governorates: 4 in Beirut, 4 in Mount Lebanon, and 4 in the South. Despite being representative of adolescents in Lebanon, schools from other governorates did not agree to participate, and therefore, differences may arise.
2.3. Data Collection
Depending on the school’s direction time preference, six pharmacists approached the students in classes from 8 a.m. to 2 p.m. on weekdays and explained the study objectives orally. They invited them to participate by filling out a printed survey. The first page included a written version of the objectives, and a consent form, with an estimated 20 min to answer.
2.4. Study Tool
After an extensive literature review, a questionnaire was developed and used for data collection. It was available in Arabic (the official language in Lebanon). It was initially piloted on 50 participants, and questions that needed more clarity were adjusted or deleted. To ensure content validity, the questionnaire was reviewed by a panel of public health and behavioral science experts and was afterward reviewed by two external reviewers to confirm that items were appropriate, relevant, and comprehensive. The internal consistency and reliability of the instrument were assessed using Cronbach’s alpha during the pilot, with acceptable results across key domains (alpha values of 0.821).
The first part included questions about the participants’ general characteristics, including sex, age, height, and weight, the location of the school (urban or rural area), and the school grade. This part also collected the lifestyle habits and sports practices of the sample, such as smoking (cigarettes, waterpipe, and passive smoking), alcohol consumption, comorbidities, physical activity, and its location (indoors, outdoors, at a gym or schools), and if they had a workout partner. The second part of the survey comprised questions related to ED consumption and dependence. Participants were also asked about the role of EDs (multiple answers were possible). These roles included physical power, stimulating awakeness, sports drinks, and improving mental activity. They were also asked if they consumed EDs in the last 12 months, the age of initial consumption, the average number of EDs per time, the frequency of consumption (daily, weekly, monthly, and rarely), and the monthly amount spent on EDs (in Lebanese pounds and was later transformed into United States Dollars (USD) based on the daily rate). Moreover, students reported having family members that consumed EDs, the place to drink them (clubs/restaurants, home or school), the time of consumption (at night, on special occasions, no specific time, before physical activity and during exams) and the reasons for ED consumption. They reported whether or not they mix EDs with alcohol or caffeinated beverages and their perceived dependence on EDs and overall satisfaction. The 5-item Alcohol Use Disorders Identification Test was used to assess dependence while replacing alcohol with ED. The questions covered included the frequency of drinking, the quantity of EDs consumed on a typical day, and the occurrence of binge drinking episodes. The test was scored on a scale of 0 to 12, with 4 or more for men and 3 or more for women used as cut-off points for dependence [
31].
2.5. Statistical Analysis
Statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) Version 28. Categorical variables were presented through frequencies and percentages; For continuous variables, including current age, Body Mass Index (BMI), age of energy drink initiation, and the number of cans consumed each time, means and standard deviations were reported.
To explore associations between ED use or dependence and participants’ sociodemographic characteristics and consumption behaviors, bivariate analyses were performed. Chi-square or Fisher’s exact tests were applied for categorical comparisons, while the unpaired Student’s t-test or Mann-Whitney U test was used for continuous data, depending on distribution.
Multivariate logistic regression models were used to identify predictors of ED consumption and dependence. Results are presented as Odds Ratios (ORs) with corresponding 95% Confidence Intervals (CIs). Only variables showing statistical significance in the bivariate analyses were included in the multivariate models. A p-value less than 0.05 was considered indicative of statistical significance.
2.6. Ethical Considerations
The study protocol, including the survey instrument and consent form, received approval from the institutional review board of the faculty of pharmacy at the Lebanese University on 2 May 2019 (Reference: 4/23/D). Participation was voluntary, and all data collected were kept strictly anonymous and non-identifiable.
Written informed consent was first obtained from each participant’s parent/legal guardian. Adolescents with parental approval were then invited to provide their own written consent before completing the questionnaire. Participants were assured that they could discontinue their involvement at any time. All collected information was used exclusively for research purposes.
3. Results
3.1. General Characteristics of the Participants
Overall, 1911 potential participants were approached, and 1855 agreed to participate in the study (97.0%). The general characteristics of the study participants are presented in . The sample comprised slightly more males (53.5%) than females (46.5%). The mean age of the students was 16.3 (1.3) years. Around 55% of schools were in urban areas, and 45.4% were in rural areas. As regards smoking status, 30.9% were current smokers, of which 11.1% were cigarette smokers, 62.1% were waterpipe smokers, and the rest (26.5%) smoked both. Only 3.5% of the sample reported having existing comorbidities, and 22.2% were alcohol consumers. Most participants (83.2%) practiced physical activity in locations: 40.3% indoors, 33.4% outdoors, 19.1% in a gym, and 7.2% at schools. Sixty-five percent of those who practiced sports reported having an exercise partner.
.
Distribution of the general characteristics of the adolescents.
| Total (N = 1855) |
|
Frequency (%) |
| Sex |
Male |
993 (53.5%) |
| Female |
862 (46.5%) |
| Age (years) |
Mean (SD) |
16.3 (1.3) |
| BMI (Kg/m2) |
Mean (SD) |
21.7 (3.7) |
| Location of the school |
Urban area |
1013 (54.6%) |
| Rural area |
842 (45.4%) |
| The school grade |
Grade 9 |
187 (12.9%) |
| Grade 10 |
506 (27.3%) |
| Grade 11 |
525 (28.3%) |
| Grade 12 |
585 (31.5%) |
| Monthly allowance (USD) |
<100 USD |
975 (52.5%) |
| 100–300 USD |
736 (39.7%) |
| >300 USD |
144 (7.8%) |
| Smoking status |
Smoker |
574 (30.9%) |
| Non-smoker |
1281 (69.1%) |
| Type of smoking (N = 574) |
Cigarettes |
64 (11.1%) |
| Waterpipe |
357 (62.1%) |
| Shisha and waterpipe |
153 (26.5%) |
| Passive smoking |
Yes |
789 (42.5%) |
| No |
1066 (57.5%) |
| Comorbidities |
Yes |
64 (3.5%) |
| No |
1791 (96.5%) |
| Alcohol consumption |
Yes |
411 (22.2%) |
| No |
1444 (77.8%) |
| Physical activity |
Yes |
1543 (83.2%) |
| No |
312 (16.8%) |
| Location of physical activity (N = 1543) |
Indoors (at home) |
623 (40.3%) |
| Outdoors |
515 (33.4%) |
| Gym |
294 (19.1%) |
| School |
111 (7.2%) |
| Exercise partners (N = 1543) |
Yes |
1003 (65.0%) |
| No |
540 (35.0%) |
3.2. Prevalence and Characteristics of Energy Drink Consumption
presents the prevalence of energy drink use among school students and its characteristics. When asked to choose which applies most to the role of EDs, 66.4% reported that they give physical power, 50.8% said they stimulate awakeness, 18.3% defined them as sports drinks, and only 7.1% reported that they improve mental activity. Overall, 55.5% of the sample used EDs during the past 12 months, with a mean age of initial consumption of 13.7 years, with 9.2% consuming them daily and around 21% consuming them weekly or monthly, respectively. Most students (71.9%) spent less than 7 USD per month on EDs, which they frequently consumed in clubs or restaurants (78.8%) and at home (55.6%). This consumption was reported more at night (43.3%), mainly to stimulate awakeness (54.3%) or as energy boosters (39.9%). Around 35% of the participants reported mixing EDs with alcohol, and 25.3% mixed them with other caffeinated beverages. Regarding dependence on EDs, 14.5% of the students reported being dependent on ED consumption.
.
Prevalence and characteristics of energy drink consumption among adolescents.
| Total (N = 1855) |
|
Frequency (%) |
| Energy drink definition |
Give physical power |
1232 (66.4%) |
| Stimulate awakeness |
943 (50.8%) |
| Sport drink |
339 (18.3%) |
| Improve mental activity |
132 (7.1%) |
| Energy drink consumption during the past 12 months |
Yes |
1029 (55.5%) |
| No |
826 (44.5%) |
| Age of initial energy drink consumption (years) |
Mean (SD) |
13.7 (1.7) |
| The average number of energy drinks per time |
Mean (SD) |
1.4 (0.7) |
Frequency of energy drink consumption
(N = 1029)
|
Daily |
95 (9.2%) |
| Weekly |
219 (21.3%) |
| Monthly |
223 (21.7%) |
| Rarely |
492 (47.8%) |
Monthly amount spent on energy drinks (USD)
(N = 1029)
|
<7 USD |
740 (71.9%) |
| 7–20 USD |
220 (21.4%) |
| >20 USD |
69 (6.7%) |
Family members consuming energy drinks
(N = 640/1029)
|
Siblings |
397 (38.6%) |
| Father |
156 (15.2%) |
| Mother |
87 (8.5%) |
The place for energy drink consumption
(N = 1029)
|
Clubs/Restaurants |
811 (78.8%) |
| Home |
572 (55.6%) |
| School |
76 (7.4%) |
The common time for energy drink consumption
(N = 1029)
|
Late at night |
445 (43.2%) |
| On special occasions |
270 (26.2%) |
| No specific time |
253 (24.6%) |
| Before physical activity |
241 (23.4%) |
| During exams |
160 (15.5%) |
Reason for energy drink consumption
(N = 1029)
|
Stimulate awakeness |
559 (54.3%) |
| Energy booster |
411 (39.9%) |
| Enhance moral state |
262 (25.5%) |
| Taste/preference |
215 (20.9%) |
| Improve confidence |
49 (4.8%) |
| Mixing energy drinks with alcohol (N = 1029) |
Yes |
357 (34.7%) |
| No |
672 (65.3%) |
| Mixing energy drinks with caffeinated drinks (N = 1029) |
Yes |
260 (25.3%) |
| No |
769 (74.7%) |
| Dependence on energy drinks (N = 1029) |
Yes |
149 (14.5%) |
| No |
880 (85.5%) |
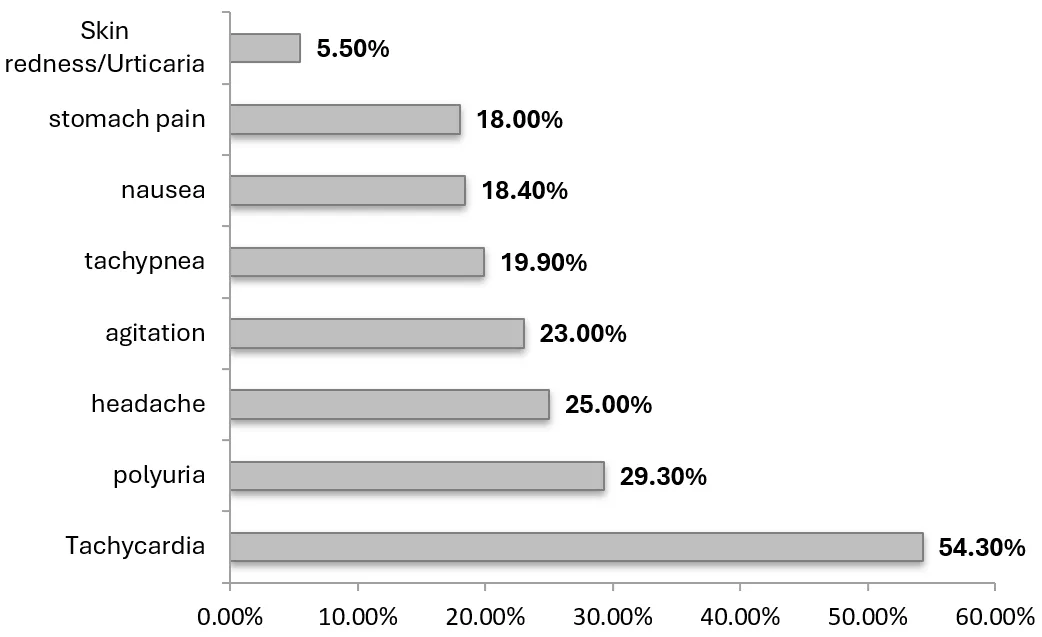
When asked if EDs have side effects, around half of the participants (51.2%) agreed, 11.1% said that EDs have no side effects and the rest (37.7%) answered with “I do not know”. Among those who responded positively, more than half (54.3%) reported tachycardia as a side effect, followed by polyuria (29.3%), headaches (25.0%), and agitation (23.0%). The least reported side effects were skin redness or urticaria (5.5%), stomach pain (18.0%), and nausea (18.4%) (
).
. Energy drinks side effects (N = 949).
shows the association between ED use and dependence on the general characteristics of adolescents and the patterns of ED consumption. Significantly more males (65.0%) used EDs than females (44.5%;
p < 0.001). Students in grades 10 (46.8%) and 11 (55.4%) significantly consumed EDs more than those in grades 9 (32.3%) and 12 (33.9%;
p = 0.039). The increase in monthly allowance significantly increased the use of EDs, where 66.7% of those receiving more than 300 USD used EDs compared to 49.1% of students receiving less than 100 USD per month (
p < 0.001). Smoking and alcohol consumption were found to be associated with ED use, where 70.5% of cigarette smokers, 74.3% of waterpipe smokers, and 80.3% of alcohol consumers reported that they use EDs compared to significantly lower percentages among non-users (
p < 0.001). Around 60.0% of students reported using EDs to stimulate awakeness compared to 50.3% of those who did not (
p < 0.001), and 65.6% of students reporting that EDs were sports drinks were actual users compared to 53.2% of those who did not (
p < 0.001). Furthermore, perceiving that EDs had no side effects (75.7%) was associated with their use (
p < 0.001). Regarding the patterns associated with ED dependence, 69.5% of students consuming EDs daily reported dependence compared to significantly lower percentages of those consuming them less frequently (
p < 0.001). Around half of those spending more than 20 USD per month on EDs reported being dependent, compared to only 5.4% of those spending less than 7 USD (
p < 0.001). Moreover, students consuming EDs before physical activity or during the exam period reported higher dependence on EDs than others (
p < 0.001). Dependence was significantly reported among 18.5% of those mixing EDs with alcohol and 28.8% of those mixing them with other caffeinated beverages than others (
p = 0.008 and
p < 0.001, respectively). The reasons for ED use were significantly associated with dependence, where 46.8% of students consumed them to increase self-confidence, 20.4% of those used them for physical power, and 26% of those who consumed EDs to enhance their moral state reported dependence significantly more than others (
p < 0.001). In addition, students reporting satisfaction with EDs had a higher association with dependence than others (
p < 0.001).
.
Association between energy drink use and dependence on the general characteristics of the students and patterns of energy drink consumption.
|
ED Users |
Non-Users |
|
|
Frequency (%) |
Frequency (%) |
p-value |
| Age (years) |
Mean (SD) |
16.4 (1.3) |
16.2 (1.2) |
0.847 |
| Sex |
Male |
645 (65.0%) |
348 (35.0%) |
<0.001 |
| Female |
384 (44.5%) |
478 (55.5%) |
| Location of the school |
Urban area |
537 (53.0%) |
476 (47.0%) |
0.019 |
| Rural area |
492 (58.4%) |
350 (41.6%) |
| The school grade |
Grade 9 |
38 (32.2%) |
80 (67.8%) |
0.039 |
| Grade 10 |
72 (46.8%) |
82 (53.2%) |
| Grade 11 |
160 (55.4%) |
129 (44.6%) |
| Grade 12 |
65 (33.9%) |
127 (66.1%) |
| Monthly allowance (USD) |
<100 USD |
479 (49.1%) |
496 (50.9%) |
|
| 100–300 USD |
454 (61.7%) |
282 (38.3%) |
<0.001 |
| >300 USD |
96 (66.7%) |
48 (33.3%) |
|
| Cigarette smoking |
Yes |
153 (70.5%) |
64 (29.5%) |
<0.001 |
| No |
876 (53.5%) |
762 (46.5%) |
| Waterpipe smoking |
Yes |
379 (74.3%) |
131 (25.7%) |
<0.001 |
| No |
650 (48.3%) |
695 (51.7%) |
| Alcohol consumption |
Yes |
330 (80.3%) |
81 (19.7%) |
<0.001 |
| No |
699 (48.4%) |
745 (51.6%) |
| EDs stimulate awakeness |
Yes |
570 (60.4%) |
373 (39.6%) |
<0.001 |
| No |
459 (50.3%) |
453 (49.7%) |
| EDs give physical power |
Yes |
712 (57.8%) |
520 (42.2%) |
0.005 |
| No |
317 (50.9%) |
306 (49.1%) |
| EDs are sports drinks |
Yes |
223 (65.6%) |
117 (34.4%) |
<0.001 |
| No |
806 (53.2%) |
709 (46.8%) |
| EDs have side effects |
Yes |
503 (53.0%) |
446 (47.0%) |
<0.001 |
| No |
156 (75.7%) |
50 (24.3%) |
|
ED dependents |
Non-dependents |
|
|
Frequency (%) |
Frequency (%) |
p-value |
| Frequency of ED consumption |
Daily |
66 (69.5%) |
29 (30.5%) |
|
| Weekly |
45 (20.5%) |
174 (79.5%) |
<0.001 |
| Monthly |
24 (10.8%) |
199 (89.2%) |
| Rarely |
14 (2.8%) |
478 (97.2%) |
| Monthly amount spent on EDs |
<7 USD |
40 (5.4%) |
700 (94.6%) |
<0.001 |
| 7–20 USD |
72 (32.7%) |
148 (67.3%) |
| >20 USD |
37 (53.6%) |
32 (46.4%) |
| ED consumption before physical activity |
Yes |
53 (22.1%) |
187 (77.9%) |
<0.001 |
| No |
95 (12.1%) |
693 (87.9%) |
| ED consumption during exams |
Yes |
37 (23.1%) |
123 (76.9%) |
0.001 |
| No |
112 (12.9%) |
757 (87.1%) |
| Mixing EDs with alcohol |
Yes |
66 (18.5%) |
291 (81.5%) |
0.008 |
| No |
83 (12.4%) |
589 (87.6%) |
| Mixing EDs with caffeinated drinks |
Yes |
75 (28.8%) |
695 (90.4%) |
<0.001 |
| No |
74 (9.6%) |
185 (71.2%) |
| EDs improve confidence |
Yes |
23 (46.9%) |
26 (53.1%) |
<0.001 |
| No |
126 (12.9%) |
854 (87.1%) |
| EDs give physical power |
Yes |
84 (20.4%) |
327 (79.6%) |
0.001 |
| No |
65 (10.5%) |
553 (89.5%) |
| EDs enhance moral state |
Yes |
68 (26.0%) |
194 (74.0%) |
<0.001 |
| No |
81 (10.6%) |
686 (89.4%) |
| Satisfaction with EDs |
Yes |
123 (19.8%) |
497(80.2%) |
<0.001 |
| No |
26 (6.4%) |
383 (93.6%) |
3.4. Predictors of Ed Use and Dependence among Adolescents
The combined effect of the predictors of ED use and dependence is presented in
. After adjusting for covariates, the odds of ED use were 3.63 times higher among alcohol consumers than others (OR 3.63, 95% CI 2.75–4.79) and 2.67 times higher among adolescents who smoked waterpipe (OR 2.67, 95% CI 2.10–3.39). Students perceiving them as sports drinks had 1.97-fold higher odds of ED use than others (OR 1.97, 95% CI 1.47–2.64), and those who reported that EDs give physical power had 1.69-fold higher odds of their use than others (OR 1.69, 95% CI 1.34–2.14). These odds were also significantly higher among those receiving a monthly allowance ≥100 USD than adolescents receiving lower amounts (OR 1.25, 95% CI 1.06–1.47). In contrast, the odds of ED use were 24% lower among adolescents acknowledging that EDs have side effects than others (OR 0.76, 95% CI 0.65–0.89), with females having 53% lower odds than males (aOR 0.47, 95% CI 0.39–0.58). As regards the patterns predicting the dependence on EDs among adolescents, participants consuming EDs daily or weekly had 2.62 times higher odds of dependence than those using them less frequently (OR 2.62, 95% CI 2.00–3.42), and students reporting satisfaction with EDs had significantly higher odds of dependence than others (OR 2.41, 95% CI 1.42–4.11). These odds were 2.33 times higher among adolescents drinking EDs before physical activity (OR 2.33, 95% CI 1.75–4.27), 2.25 times higher among those using them to improve confidence (OR 2.25, 95% CI 1.02–4.99), and 2.17 times among participants consuming EDs to enhance their moral state (OR 2.17, 95% CI 1.05–2.59) than others. Adolescents spending more than 7 USD on EDs had 1.72-fold higher odds of dependence than others (OR 1.72, 95% CI 1.19–2.49).
.
Predictors of ED use and dependence among adolescents in schools.
| Energy Drink Use |
| Adjusted model |
|
aOR [95% CI] |
p-value |
| Alcohol consumption (No as a reference) |
3.63 [2.75–4.79] |
<0.001 |
| Waterpipe smoking (No as a reference) |
2.67 [2.10–3.39] |
<0.001 |
| EDs are sports drinks (No as a reference) |
1.97 [1.47–2.64] |
<0.001 |
| EDs give physical power (No as a reference) |
1.69 [1.34–2.14] |
<0.001 |
| Monthly allowance (<100 USD as a reference) |
|
|
| ≥100 USD |
1.25 [1.06–1.47] |
0.008 |
| EDs have side effects (No as a reference) |
0.76 [0.65–0.89] |
0.001 |
| Female sex (Male as a reference) |
0.47 [0.39–0.58] |
<0.001 |
| Energy drink dependence |
| Adjusted model |
|
aOR [95% CI] |
p-value |
| Daily/Weekly consumption (Monthly/rarely as a reference) |
2.62 [2.00–3.42] |
<0.001 |
| Satisfaction with ED consumption (No as a reference) |
2.41 [1.42–4.11] |
0.001 |
| ED consumption before physical activity (No as a reference) |
2.33 [1.75–4.27] |
0.032 |
| ED consumption to improve confidence (No as a reference) |
2.25 [1.02–4.99] |
0.041 |
| ED consumption to enhance moral state (No as a reference) |
2.17 [1.05–2.59] |
0.029 |
| Higher spending on ED (<7 USD as a reference) |
1.72 [1.19–2.49] |
0.004 |
| Number of cans consumed (per increase of one unit) |
1.32 [1.03–1.76] |
0.046 |
4. Discussion
This multi-center cross-sectional study aimed to determine the prevalence and patterns of ED consumption among adolescents and assess the predictors of ED use and addiction. Based on findings from the present study, the prevalence of ED consumption is high among the study sample (adolescents between 13 and 18 years) during the past year, but slightly lower than the one found in the previously conducted pilot study among youths between 13 and 30 years of age, and reporting lifetime consumption (63.6%) [
26]. This prevalence (55.5%) is comparable to another study conducted among high school students in Canada (62.0%) also assessing ED use over one-year period [
32], and another among German investigating adolescents’ lifetime use (61.7%) [
33]. A recently published systematic review showed that ED use at an early age increased the risk of substance use or risky behaviors later in life [
23], which emphasizes the need for early interventions and policy implementation to prevent such long-term harm, particularly in a low-income country like Lebanon. Males significantly used EDs more than females, which agrees with the existing literature [
34,
35]. This variation may be attributable to the advertisements in which ED consumers are mainly males who use them to boost their confidence and improve their social lives [
6,
36].
Around half of the sample reported that EDs have side effects, of which tachycardia, polyuria, headache, and agitation were more common. Research highlighted these side effects that are significantly associated with the frequency and quantity consumed [
37,
38]. These adverse events were rising with the increasing monthly budget spent on EDs, possibly correlated with the higher exposure to caffeine since the corresponding side effects were found to be directly associated with the dose of caffeine consumed [
39]. Despite the knowledge of the adverse outcomes of ED consumption, more than half of the students consumed them. The main reasons for ED use were to stimulate awakeness and gain physical power, which can explain the timing of ED consumption that was mainly during late nights. Such findings are concomitant with previous research in which ED users reported consuming them to stay awake and increase energy in parties [
40,
41]. Reports also showed associated behaviors with ED use, including smoking, and mixing them with alcohol or caffeinated beverages [
40,
42]. Consumers tended to mix EDs with alcohol, assuming to counteract the depressant effects of alcohol and thereby decrease hangover [
8]. These practices, in addition to the relatively low price of cigarettes and alcohol in Lebanon and the absence of age restriction regarding their acquisition [
43], can explain the higher ED use among cigarette and waterpipe smokers and alcohol consumers, which increased 2–3 folds the odds of ED use. Despite laws and regulations in place to prevent such activities, enforcement can sometimes be challenging, namely due to social pressures and norms deeming them acceptable. Communities, law enforcement, and regulators must collaborate, enforcing stricter penalties for supplying minors with tobacco and alcohol, enhancing ID verification, and raising awareness of the risks. Around 15% of the sample reported being dependent on EDs. This dependence was found to be associated with a higher susceptibility to other substance abuse or dependence [
42,
44]. Students used EDs to stimulate awakeness, enhance their morale, and boost their energy. A recent study found that low health-related quality of life among students [
45], expected to be exacerbated during the pandemic and the economic crisis in Lebanon [
46], which could be a coping mechanism to overcome this state.
This study has limitations. Despite considering the effect size in the sample size calculation, the included students were from private schools since no permission was obtained to enter public schools. Therefore, possible differences might exist between schools. The invited schools were distributed in urban and rural areas in the different governorates in Lebanon. Nevertheless, those who accepted to participate were from three main governorates. Findings from this study may differ compared to excluded adolescents (18–19 years) since easier access to alcohol and cigarettes may induce additional ED consumption. Recall bias can affect the findings since a self-reported survey was used for data collection. However, data collectors were uniformly trained and used the same form, and a different researcher performed data coding and analysis. While this study explored several sociodemographic and behavioral characteristics associated with ED consumption and dependence among adolescents, certain important dimensions were not assessed. Specifically, psychological and personality-related factors, such as sensation seeking, impulsivity, susceptibility to peer pressure, and attitudes toward marketing, were not included in the analysis due to the scope and design of the original questionnaire. These psychosocial determinants are known to influence substance-related behaviors and could further explain the motivations behind problematic energy drink use. Future research should incorporate validated psychological scales to better understand how individual personality traits and cognitive drivers interact with environmental and social influences to shape consumption patterns. Including these dimensions would provide a more holistic view and strengthen the design of targeted interventions and policy measures. The present study is among the few multi-center studies tackling the prevalence and patterns of ED consumption among adolescents and the predictors of this consumption and possible dependence. Findings can allow better-informed decisions and tailored campaigns targeting this specific group in Lebanon and other similar settings worldwide.
5. Conclusions and Implications for Practice
A high prevalence of ED consumption was found among adolescents between 13 and 18 years, mainly males. ED use and dependence were associated with various lifestyles and misconceptions of EDs. The combined predictors of ED use and dependence should be considered to reduce the harm associated with uncontrolled consumption, which may lead to substance abuse at an older age. Interventions encouraging healthy alternatives are recommended, such as drinking water or natural juices instead of EDs or participating in physical activities that can boost their energy levels naturally.
The findings of this study have important implications for both public health practice and policymaking. Given the high prevalence of ED consumption and signs of dependence among adolescents, there is an urgent need to implement targeted educational programs in schools that raise awareness about the potential health risks associated with ED use, particularly those related to cardiovascular, neurological, and behavioral consequences. Health professionals, educators, and parents should be equipped with evidence-based resources to guide youth toward healthier choices. At the policy level, regulatory measures such as age restrictions for ED purchases, clearer labeling of caffeine and sugar content, restrictions on marketing directed at adolescents, and enforcement of existing caffeine content limits are crucial steps. Collaboration between the ministries of health, education, and youth affairs is essential to develop and enforce effective strategies that reduce access and appeal of EDs to minors, while promoting a culture of health and informed decision-making among the younger population.
Author Contributions
Conceptualization, S.M., M.C., S.A. and S.R.; Methodology, G.H., M.E.-H., S.A. and S.R.; Software, S.M. and G.H.; Validation, M.C., S.A. and S.R.; Formal Analysis, S.M., G.H., A.M. and M.E.-H.; Investigation, S.M., M.E.-H., F.B., A.M. and S.R.; Resources, S.M., M.C., A.M., M.E.-H. and F.B.; Data Curation, S.M. and G.H.; Writing—Original Draft Preparation, S.M., G.H., M.C., S.A., M.E.-H., A.M. and F.B.; Writing—Review & Editing, G.H., M.C., S.A. and S.R.; Visualization, G.H., A.M. and S.R.; Supervision, M.C. and S.R.; Project Administration, S.M., A.M., F.B. and S.R.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Faculty of Pharmacy at the Lebanese University on 2 May 2019 (Reference: 4/23/D). Participation was voluntary, and all data collected were kept strictly anonymous and non-identifiable.
Informed Consent Statement
Written informed consent was first obtained from each participant’s parent/legal guardian.
Data Availability Statement
Data are provided at a reasonable request from the corresponding author after approval of the scientific committee of the Lebanese University.
Funding
This research received no external funding.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
1.
Ariffin H, Chong XQ, Chong PN, Okechukwu PN. Is the consumption of energy drink beneficial or detrimental to health: a comprehensive review?
Bull. Natl. Res. Cent. 2022,
46, 163.
[Google Scholar]
-
2.
Chtourou H, Trabelsi K, Ammar A, Shephard RJ, Bragazzi NL. Acute effects of an “Energy drink” on short-term maximal performance, reaction times, psychological and physiological parameters: insights from a randomized double-blind, placebo-controlled, counterbalanced crossover trial.
Nutrients 2019,
11, 992.
[Google Scholar]
-
3.
Jagim AR, Harty PS, Tinsley GM, Kerksick CM, Gonzalez AM, Kreider RB, et al. International society of sports nutrition position stand: energy drinks and energy shots.
J. Int. Soc. Sports Nutr. 2023,
20, 2171314.
[Google Scholar]
-
4.
Simulescu V, Ilia G, Macarie L, Merghes P. Sport and energy drinks consumption before, during and after training.
Sci. Sports 2019,
34, 3–9.
[Google Scholar]
-
5.
Sampasa-Kanyinga H, Masengo L, Hamilton HA, Chaput JP. Energy drink consumption and substance use among middle and high school students.
Int. J. Environ. Res. Public Health 2020,
17, 3110.
[Google Scholar]
-
6.
Ghozayel M, Ghaddar A, Farhat G, Nasreddine L, Kara J, Jomaa L. Energy drinks consumption and perceptions among University Students in Beirut, Lebanon: A mixed methods approach.
PloS ONE 2020,
15, e0232199.
[Google Scholar]
-
7.
Gashkarimov V, Uritsky B, Tukhvatullina D, Efremov I, Asadullin A. Relationship between frequency of energy drink consumption and insomnia, depression, alcohol abuse, socioeconomic status, and religion among students in the Republic of Bashkortostan.
Adiktologie 2021,
21, 7–15.
[Google Scholar]
-
8.
Nadeem IM, Shanmugaraj A, Sakha S, Horner NS, Ayeni OR, Khan M. Energy drinks and their adverse health effects: A systematic review and meta-analysis.
Sports Health 2021,
13, 265–277.
[Google Scholar]
-
9.
Trapp GS, Hurworth M, Jacoby P, Maddison K, Allen K, Martin K, et al. Energy drink intake is associated with insomnia and decreased daytime functioning in young adult females.
Public Health Nutr. 2021,
24, 1328–1337.
[Google Scholar]
-
10.
Grinberg N, Benkhedda K, Barber J, Krahn AD, La Vieille S. Effects of caffeinated energy drinks on cardiovascular responses during exercise in healthy adults: A systematic review and meta-analysis of randomized controlled trials.
Appl. Physiol. Nutr. Metab. 2022,
47, 618–631.
[Google Scholar]
-
11.
Bae EJ, Kim EB, Choi BR, Won SH, Kim JH, Kim SM, et al. The relationships between addiction to highly caffeinated drinks, burnout, and attention-deficit/hyperactivity disorder.
J. Korean Acad. Child Adolesc. Psychiatry 2019,
30, 153.
[Google Scholar]
-
12.
Marks R. Energy drinks, A potentially overlooked obesity correlate.
Adv. Obes. Weight Manag. Control 2015,
2, 00019. doi:10.15406/ aowmc.2015.02.00019.
[Google Scholar]
-
13.
Trapp G, Hurworth M, Jacoby P, Christian H, Ambrosini G, Oddy W, et al. Energy drink intake and metabolic syndrome: A prospective investigation in young adults
. Nutr. Metab. Cardiovasc. Dis. 2020,
30, 1679–1684.
[Google Scholar]
-
14.
Karimi M. Why Drinking Carbonated Beverages and Energy Drinks are Detrimental to Children’s Oral Health?
EC Paediatr. 2019,
8, 537–543.
[Google Scholar]
-
15.
Kaur S, Christian H, Cooper MN, Francis J, Allen K, Trapp G. Consumption of energy drinks is associated with depression, anxiety, and stress in young adult males, Evidence from a longitudinal cohort study.
Depress. Anxiety 2020,
37, 1089–1098.
[Google Scholar]
-
16.
Lee JH, Lee JH, Choi YJ, Kim YJ. Effects of Long-and Short-term Consumption of Energy Drinks on Anxiety-like, Depression-like, and Cognitive Behavior in Adolescent Rats.
J. Korean Biol. Nurs. Sci. 2020,
22, 111–118.
[Google Scholar]
-
17.
Temple JL. Trends, safety, and recommendations for caffeine use in children and adolescents.
J. Am. Acad. Child Adolesc. Psychiatry 2019,
58, 36–45.
[Google Scholar]
-
18.
Vercammen KA, Koma JW, Bleich SN. Trends in energy drink consumption among US adolescents and adults, 2003–2016.
Am. J. Prev. Med. 2019,
56, 827–833.
[Google Scholar]
-
19.
Gariépy G, Doré I, Whitehead RD, Elgar FJ. More than just sleeping in, a late timing of sleep is associated with health problems and unhealthy behaviours in adolescents.
Sleep Med. 2019,
56, 66–72.
[Google Scholar]
-
20.
Brunborg GS, Raninen J, Andreas JB. Energy drinks and alcohol use among adolescents: A longitudinal study.
Drug Alcohol Depend. 2022,
241, 109666.
[Google Scholar]
-
21.
Kaldenbach S, Strand TA, Holten-Andersen MN. Experiences with energy drink consumption among Norwegian adolescents.
J. Nutr. Sci. 2023, 12, e30.
[Google Scholar]
-
22.
Puupponen M, Tynjälä J, Välimaa R, Paakkari L. Associations between adolescents’ energy drink consumption frequency and several negative health indicators.
BMC Public Health 2023,
23, 258.
[Google Scholar]
-
23.
Marinoni M, Parpinel M, Gasparini A, Ferraroni M, Edefonti V. Risky behaviors, substance use, and other lifestyle correlates of energy drink consumption in children and adolescents: A systematic review.
Eur. J. Pediatr. 2022,
181, 1–13.
[Google Scholar]
-
24.
Tóth Á, Soós R, Szovák EM. Najbauer N, Tényi D, Csábí G, et al. Energy drink consumption, depression, and salutogenic sense of coherence among adolescents and young adults.
Int. J. Environ. Res. Public Health 2020,
17, 1290.
[Google Scholar]
-
25.
Memudu AE, Ebun O, Osahon IR, Oviosun A. Caffeinated energy drink induces oxidative stress, lipid peroxidation and mild distortion of cells in the renal cortex of adult wistar rats.
Eur. J. Pharm. Med. Res. 2020,
6, 817–824.
[Google Scholar]
-
26.
Itany M, Diab B, Rachidi S, Awada S, Al Hajje A, Bawab W, et al. Consumption of energy drinks among lebanese youth: A pilot study on the prevalence and side effects.
Int. J. High Risk Behav. Addict. 2014,
3, e18857.
[Google Scholar]
-
27.
Hatem G, Eid E, Zaraket I, Mechref S, Awada S, Al-Hajje A, et al. Energy drink consumption among physically active persons in lebanon: a multicenter cross-sectional study.
Cent. Eur. J. Sport Sci. Med. 2023,
42, 5–15. doi:10.18276/cej.2023.2-01.
[Google Scholar]
-
28.
Yassin N, Afifi R, Singh N, Saad R, Ghandour L. “There is zero regulation on the selling of alcohol”: the voice of the youth on the context and determinants of alcohol drinking in Lebanon.
Qual. Health Res. 2018,
28, 733–744.
[Google Scholar]
-
29.
Khalil M, Antoun J. Knowledge and consumption of caffeinated products by university students in Beirut, Lebanon.
Clin. Nutr. ESPEN 2020,
37, 213–217.
[Google Scholar]
-
30.
Hatem G, Zeidan J, Goossens M, Moreira C. Normality testing methods and the importance of skewness and kurtosis in statistical analysis.
BAU J. -Sci. Technol. 2022,
3, 7.
[Google Scholar]
-
31.
Kim JW, Lee BC, Lee DY, Seo CH, Kim S, Kang TC, et al. The 5-item Alcohol Use Disorders Identification Test (AUDIT-5): An effective brief screening test for problem drinking, alcohol use disorders and alcohol dependence.
Alcohol Alcohol. 2013,
48, 68–73.
[Google Scholar]
-
32.
Azagba S, Langille D, Asbridge M. An emerging adolescent health risk: Caffeinated energy drink consumption patterns among high school students.
Prev. Med. 2014,
62, 54–59.
[Google Scholar]
-
33.
Galimov A, Hanewinkel R, Hansen J, Unger JB, Sussman S, Morgenstern M. Energy drink consumption among German adolescents: Prevalence, correlates, and predictors of initiation.
Appetite 2019,
139, 172–179.
[Google Scholar]
-
34.
Subaiea GM, Altebainawi AF, Alshammari TM. Energy drinks and population health: consumption pattern and adverse effects among Saudi population.
BMC Public Health 2019,
19, 1539.
[Google Scholar]
-
35.
Dillon P, Kelpin S, Kendler K, Thacker L, Dick D, Svikis D. Gender differences in any-source caffeine and energy drink use and associated adverse health behaviors.
J. Caffeine Adenosine Res. 2019,
9, 12–19.
[Google Scholar]
-
36.
Kumar G, Onufrak S, Zytnick D, Kingsley B, Park S. Self-reported advertising exposure to sugar-sweetened beverages among US youth.
Public Health Nutr. 2015,
18, 1173–1179.
[Google Scholar]
-
37.
Khan N. Caffeinated beverages and energy drink: Pattern, awareness and health side effects among Omani university students.
Biomed. Res. 2019,
30, 113–121.
[Google Scholar]
-
38.
Mora-Rodriguez R, Pallares JG. Performance outcomes and unwanted side effects associated with energy drinks.
Nutr. Rev. 2014,
72, 108–120.
[Google Scholar]
-
39.
de Souza JG, Del Coso J, Fonseca FD, Silva BV, de Souza DB, da Silva Gianoni RL, et al. Risk or benefit? Side effects of caffeine supplementation in sport: A systematic review.
Eur. J. Nutr. 2022,
61, 3823–3834.
[Google Scholar]
-
40.
Droste N, Pennay AE, Lubman DI, Zinkiewicz L, Peacock A, Miller P. The right place at the right time: The social contexts of combined alcohol and energy drink use.
Drugs Educ. Prev. Policy 2016,
23, 445–456.
[Google Scholar]
-
41.
Nuss T, Morley B, Scully M, Wakefield M. Energy drink consumption among Australian adolescents associated with a cluster of unhealthy dietary behaviours and short sleep duration.
Nutr. J. 2021, 20, 1–10.
[Google Scholar]
-
42.
Yasuma N, Imamura K, Watanabe K, Nishi D, Kawakami N, Takano A. Association between energy drink consumption and substance use in adolescence: A systematic review of prospective cohort studies.
Drug Alcohol Depend. 2021,
219, 108470.
[Google Scholar]
-
43.
Nakhoul L, Obeid S, Sacre H, Haddad C, Soufia M, Hallit R, et al. Attachment style and addictions (alcohol, cigarette, waterpipe and internet) among Lebanese adolescents: a national study.
BMC Psychol. 2020,
8, 33.
[Google Scholar]
-
44.
Galimov A, Hanewinkel R, Hansen J, Unger JB, Sussman S, Morgenstern M. Association of energy drink consumption with substance-use initiation among adolescents: a 12-month longitudinal study.
J. Psychopharmacol. 2020,
34, 221–228.
[Google Scholar]
-
45.
Awada S, Ahmad L, Assi RB, Rafei Z, Omar CA, Hatem G. Health-related Quality of life of medical students during the COVID-19 pandemic: A cross-sectional study in Lebanon.
Power Educ. 2024,
16, 1–3.
[Google Scholar]
-
46.
Hatem G, Goossens M. Health care system in lebanon: A review addressing health inequalities and ethical dilemmas of frontline workers during COVID-19 pandemic.
BAU J.—Health Wellbeing 2022,
5, 4.
[Google Scholar]