1. Introduction
Age determination in the case of missing documents has gained a great deal of merit in recent years due to the refugee crisis. It is carried out on an interdisciplinary basis in Germany according to known standards. The focus is on an interdisciplinary approach, which is combined into an overall expert opinion by involving experts from forensic medicine as well as from radiology and dentistry. Age determination based on biological structures is used both within and outside of criminal proceedings and is intended to determine the most probable age in the overall result [
1]. The legally relevant age limits of 14, 18 and 21 are of particular interest. In this case, the lack of documents and legal proof of the real age is resorted to the development of biological structures. Here, ossifications of biological structures and their correlation with age are well studied in the literature [
2,
3]. A major distinction must be made between age determination in living individuals and that in deceased individuals. Radiation exposure is widely discussed to be reduced to a minimum in relation to the benefit of age determination in living subjects, and the accuracy of the method is the subject of literature with divergent results in outcome [
4,
5,
6]. Consequently, strict requirements govern the permitted methodologies for using radiation in age determination, with current recommendations identifying wisdom teeth as a reliable biological marker. The use of, e.g., computed tomography scans for the visualization of the sutures and their ossifications in the head area could not be established in the literature. Due to the variance, they are only used in deceased individuals when it comes to age diagnostics, but seem to be often underestimated value for age determination according to Ruengdit et al. [
7]. In contrast, common diseases such as hyperthyroidism, thalassemia, and metabolic disorders are assumed to have an influence on early ossification of the sutures [
8]. Dental age determination using the orthopantomogram as a 2D diagnostic method is used worldwide and is also performed in Germany as a standard procedure in an interdisciplinary approach. Nowadays, 2D diagnostics are supported by 3D diagnostics in an everyday dental practice when there are special indications—for example when planning guided implantology and assessing the nerve position in the case of complicatedly displaced wisdom teeth [
9,
10]. However, this is not a standard procedure and is associated with a higher radiation dose [
11,
12]. In the literature, the wisdom teeth, which are of interest for the relevant age range between 14 and 22, show a population- and sex-specific development [
13]. The presence of wisdom teeth is crucial for dental age determination and can be limited by frequent congenital absence. In a study by Gambier et al., the forensic age estimation method focuses on assessing third molar eruption stages via orthopantomograms. While offering a simpler and faster alternative to detailed developmental analyses, Gambier et al. found that fully erupted molars are a strong, but not entirely definitive, indicator of being 18 or older [
14]. Although Gambier’s method offers valuable insights, its reliability is currently limited for definitive forensic age determination, given the requirement for all four third molars to be fully erupted and the natural variability in third molar development among individuals. Further research is essential to enhance the accuracy and applicability of this method [
15]. In a study by Yamada et al., it was found that 30% of the population had an agenesis of wisdom teeth [
16]. In a study by Kirkham et al., it was shown that the congenital absence of a wisdom tooth in one jaw is more likely to result in the absence of the other wisdom tooth in the same jaw [
17]. If all wisdom teeth are present, the evaluation of all four teeth is recommended if they can be radiologically located adequately [
1,
18]. Differences between the development of wisdom teeth in the maxilla and mandible could be described in the literature as well as between the right and left side of the patients [
19]. A study from the Thai region was able to show that if only the mandibular wisdom teeth were considered and stage H was declared according to the Demirjian staging method [
20], there was an almost certain probability that the subject had reached the age of 18 [
21]. Furthermore, a study could show that lower wisdom teeth are associated with a more accurate determination of the chronological age [
22]. Nevertheless, no study can be found in the literature that advocates a specific combination of wisdom teeth and clavicles while performing age estimation. After the completion of tooth development, age determination using dental methods is limited. Other methods, such as the original Gustafson’s age determination based on the determination of secondary dentin deposition, translucency and resorption of the tooth root, are accompanied by extraction of the tooth. This method has been further refined by multiple scientists to eliminate its invasive nature and enable dental age estimation in older individuals [
23,
24]. A non-invasive methodology for dental age determination in living individuals is mandatory and aligns with the standard procedure established by the working group for forensic age diagnostics (AGFAD). The developmental stages of the wisdom teeth (A-H) are classified according to the much-studied Demirjian staging method [
6,
25]. When the growth of the hand is completed (according to the Greulich and Pyle Atlas method), a computed tomography of the ossification of the medial epiphyseal fossa of the clavicles is attached. These ossify last compared to the entire skeleton [
18]. The five stages with respective sub-stages provide information on the completion of the 19th (stage 3c) and 21st year of life (stage 4). There is no indication of a clavicle x-ray in the case of underage hand growth. The clavicles then confirm the age of majority by the corresponding staging and specify it more precisely in the context of age determination [
6,
26,
27]. This study aims to investigate the interaction between dental age diagnostics and clavicle analysis and their combined influence on the overall forensic expert’s opinion. Even though Demirjian’s staging method is implemented frequently in the literature/forensic practice, it is still unclear how much this method agrees with other methods, such as the clavicula. Therefore, the study aimed to determine the reliability rate by comparing dental age estimation and the clavicula based on the following hypothesis:
- Combining the wisdom teeth with the clavicle leads to a more accurate overall result.
- Combining only the lower wisdom teeth with the clavicle leads to a more precise result in the overall age estimation.
2. Materials and Methods
2.1. Subject Group
Overall expert opinions generated by the Institute of Forensic Medicine in (Mainz) from 2011 to 2021 were re-examined. All cases that had been commissioned within as well as outside of criminal proceedings were examined in reference to the existence of wisdom teeth and clavicula-CTs in the expert opinions. Thereby, 104 cases with existing clavicula-CTs were found, of which wisdom teeth were present in 84 cases. Only 4 female cases were found in this time period. To maintain uniformity within the group, these were excluded. We used the FDI World Dental Federation’s notation system as our schema for tooth identification. There was always one forensic radiologist, one forensic odontologist and one forensic pathologist, performing the overall expert opinions in equal parts as a standard procedure according to the Guidelines of the Study Group on Forensic Age Diagnostics (AGFAD) in Germany.
2.2. Sample
All subjects were male. They came from 15 countries, with 31% from Afghanistan, 24% from Somalia, 14% from Guinea, and 6% from Iran. Other countries contributed fewer than 5% of the subjects. The mean estimated age was approximately 21, and the exact age was unknown. All individuals were asylum seekers required to undergo age estimation following the standard procedure.
2.3. Statistical Analysis
A total of five indicators were examined to predict the estimated age: development of the clavicula coded according to Wittschieber et al. (2014) and mineralization of the four wisdom teeth coded according to Demirjian’s method. Ordinary Least Square regression analyses were performed for each indicator separately due to missing data on various indicators, e.g., if a certain tooth was not available. Unstandardized regression coefficients with standard errors were reported, including the adjusted explained variance of the estimated age (R²). 95% confidence intervals were reported. Finally, the predictive value of taking more than one possible age indicator into a model simultaneously was examined. Due to missing data on the clavicula developmental stage and some teeth, multiple imputations had to be performed. Only the 84 cases having an age estimation were included in this part of the statistic (Hardt et al., 2012). A total of 100 datasets were imputed using the MICE algorithm with predictive mean matching (van Buuren et al., 2011). Statistical analyses were performed by STATA 17 (STATACorp, College Station, TX, USA, 2021), R², after multiple imputations by the package mibeta, using an algorithm described by Hare (2009).
3. Results
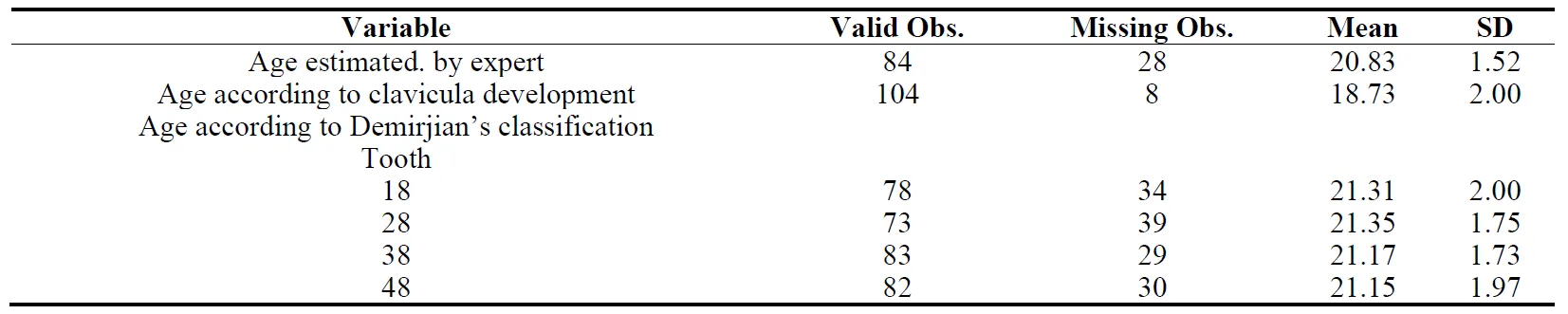
displays the sample description. An estimate of the age could be performed for 84 of the 112 subjects. However, the remaining 28 subjects’ available data did not provide sufficient evidence. The development of the clavicula could be determined in 104 subjects, 24% of them had a developed clavicula, 76% did not. Hand development was observed in all subjects. Wisdom teeth were far less often available ().
All five indicators were significantly associated with the estimated age (correlations between
r = 0.22 and 0.69, all
p < 0.01).
Clavicula was the best indicator, Tooth 48 the second best (
r = 0.69 and 0.59, , last column. Teeth 38 and 28 were the third-best indicators (
r = 0.46 for each), and
tooth 18 the poorest (
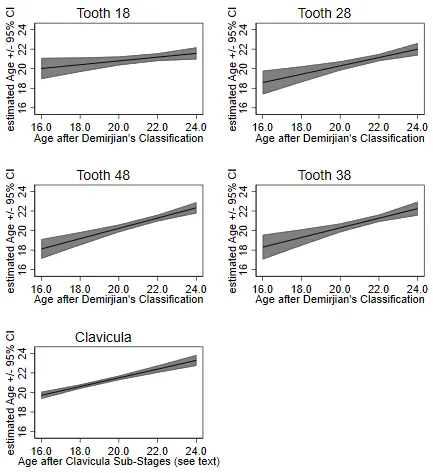
r = 0.22, ). displays the linear prediction of the estimated age.
Clearly visible was that clavicula and tooth 48 perform better than the other ones.
Figure 1. Prediction of expert estimated age by development of the clavicula or the mineralization of the four wisdom teeth.
. Linear prediction of age when utilizing clavicula development and Demirjian’s classification of each tooth individually.
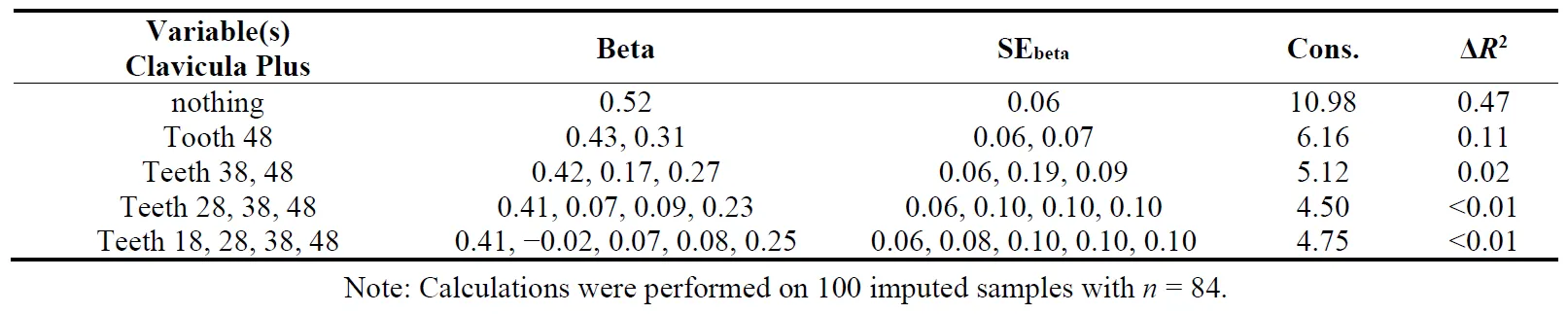
shows the results after multiple imputations to examine the prediction of combined indicators. Clavicula development alone (first line in ) explained in this model 47% of the variance of the age estimation, which is 1% less than in the bivariate analysis. This is normal in datasets of this size.
Adding tooth 48, which showed the second-best prediction in the bivariate analyses,
led to an increase of the explained variance of 11% to a total of 58% explained variance (
p < 0.001). Including the next-best candidate, tooth 38, resulted in only a 2% increase in explained variance, which was not statistically significant (
p > 0.34). Adding two additional teeth showed no relevant effect.
. Linear prediction of age when utilizing clavicula development stage and mineralization of several teeth combined.
4. Discussion
Teeth show a constant biological development in primary and secondary dentition, which is hardly influenced by external factors [
28]. Besides systematic factors, peculiarities in the development of the stomatognathic system do not seem to influence the expression of wisdom teeth as well. Of particular interest here is the differentiation between the maxilla and mandible. Follow-up studies of unilateral palatally displaced canine teeth in the maxilla showed no statistically significant change in the development of teeth related to their biological age [
29]. This contrasts with a 2011 study by Rozylo-Kalinowska et al., who found delayed tooth development in buccally or palatally displaced canines in the maxilla [
30]. In contrast, Becker et al. demonstrated that buccally displaced canines showed no significant difference in teeth development [
31]. However, palatally emerging canines in the maxilla showed abnormalities in the overall development of permanent dentition. In a study from the Thai region by Duangto et al., only mandibular wisdom teeth were used since maxillary wisdom teeth are often subject to superimposition of anatomical structures, such as the os zygomaticus, maxillary sinus, and processus zygomaticus [
32]. This supports our assumption that mandibular wisdom teeth should be clearly preferred when it comes to dental age estimation. Friedrich et al. were able to demonstrate that the root development of the maxillary wisdom teeth was not assessable in twice as many cases as of the mandible [
33]. In this study, the mandibular wisdom teeth also showed a stronger correlation with the overall age than the maxillary wisdom teeth. Tooth 48 showed the best predictability, and tooth 38 was the second best. A study by Angelakopoulos et al. that included African and European and Asian subjects found no significant difference between tooth 38 and 48 in correlation to actual age [
34]. A left-right asymmetry has been described in the literature. Still, no correlation between the asymmetric development of the wisdom teeth and the asymmetry of the development of the clavicles could be found [
35]. The clavicle’s significance in age determination, particularly in verifying legal adulthood, has been extensively documented in the literature and applied in population studies, including the use of innovative methods like MRI [
27,
36,
37,
38]. In this study, it was shown that the clavicle alone can best predict age, whereby the combination with the dental methodology (wisdom tooth regio 48) shows optimization. An alternative identification method is the Cameriere technique, as described in the study by Celik Güler et al. [
39]. The study compared Cameriere’s open-apex method for dental age and the skeletal age method using the fourth cervical vertebra (C4) and found that both methods showed reduced accuracy in older adolescents. For children under 13, the skeletal age method provided more reliable age estimates, while both methods tend to underestimate age in adolescents, highlighting limitations for forensic applications in older age groups [
39]. In a study by De Tobel et al., a multifactorial age determination that included all four wisdom teeth, as well as the left wrist, as well as both clavicles was shown to perform better than the age estimation with just one age indicator [
40]. This supports the requirement for interdisciplinary process chains in age estimation and reinforces the standardized approach within and outside the criminal justice system [
6,
41,
42,
43]. The agenesis of one or all wisdom teeth presents a problem in dental age determination [
44] and requires further development and investigation regarding combinations of age determination factors for the most accurate methodology. Further statistical analyses are required for the creation of a statistical model if the age of the subject is known. A study by Kvaal et al. compared skeletal and dental age assessment methods for unaccompanied asylum-seeking minors in Norway to determine if individuals were over or under 18 years. Skeletal maturity (hand-wrist) and third molar development showed 83% agreement for males and 79% for females, with skeletal assessments often indicating an older age than dental. Differences in assessment consistency across ethnic groups highlight the need for a combined approach, though biological variation remains a challenge [
45].
In a study from Portugal by Pereira et al., it could be demonstrated that dental age estimation tends to underestimate the chronological age by using most of the common methods described in the literature. This highlights the judicial effort to adopt the best approach under the principle of in “dubio pro reo”, even though some studies suggest a preference for assessing wisdom teeth in the mandible [
37,
46]. Nevertheless, the use of sex- and population-specific age information is important to ensure an accurate approach to the actual age. In this study, only male subjects were to be followed up, which should be clearly addressed as a limitation of the present study. In contrast to this, the literature contains studies of female and male subjects; for example, a study from India by Ashifa et al. could demonstrate that maxillary and mandibular wisdom teeth develop at different rates, and according to Demirjian stages F–H are reached faster in the maxilla in males than in females [
19].
Further studies should follow to investigate the combination of wisdom tooth and clavicle in relation to the actual confirmed age. In order to idealize the patient collective and to verify our results for clinical applicability, subsequent studies should harmonize the patient collective and test the resulting combinations on a collective that has a known age and includes women.
5. Conclusions
Within the limitations of this study, the following conclusions are drawn:
1. An interdisciplinary approach is essential in forensic age determination.
The statued approach of a team of experts consisting of radiologists, dentists and forensic pathologists has proven itself to help in the accuracy of age determination. Each discipline stands for a well-founded individual assumption, which, in its overall view, means a more accurate approximation of the actual age. Here, the clavicle shows itself to be an outstanding feature, especially for the evidence of adulthood.
2. The mandibular wisdom teeth are preferable to the maxillary wisdom teeth, in my opinion.
It could be observed that upper jaw wisdom teeth are often not included in the overall assessment due to poor assessability and quality. In this study, it was shown that the lower jaw wisdom teeth play a preferred role when it comes to determining the dental age. The combination of a lower jaw wisdom tooth and the clavicle was rated as the most effective approach, with the addition of further wisdom teeth providing no significant improvement.
3. In the presence of even one wisdom tooth, the combination of this with the clavicle can be used for age determination.
Due to agenesis or previous extractions, the presence of all four possible wisdom teeth is often not given. The results indicate that combining another feature, such as the clavicle, is essential for conducting a reliable age determination.
Author Contributions
Conceptualization, M.B., K.E., K.P.; methodology, M.B., J.H., K.P.; software, M.B.; validation, K.P., M.B., K.E., T.G. and J.H.; formal analysis, K.P.; investigation, M.B., K.E., P.B.; resources, M.B., K.E., P.B.; data curation, M.B., K.K., P.B.; writing—original draft preparation, M.B., K.E.; writing—review and editing, K.P., T.G. and K.K.; visualization, M.B.; supervision, K.P.; project administration, M.B. and K.P. All authors have read and agreed to the published version of the manuscript.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and Ethical approval was waived by the local Ethics Committee of Rhineland-Palatinate in view of the retrospective nature of the study and all the procedures being performed were part of the routine care.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Funding
This research received no external funding.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data Availability Statement
The data from this study were part of the dissertation paper from P.B. Data can be seen in Table 1, Table 2 and Table 3 and Figure.
References
-
1.
Schmeling A, Geserick G, Reisinger W, Olze A.
Age
estimation.
Forensic Sci. Int. 2007,
165, 178–181.
[Google Scholar]
-
2.
Bassed RB, Briggs C, Drummer OH. Analysis
of
time
of
closure
of
the
spheno-occipital
synchondrosis
using
computed
tomography.
Forensic Sci. Int. 2010,
200, 161–164.
[Google Scholar]
-
3.
Sinanoglu A, Kocasarac HD, Noujeim M. Age
estimation
by
an
analysis
of
spheno-occipital
synchondrosis
using
cone-beam
computed
tomography.
Leg Med. 2016,
18, 13–19.
[Google Scholar]
-
4.
Kapadia F, Stevens J, Silver D. Dental
Radiographs
for
Age
Estimation
in
US
Asylum
Seekers:
Methodological,
Ethical,
and
Health
Issues.
Am. J. Public. Health 2020,
110, 1786–1789.
[Google Scholar]
-
5.
Laniado N, Wright ML, Seymour B. The
use
of
dental
radiographs
for
age
estimation
of
unaccompanied
migrant
minors:
Scientific
and
ethical
concerns.
J. Public. Health Dent. 2022,
82, 349–351.
[Google Scholar]
-
6.
Schmeling A, Dettmeyer R, Rudolf E, Vieth V, Geserick G.
Forensic
Age
Estimation.
Dtsch. Arztebl. Int. 2016,
113, 44–50.
[Google Scholar]
-
7.
Ruengdit S, Troy Case D, Mahakkanukrauh P.
Cranial
suture
closure
as
an
age
indicator:
A
review.
Forensic Sci. Int. 2020,
307, 110111.
[Google Scholar]
-
8.
Ursitti F, Fadda T, Papetti L, Pagnoni M, Nicita F, Iannetti G, et al.
Evaluation
and
management
of
nonsyndromic
craniosynostosis.
Acta Paediatr. 2011,
100, 1185–1194.
[Google Scholar]
-
9.
Jorba-Garcia A, Gonzalez-Barnadas A, Camps-Font O, Figueiredo R, Valmaseda-Castellon E.
Accuracy
assessment
of
dynamic
computer-aided
implant
placement:
A
systematic
review
and
meta-analysis.
Clin. Oral. Investig. 2021,
25, 2479–2494.
[Google Scholar]
-
10.
Derksen W, Wismeijer D, Flugge T, Hassan B, Tahmaseb A. The
accuracy
of
computer-guided
implant
surgery
with
tooth-supported,
digitally
designed
drill
guides
based
on
CBCT
and
intraoral
scanning.
A
prospective
cohort
study.
Clin. Oral. Implant. Res. 2019,
30, 1005–1015.
[Google Scholar]
-
11.
Sezgin ÖS, Kayipmaz S, Yasar D, Yilmaz AB, Ozturk MH. Comparative
dosimetry
of
dental
cone
beam
computed
tomography,
panoramic
radiography,
and
multislice
computed
tomography.
Oral. Radiol. 2012,
28, 32–37.
[Google Scholar]
-
12.
Carrafiello G, Dizonno M, Colli V, Strocchi S, Pozzi Taubert S, Leonardi A, et al.
Comparative
study
of
jaws
with
multislice
computed
tomography
and
cone-beam
computed
tomography.
Radiol. Med. 2010,
115, 600–611.
[Google Scholar]
-
13.
Lewis JM, Senn DR. Dental
age
estimation
utilizing
third
molar
development:
A
review
of
principles,
methods,
and
population
studies
used
in
the
United
States.
Forensic Sci. Int. 2010,
201, 79–83.
[Google Scholar]
-
14.
Gambier A, Rerolle C, Faisant M, Lemarchand J, Pare A, Saint-Martin P.
Contribution
of
third
molar
eruption
to
the
estimation
of
the
forensic
age
of
living
individuals.
Int. J. Legal Med. 2019,
133, 625–632.
[Google Scholar]
-
15.
Svabova Nee Uhrova P, Benus R, Chovancova Nee Kondekova M, Vojtusova A, Novotny M, Thurzo A. Use
of
third
molar
eruption
based
on
Gambier’s
criteria
in
assessing
dental
age.
Int. J. Legal Med. 2023,
137, 691–699.
[Google Scholar]
-
16.
Chiba F, Makino Y, Motomura A, Inokuchi G, Torimitsu S, Ishii N, et al.
Age
estimation
by
multidetector
CT
images
of
the
sagittal
suture.
Int. J. Leg. Med. 2013,
127, 1005–1011.
[Google Scholar]
-
17.
Kirkham J, Kaur R, Stillman EC, Blackwell PG, Elcock C, Brook AH.
The
patterning
of
hypodontia
in
a
group
of
young
adults
in
Sheffield,
UK.
Arch. Oral. Biol. 2005,
50, 287–291.
[Google Scholar]
-
18.
Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, et al. Criteria
for
age
estimation
in
living
individuals.
Int. J. Legal Med. 2008,
122, 457–460.
[Google Scholar]
-
19.
Ashifa N, Parakh MK, Ulaganambi S. Estimation
of
Age
Using
Third
Molar
Development:
A
Radiological
Cross-Sectional
Study.
Am. J. Forensic Med. Pathol. 2020,
41, 115–118.
[Google Scholar]
-
20.
Demirjian A, Goldstein H, Tanner JM. A
new
system
of
dental
age
assessment.
Hum. Biol. 1973,
45, 211–227.
[Google Scholar]
-
21.
Duangto P, Iamaroon A, Prasitwattanaseree S, Mahakkanukrauh P, Janhom A.
New
models
for
age
estimation
and
assessment
of
their
accuracy
using
developing
mandibular
third
molar
teeth
in
a
Thai
population.
Int. J. Legal Med. 2017,
131, 559–568.
[Google Scholar]
-
22.
Bjelopavlovic M, Zeigner A-K, Hardt J, Petrowski K. Forensic
Dental
Age
Estimation:
Development
of
New
Algorithm
Based
on
the
Minimal
Necessary
Databases.
J. Pers. Med. 2022,
12, 1280.
[Google Scholar]
-
23.
Kvaal SI, Kolltveit KM, Thomsen IO, Solheim T. Age
estimation
of
adults
from
dental
radiographs.
Forensic Sci. Int. 1995,
74, 175–185.
[Google Scholar]
-
24.
Timme M, Timme WH, Olze A, Ottow C, Ribbecke S, Pfeiffer H, et al. Dental
age
estimation
in
the
living
after
completion
of
third
molar
mineralization:
New
data
for
Gustafson’s
criteria.
Int. J. Legal Med. 2017,
131, 569–577.
[Google Scholar]
-
25.
Rolseth V, Mosdol A, Dahlberg PS, Ding Y, Bleka O, Skjerven-Martinsen M, et al. Age
assessment
by
Demirjian’s
development
stages
of
the
third
molar:
A
systematic
review.
Eur. Radiol. 2019,
29, 2311–2321.
[Google Scholar]
-
26.
Kellinghaus M, Schulz R, Vieth V, Schmidt S, Schmeling A. Forensic
age
estimation
in
living
subjects
based
on
the
ossification
status
of
the
medial
clavicular
epiphysis
as
revealed
by
thin-slice
multidetector
computed
tomography.
Int. J. Legal Med. 2010,
124, 149–154.
[Google Scholar]
-
27.
Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, et al.
The
value
of
sub-stages
and
thin
slices
for
the
assessment
of
the
medial
clavicular
epiphysis:
A
prospective
multi-center
CT
study.
Forensic Sci. Med. Pathol. 2014,
10, 163–169.
[Google Scholar]
-
28.
Manjunatha BS, Soni NK.
Estimation
of
age
from
development
and
eruption
of
teeth.
J. Forensic Dent. Sci. 2014,
6, 73–76.
[Google Scholar]
-
29.
Hashim F, Roberts G, Alzoubi E, Camilleri S. Dental
age
estimation
of
young
subjects
with
unilateral
palatally
displaced
canine
teeth.
Am. J. Orthod. Dentofacial Orthop. 2021,
160, 560–566.
[Google Scholar]
-
30.
Rozylo-Kalinowska I, Kolasa-Raczka A, Kalinowski P. Dental
age
in
patients
with
impacted
maxillary
canines
related
to
the
position
of
the
impacted
teeth.
Eur. J. Orthod. 2011,
33, 492–497.
[Google Scholar]
-
31.
Becker A, Chaushu S.
Dental
age
in
maxillary
canine
ectopia.
Am. J. Orthod. Dentofacial Orthop. 2000,
117, 657–662.
[Google Scholar]
-
32.
de Oliveira FT, Capelozza AL, Lauris JR, de Bullen IR. Mineralization
of
mandibular
third
molars
can
estimate
chronological
age--Brazilian
indices.
Forensic Sci. Int. 2012,
219, 147–150.
[Google Scholar]
-
33.
Friedrich RE, Ulbricht C, Ljuba ABvM. The
influence
of
wisdom
tooth
impaction
on
root
formation.
Ann. Anat. 2003,
185, 481–492.
[Google Scholar]
-
34.
Angelakopoulos N, Galic I, Balla SB, Kis HC, Gomez Jimenez L, Zolotenkova G, et al. Comparison
of
the
third
molar
maturity
index
(I3M)
between
left
and
right
lower
third
molars
to
assess
the
age
of
majority:
A
multi-ethnic
study
sample.
Int. J. Legal Med. 2021,
135, 2423–2436.
[Google Scholar]
-
35.
Bassed RB, Briggs C, Drummer OH. The
incidence
of
asymmetrical
left/right
skeletal
and
dental
development
in
an
Australian
population
and
the
effect
of
this
on
forensic
age
estimations.
Int. J. Legal Med. 2012,
126, 251–257.
[Google Scholar]
-
36.
Scharte P, Vieth V, Schulz R, Ramsthaler F, Puschel K, Bajanowski T, et al. Comparison
of
imaging
planes
during
CT-based
evaluation
of
clavicular
ossification:
A
multi-center
study.
Int. J. Legal Med. 2017,
131, 1391–1397.
[Google Scholar]
-
37.
Reder SR, Fritzen I, Brockmann MA, Hardt J, Elsner K, Petrowski K, et al. Comparing
a
common
clavicle
maturation-based
age
estimation
method
to
ordinary
regression
analyses
with
quadratic
and
sex-specific
interaction
terms
in
adolescents.
Sci. Rep. 2024,
14, 2754.
[Google Scholar]
-
38.
Widek T, De Tobel J, Ehammer T, Genet P. Forensic
age
estimation
in
males
by
MRI
based
on
the
medial
epiphysis
of
the
clavicle.
Int. J. Legal Med. 2023,
137, 679–689.
[Google Scholar]
-
39.
Guler OC, Deniz Y, Arslan S. Comparison
of
Dental
and
Skeletal
Age
Estimating
Methods
in
Children.
Acta Stomatol. Croat. 2023,
57, 2–11.
[Google Scholar]
-
40.
De Tobel J, Fieuws S, Hillewig E, Phlypo I, van Wijk M, de Haas MB, et al.
Multi-factorial
age
estimation:
A
Bayesian
approach
combining
dental
and
skeletal
magnetic
resonance
imaging.
Forensic Sci. Int. 2020,
306, 110054.
[Google Scholar]
-
41.
Lossois M, Cyteval C, Baccino E, Peyron PA. Forensic
age
assessments
of
alleged
unaccompanied
minors
at
the
Medicolegal
Institute
of
Montpellier:
A
4-year
retrospective
study.
Int. J. Legal Med. 2022,
136, 853–859.
[Google Scholar]
-
42.
Hagen M, Schmidt S, Schulz R, Vieth V, Ottow C, Olze A, et al. Forensic
age
assessment
of
living
adolescents
and
young
adults
at
the
Institute
of
Legal
Medicine,
Munster,
from
2009
to
2018.
Int. J. Legal Med. 2020,
134, 745–751.
[Google Scholar]
-
43.
Mansour H, Fuhrmann A, Paradowski I, van Well EJ, Puschel K. The
role
of
forensic
medicine
and
forensic
dentistry
in
estimating
the
chronological
age
of
living
individuals
in
Hamburg,
Germany.
Int. J. Legal Med. 2017,
131, 593–601.
[Google Scholar]
-
44.
Akman H, Surme K, Cimen T, Ayyildiz H. Accuracy
of
different
dental
age
estimation
methods
for
determining
the
legal
majority
of
18
years
in
the
Turkish
population.
Clin. Oral. Investig. 2022,
26, 4537–4547.
[Google Scholar]
-
45.
Kvaal SI, Haugen M. Comparisons
between
skeletal
and
dental
age
assessment
in
unaccompanied
asylum
seeking
children.
J. Forensic Odontostomatol. 2017,
35, 109–116.
[Google Scholar]
-
46.
Pereira CP, Rodrigues A, Augusto D, Santos A, Nushic V, Santos R.
Dental
age
assessment
and
dental
scoring
systems:
Combined
different
statistical
methods.
Int. J. Legal Med. 2024,
138, 1533–1557.
[Google Scholar]
 Katrin Elsner
2,†
Keywan Kianusch
1
Philipp Behrendt
1
Tanja Germerott
2
Jochen Hardt
3
Katja Petrowski
3
Katrin Elsner
2,†
Keywan Kianusch
1
Philipp Behrendt
1
Tanja Germerott
2
Jochen Hardt
3
Katja Petrowski
3