1. Introduction
Depression is one of the most common mental disorders. According to estimates from the Institute for Health Metrics and Evaluation, approximately 280 million people worldwide suffer from depression [
1]. Empirical evidence emphasizes that the depression prevalence among university students is gradually increased [
2], and the detection rate of depression among college students is 24.17%, which is much higher than the 10.6% depression detection rate of the general population [
3]. Continuous academic pressure, changes in living environment and lifestyle, and economic or employment stress make university students more vulnerable to depression [
4]. Depression is significantly negatively related to academic performance [
5], and students with moderate levels of depressive symptoms demonstrated lower academic performance than normal students [
6]. Besides, depression could lead to decreased physical health, difficulties in social functioning [
7,
8], and ultimately increased suicide risk [
9]. Therefore, unraveling the underlying mechanisms of depression among university students could provide evidence for the prevention and intervention of depression.
Over the past two decades, the dual-process model has been applied extensively in the study of various mental disorders, including depression [
10,
11,
12]. This model suggests that behavior is controlled by two systems: a reflexive system and a reflective system, which function and compete with each other. The reflexive system engages in bottom-up, automatic activation through associative processes, requiring minimal cognitive resources. In contrast, the reflective system involves top-down, conscious decision-making processes based on goals and potential consequences, necessitating cognitive resource allocation [
13,
14]. Beevers [
15] utilized the dual-process model to explain depression, suggesting that individuals with negative associative processes exhibit a negative bias toward self-relevant information, leading to susceptibility to depression. When cognitive resources are sufficient, the reflective system could rectify these associative processes. However, if negative cognitive processing bias is not fully corrected, it will lead to irritability, cognitive resource depletion, reinforcement of associative processing, and creating a vicious cycle that ultimately contributes to depression [
15]. Negative cognitive processing bias describes the inclination of individuals to choose, memorize, and interpret information negatively during the information processing phase [
16,
17,
18]. The reflective process is linked to self-control [
19]. Insufficient self-control may result in emotion dysregulation, persistent negative mood, and subsequently depression [
20]. Therefore, grounded in the dual-process model, this study takes negative cognitive processing bias and self-control as reflexive and reflective system variables to investigate their synergistic antagonistic mechanisms on depression.
Negative cognitive processing bias is closely related to depression. Negative cognitive processing bias indicates the involuntary inclination to prioritize attention, memory, and interpretation of negative information [
20,
21]. Previous research has shown that individuals at risk for depression or depressed patients both exhibit negative cognitive processing bias [
22], and this bias is a pivotal predisposing factor for depression development, maintenance, and recurrence [
23,
24,
25]. However, the significance of distinct dimensions of negative cognitive processing bias for depression could be different. Notably, the most relevant aspect of depression is memory bias [
26], and depressed individuals exhibit a bias in memory that aligns with their mood [
21]. According to Marchetti’s study, negative memory bias is strongly related to various depression symptoms, including sad mood, feelings of worthlessness, and pessimism [
27]. Relatively consistent conclusions have also been yielded in studies examining the connection between interpretation bias and depression. Negative interpretation bias has been identified in both adult and adolescent depression samples [
28]. Additionally, those individuals with severe depression interpret ambiguous emotional information more negatively compared with mild and moderate individuals [
29]. Nevertheless, concerning negative attention bias, its association with depression remains controversial. Some studies have suggested a lack of significant correlation between negative attention bias and depression symptoms [
30,
31]. However, a 6-week longitudinal study has identified negative attention bias as the most reliable predictor of changes in depression symptoms [
32].
Self-control refers to the capacity to restrain undesirable thoughts or behaviors in pursuit of long-term achievements [
33], serves as an effective protective factor against depression [
34]. Individuals with high self-control are more likely to build more harmonious interpersonal relationships to reduce depression risk [
33,
35,
36,
37]. Moreover, enhancing the ability of self-control among university students experiencing major depressive disorder has been identified helpful to mitigate the severity of depression symptoms [
38]. Conversely, lack of self-control weakens the capacity to regulate emotions and behaviors [
39]. Chronic control failure increases restlessness and anxiety, elevating the risk of depression [
40]. In addition, anhedonia makes depressed individuals lack motivation to pursue goals, and low self-control will amplify this problem, hindering action-taking [
13].
Negative cognitive processing bias and self-control have a mutually inhibitory relationship. On one hand, self-control could suppress the maladaptive pattern of negative cognitive processing bias. By regulating thoughts and emotions, self-control enables individuals to better adapt to their environment [
33]. On the other hand, negative cognitive processing bias tends to diminish self-control capability. It may lead individuals to rumination, depleting the psychological resources necessary for problem-solving [
41], thereby weakening self-control. Additionally, negative cognitive processing bias can elevate negative emotions and deepen individual dysregulated responses, ultimately reducing self-control [
42,
43].
However, concerning depression, there are few studies investigating the relationship between negative cognitive processing bias, self-control, and depression based on the dual-process model. In addition, previous studies primarily concentrated on the overall level of depression, neglecting exploration at the symptom level. Empirical studies have indicated that as a heterogeneous disorder, depression consists of core and peripheral symptoms [
44], with specific individual symptom differing in underlying biological mechanisms, predisposing factors, and damaging effects. Specific life events predict the occurrence of distinct depression symptoms and there may be potential direct causal relationships between these symptoms [
45]. Assessing the severity of depression using a total score might obscure the associations between symptoms, impeding the exploration of the interplay of different symptoms and their respective associated risk and protective factors. Therefore, a focused inquiry into the relationships between diverse dimensions of negative cognitive processing bias, self-control, and specific depression symptoms, employing the dimension-symptom paradigm rooted in the dual-process model, is important to get a more accurate comprehension of the mechanism of depression.
Consequently, the network analysis method was adopted in order to address these gaps. Network analysis theory interprets mental disorders as results of interactions among symptoms [
46,
47] to identify possible transmissibility and potential causality between symptoms [
48]. The network comprises symptoms of disorders or factors influencing symptoms (nodes) and the edges connecting them. It visualizes relationships between symptoms and influencing factors, aiding researchers in identifying which symptom is most closely associated with each influencing factor [
49]. Furthermore, network analysis provides new indicators to identify central nodes that have the greatest impact on the entire network, as well as bridge nodes that facilitate transmission between communities. These nodes are identified as potential targets for more effective disease prevention and intervention [
50]. Thus, the present study employed network analysis to explore the relationships between negative cognitive processing bias, self-control, and depression at a fine-grained level. By estimating node expected influences, bridge expected influences, and the network structure, our aim was to examine: (1) which symptom or influencing factor dimension plays an important role in maintaining the entire network and the co-occurrence of these constructs; (2) how the unique connection pathways link different negative cognitive processing biases to depression symptoms, as well as dimensions of self-control to depression symptoms; (3) how negative cognitive processing bias and self-control interact with each other in the manifestation of depression. Based on previous research that increased interpretation of negative information, difficulties in distracting from mood-congruent negative materials, and cognitive control deficits in processing negative information are characters of depression [
20], we hypothesized that negative cognitive processing biases and self-control are primarily associated with emotional and cognitive symptoms of depression. According to the antagonistic relationship between the reflexive system and the reflective system of the dual-process model, we hypothesized that negative cognitive processing bias and self-control counteract each other in the manifestation of depression. There were no specific hypotheses about central and bridge symptoms formulated on account of the novelty of the network constructed by the three variables.
2. Methods
2.1. Participants
This cross-sectional study was conducted through an online survey from September 2022 to October 2022. A convenience sampling method was adopted to recruit participants from a university in Tianjin, China. A total of 1211 students participated in the study, and 43 were excluded for answering the questionnaire incompletely (the effective rate is 96.4%). Thus, data from 1168 participants (
M = 17.98 years,
SD = 0.72 years, age range: 16–30 years) was analyzed, with females comprising the majority (61.04%). Prior to participation, informed consent was obtained from all individuals, and the study received approval from the Ethics Committee of Tianjin Medical University (study number: TMuhMEC2022019).
2.2. Measures
Depression symptoms were evaluated using the Chinese version of the nine-item Patient Health Questionnaire (PHQ-9) [
51,
52]. Participants were asked to recall the past two weeks when answering the questionnaire. The scale comprises 9 items, and each is rated from 0 (not at all) to 3 (nearly every day). The total score ranges from 0 to 27, and higher scores reflect greater severity of depression symptoms. Total scores of 5, 10, 15, and 20 represent mild, moderate, moderately severe, and severe depression, respectively. The Chinese version of the PHQ-9 has demonstrated good reliability and validity, with a Cronbach’s alpha coefficient of 0.84 in the present sample.
The negative Cognitive Processing Bias Questionnaire (NCPBQ) was administered to assess the negative bias when processing information. This study focused on three subscales of the NCPBQ: negative attention bias, negative memory bias, and negative interpretation bias [
53,
54]. Each subscale consists of 5 items, with responses rated on a 4-point Likert scale ranging from 1 (complete nonconformity) to 4 (complete conformity). A higher score indicates a stronger negative cognitive processing bias. The present study demonstrated preferable internal consistency, with Cronbach’s α values of 0.86, 0.88, and 0.83 for negative attention bias, negative memory bias, and negative interpretation bias, respectively.
The Chinese version of the Brief Self-Control Scale (BSCS) was applied to measure the capability of self-control [
33,
55]. The scale comprises 7 items, rated on a 5-point Likert scale ranging from 1 (complete nonconformity) to 5 (complete conformity). The BSCS consists of two subscales: self-discipline (items 1, 3, and 5) and impulse control (items 2, 4, 6, and 7), with the latter being reverse-scored. The total score ranges from 7 to 35, with higher scores indicating greater self-control ability. The Cronbach’s α values of the two subscales were 0.73 and 0.76, respectively.
2.3. Statistical Analysis
2.3.1. Network Estimation
All data analyses were conducted using R (version 4.2.0) [
56], and R packages qgraph (version 1.9.2), bootnet (version 1.5), and networktools (version 1.5.0) were applied. The network model utilizes a node and edge representation, with nodes indicating variables, and edges indicating their associations. Grey edges represent positive associations, while red edges represent negative associations. The thickness of an edge reflects the strength of the association between two variables. To achieve a sparser and more interpretable network, the least absolute shrinkage and selection operator (LASSO) [
57] and extended Bayesian information criteria (EBIC) [
58] were applied, with tuning parameters setting 0.5. Given the skewed distribution of depression scores, the Spearman Correlation was used to calculate correlation coefficients. The R packages qgraph (version 1.9.2) [
59] and bootnet (version 1.5) [
60] were utilized to estimate and visualize the network model.
2.3.2. Estimation of Network Centrality, Accuracy, and Stability
To determine which symptom played a significant role in the network structure, the R package qgraph (version 1.9.2) [
59] was employed to calculate the expected influence (EI) of nodes. EI evaluates a node’s impact on others [
50], and nodes with high EI values are regarded as central symptoms of the network. Additionally, bridge expected influence (BEI) was computed via the R package networktools (version 1.5.0). Nodes with higher BEI values are considered to have a stronger connection with nodes of other communities. If BEI ranks in the top 20 percent, the node is identified as the bridge symptom [
61].
To evaluate the reliability of the network, we utilized the R package bootnet (version 1.5) [
60]. In order to calculate the accuracy of edge weights, the non-parametric method was adopted to compute 95% confidence intervals (CIs). A narrow range of 95% CIs indicates that the network is reliable. Additionally, 1000 bootstrap tests were performed to examine differences between edge weights and nodes’ EI [
60].
To evaluate the stability of centrality indexes, we employed a case-dropping bootstrap procedure to compute correlation stability (CS) coefficients. If most samples can be removed without significantly differing in centrality indices with the primary dataset, the network is considered stable. CS-coefficient values reflect the maximum proportion of samples that can be excluded. Ideally, the CS-coefficient values should be above 0.25, and preferably exceed 0.50 [
60].
3. Results
3.1. Study Sample
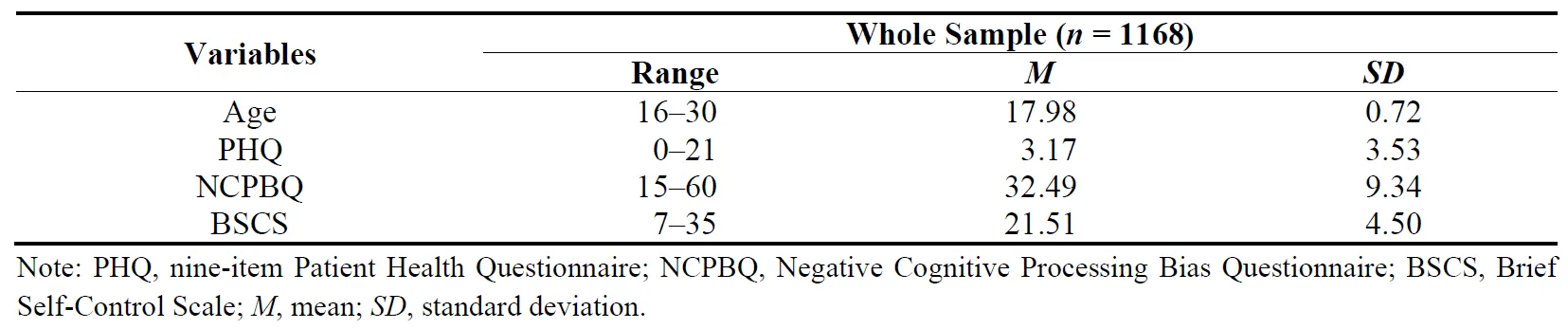
A cohort of 1211 undergraduate students were invited to participate in this study, and 1168 participants completed the assessments. Among all participants, 23.03% showed mild depressive symptoms, 4.11% moderate, 0.94% moderately severe, and 0.34% severe depressive symptoms. The range, mean, and standard deviation scores are shown in .
. Sample descriptive statistics.
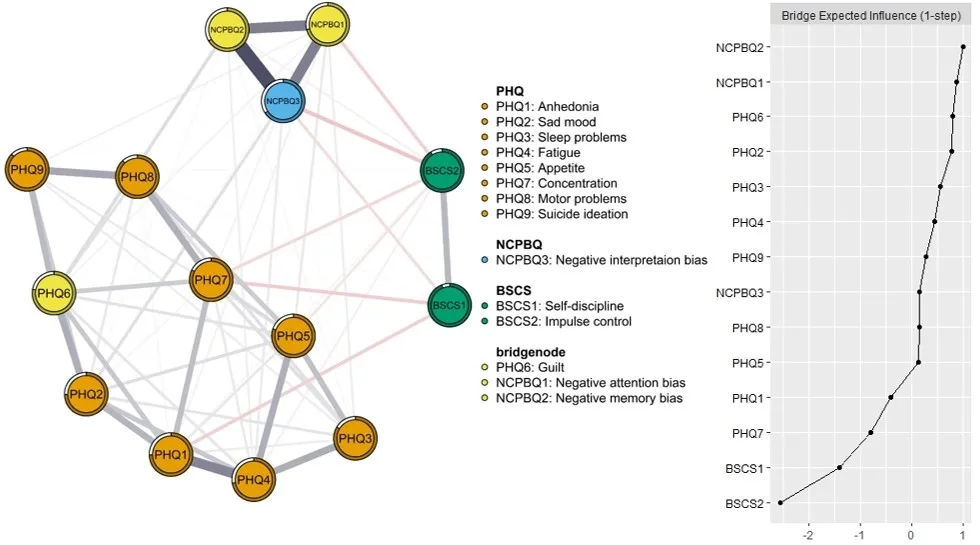
displays the network of negative cognitive processing bias, self-control, and depression. Regarding basic characteristics of the network, 65 of 91 possible edges (71.4%) were not zero, suggesting substantial interconnectivity among variables. Additionally, associations within communities were generally stronger than those between communities. Within the network, the five strongest positive relations were observed in respective communities, with three edges in the negative cognitive processing bias community, and two in the depression community.
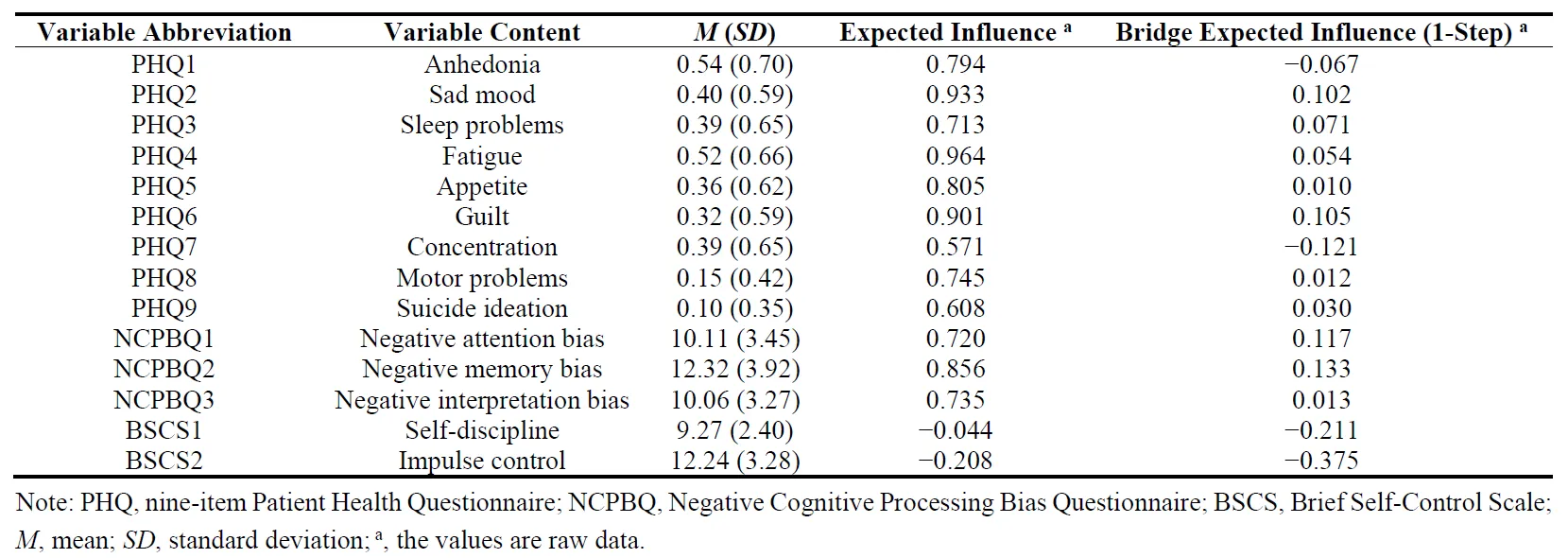
The right panel of and display the expected influences of all network nodes. The PHQ4 (“Fatigue”) had the highest EI value, followed by PHQ2 (“Sad mood”) and PHQ6 (“Guilt”), suggesting that these nodes had the most significant influence within the network model. In contrast, BSCS1 (“Self-discipline”) and BSCS2 (“Impulse control”) had negative EI values, indicating that these nodes played a role in alleviating the severity of symptoms. With regard to bridge symptoms, NCPBQ2 (“Negative memory bias”), NCPBQ1 (“Negative attention bias”), and PHQ6 (“Guilt”) had the highest BEI values (, ).
Within the network, NCPBQ2 (“Negative memory bias”) had the strongest positive correlation with NCPBQ3 (“Negative interpretation bias”), followed by the relations between NCPBQ1 (“Negative attention bias”) and NCPBQ2 (“Negative memory bias”), NCPBQ1 (“Negative attention bias”) and NCPBQ3 (“Negative interpretation bias”), PHQ1 (“Anhedonia”) and PHQ4 (“Fatigue”), as well as PHQ8 (“Motor problems”) and PHQ9 (“Suicide ideation”). Between different communities, the node PHQ6 (“Guilt”) had the most positive direct connection with NCPBQ2 (“Negative memory bias”), followed by the correlation between PHQ2 (“Sad mood”) and NCPBQ3 (“Negative interpretation bias”). The most negative edge was observed between NCPBQ3 (“Negative interpretation bias”) and BSCS2 (“Impulse control”), followed by the association between PHQ7 (“Concentration”) and BSCS1 (“Self-discipline”). In general, the NCPBQ dimensions were positively associated with the PHQ items, while the BSCS dimensions were negatively associated with the PHQ items and the NCPBQ dimensions. The edge weights matrix is shown in Supplementary Table S1.
. Estimated network model for negative cognitive processing bias, self−control, and depression. Note: The PHQ items (nine−item Patient Health Questionnaire), the NCPBQ dimensions (Negative Cognitive Processing Bias Questionnaire), and the BSCS dimensions (Brief Self−Control Scale) are represented by orange, blue, and green nodes, respectively. Grey lines indicate positive correlations, while red lines indicate negative correlations, with the edge thickness indicating the strength of the association.
. Descriptive statistics of measurement variables.
. An estimated network model for negative cognitive processing bias, self-control, and depression shows bridge nodes. Note: Grey lines indicate positive correlations, while red lines indicate negative correlations, with the edge thickness indicating the strength of the association.
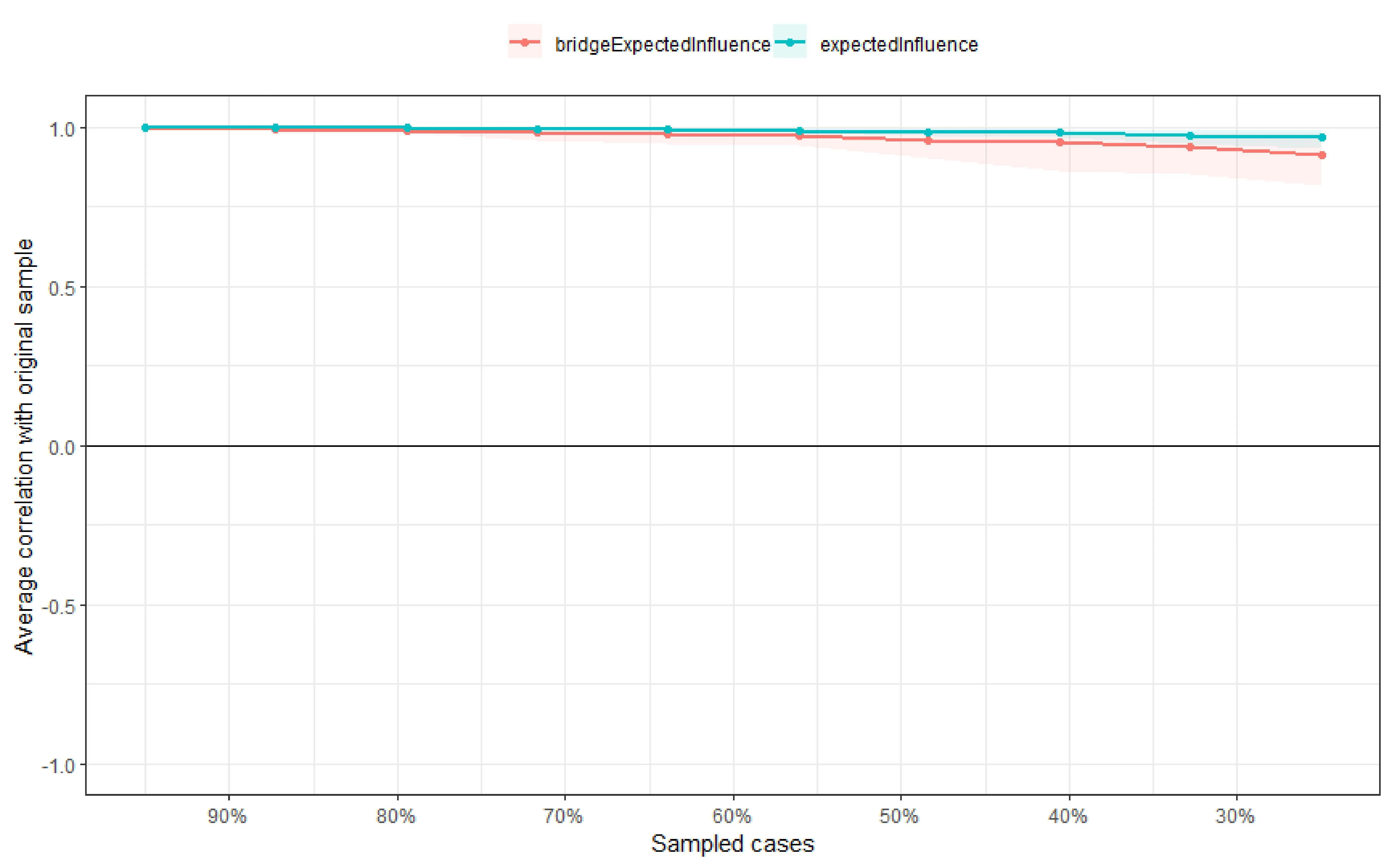
As depicted in , the EI and BEI values exhibited exceptional stability (CS-coefficient = 0.75), indicating that up to 75% of samples could be excluded without significantly affecting the network structure. The narrow bootstrapped 95% CIs of edge weights indicate the estimation of the network is accurate (Supplementary Figure S1 Panel A). The bootstrapped difference test for EI values and edges were represented in Supplementary Figure S1 Panel B and C.
. Centrality stability assessment by the case−dropping bootstrap method. Note: The <i>x</i>−axis indicates the percentage of cases sampled from the original dataset to constitute the subset dataset, while the <i>y</i>−axis represents the average correlations of centrality indices between the original network and the re−estimated networks after sampling the specified percentage of cases.
4. Discussion
This is the first study to investigate the relationships between negative cognitive processing bias, self-control, and depression based on the network analysis. By this approach, we constructed a complex network comprising different negative cognitive processing biases, self-control dimensions, and depression symptoms. Within the network, central nodes and bridge nodes that played crucial roles were identified. Additionally, distinct connections of different negative cognitive processing biases and dimensions of self-control to depression symptoms were revealed, indicating these variables are associated with depression development through specific edges. From the dual-process model, this study enhances our understanding of the psychopathological mechanism of depression at the symptom level. It also provides reference points and effective targets for the prevention and intervention of depression.
Fatigue, sad mood, and guilt of depression are central nodes within the network. This aligns with research suggesting that depression manifests across physical, emotional, and cognitive domains [
62]. Fatigue emerges as the second most frequent symptom among the nine criteria for depression in the DSM-IV classification [
63]. The somatization of distress may explain the high centrality of fatigue. In non-Western cultures, particularly in China, somatization symptoms of depression are more prevalent compared with Western countries [
64]. Some individuals with depression solely exhibit somatic symptoms, often being the primary reason for their initial hospital visits [
65]. Sad mood held significant weight within the network. It is one of the two necessary symptoms of depression diagnosis in DSM-V and ICD-11, and the hallmark symptom of depression [
66,
67]. Furthermore, guilt is one of the few repeatable factors that predict the occurrence and maintenance of depression [
68]. Research has indicated that 85% of depressed individuals report symptoms of guilt, worthlessness, and feelings of inadequacy [
69]. Guilt is associated with an attributional style of excessive self-blame, which often leads to emotions such as despair, helplessness, frustration, and depression [
70].
In the network, negative memory bias, negative attention bias, and guilt emerged as bridge nodes. Negative memory bias and attention bias are considered as critical factors in the onset and persistence of depression [
32,
71]. Memory bias demonstrates a moderate association with depression symptoms, independent of research paradigms or measurement tools [
22]. Specifically, this bias is significantly linked to cognitive-affective symptoms, including sad mood, worthlessness, suicidal ideation, and loneliness, which are considered core symptoms of depression, posing a more detrimental effect on overall depression development [
72]. Negative attention bias directs individuals’ attention toward negative information and hampers their ability to distract, which is relevant to the sustained sad mood in depressed individuals [
73]. Additionally, negative attention bias is found to be associated with rumination, which is a cognitive vulnerability factor of depression [
74]. Moreover, guilt served as a bridge node within the network. Guilt, concerning cognitive and attitudinal changes, represents another critical symptom of depression besides mood alterations [
64]. As a cognitive symptom, guilt is closely connected to the pathways of negative cognitive processing bias and self-control [
75].
Negative cognitive processing bias serves as a risk factor for depression, and all three dimensions are positively correlated with depression symptoms. Among these, negative memory bias exhibited the strongest positive association with guilt in depression across different communities. Negative memory bias reduces the difficulty of encoding and retrieving negative information [
76], particularly when it aligns with negative self-referential schemas of individuals [
77]. This tendency might add to self-blame, worthlessness, and a sense of failure, increasing guilt. A strong positive correlation was observed between negative interpretation bias and sad mood in depression. Negative interpretation bias inclines individuals to attribute negative events to internal, stable, and universal factors, leading to lower self-evaluations, and producing more negative emotions [
78]. Furthermore, this bias predisposes individuals to interpret ambiguous information negatively [
16]. Correction of negative interpretations also decreases when confronted with ambiguous positive information [
79]. Such biased and inflexible interpretations elicit sad emotional responses and difficulties in emotion regulation, thereby increasing the risk of depression [
80].
Self-control functions as a facilitating factor for depression prevention and intervention. Within the network, a strong negative correlation was found between self-discipline in self-control and the lack of concentration in depression. University students with higher levels of self-discipline tend to focus more on their studies and maintain a regular life routine [
81]. Consequently, they may experience a stronger sense of control, higher life satisfaction, and lower depression. In contrast, lower self-discipline is relevant to lower cognitive control, which is important for emotion regulation [
82]. Facing external negative information, individuals with lower self-discipline may be more susceptible due to difficulties in regulating emotion, leading to increased worry and sadness, exacerbating internalization issues [
83]. Additionally, individuals with lower self-discipline may adopt unhealthy lifestyles and often lack sufficient energy to achieve their goals [
84].
Negative cognitive processing bias and self-control antagonize each other. On one hand, negative cognitive processing bias undermines self-control, further exacerbating depression. The most substantial negative correlation was observed between negative interpretation bias and impulse control, indicating that an excessive negative interpretation bias could cause a reduction in impulse control ability [
85]. Negative interpretation bias is linked to higher levels of rumination [
86], and this detrimental cognitive style could produce lots of negative emotions. Dealing with negative emotions consumes limited cognitive resources, diminishing an individual’s impulse control [
87], prompting the use of maladaptive methods to handle emotional problems, and raising the likelihood of depression [
88]. For another, self-control could alleviate depression by reducing negative cognitive processing bias. According to Gross’s emotion regulation process model [
89], individuals exhibiting high self-control are more goal-oriented and could reduce rumination generated by negative interpretation bias through strategies like diverting attention from negative stimuli and cognitive reappraisal, thus minimizing sad emotions [
86,
90]. Additionally, higher self-control results in better inhibition and initiation abilities [
88], and assists individuals in achieving beneficial outcomes by avoiding undesirable behaviors and engaging in desired actions [
91].
This study examined the intricate network relationships among dimensions of negative cognitive processing bias, dimensions of self-control, and depressive symptoms. It revealed the specific links between the bottom-up negative cognitive processing bias to depressive symptoms and the top-down self-control to depressive symptoms, and highlighted the adversarial relationship between the dual-process model variables in the manifestation of depression. Our research offered new possible psychopathological pathways linking negative cognitive processing bias, self-control to depression. Additionally, this study provided suggestions for clinical depression identification, prevention, and intervention. Network analysis suggests that central nodes and bridge nodes may represent crucial targets, as intervention on these nodes can effectively reduce the severity of the entire network and prevent the co-occur of other disorders [
47,
61]. Our findings emphasized the significance of fatigue, sad mood, and guilt within the network, and highlighted the role of transmission of negative memory bias and negative attention bias. Employing these crucial symptoms as primary screening indicators may facilitate the timely detection of individuals at risk of depression. Furthermore, targeting these key nodes and connecting pathways may be more effective in depression prevention and intervention. Cognitive-behavioral therapy (CBT) is rapid in improving sad mood and guilt among various depression symptoms [
92], and it is one of the most effective treatments for depression. Besides, based on the confrontation of dual-process model variables, applying combined cognitive bias modification and cognitive control training simultaneously to reduce negative cognitive processing bias and improve self-control may be promising in relieving depressive symptoms [
93,
94].
Although this study explored the fine-grained relationships between negative cognitive processing bias, self-control, and depression from a dual-process perspective, offering critical information, the following limitations should be acknowledged. First, the study sample comprised university students, only part of them have mild or more severe depressive symptoms (28.4% of participants scored more than 5 points on the PHQ-9 questionnaire). Although as one of the most vulnerable groups of depression, studying the underlying relationships between depression and influencing factors is significant, caution is necessary in extending these findings to other age groups or clinically diagnosed depressed patients. Second, the cross-sectional design limits the ability to confirm causal relationships between variables. In the future, longitudinal analysis and experimental methods are warranted to validate the model constructed and assess the effect of interventions targeting central symptoms and bridge symptoms for depression. Third, we used a self-report method to collect data, which may result in participants’ responses being influenced by social desirability effects and subjective biases, contributing to the lower reliability of the study. A more objective method to measure data should be considered for future studies. Fourth, in the present study, the network is specific to the scales we applied. There are other scales that can be used to measure depression, negative cognitive processing bias, and self-control, and the dimensions of these scales may also be different. This suggests that the network structure of the study may only partially indicate the relationships between the three variables. Although the scales we selected have good reliability and validity, the NCPBQ is a relatively new questionnaire, which may partially limit the comparability of the results.
5. Conclusions
The present study revealed specific pathways linking negative cognitive processing bias and self-control to depression at a fine-grained level, highlighted the antagonistic effect of the dual-process model variables in depression, and identified crucial nodes for depression development. These findings offered probably psychopathology of depression and provided evidence for identification, prevention and intervention of depression. For university teachers, paying attention to indicators such as fatigue, sad mood, guilt, negative attention bias, and negative memory bias is conducive to the early depression identification of students and the conduction of subsequent mental work. For patients, actively focusing on and adjusting negative emotions and cognitive styles promptly can help reduce the risk of depression and aid in its prevention. For clinicians, it is recommended to target crucial nodes and intervene from the dual-process perspective to achieve optimal results.
Supplementary Materials
The following supporting information can be found at: https://www.sciepublish.com/article/pii/288, Figure S1. Nonparametric bootstrapped difference test; Table S1. Edge weights matrix of negative cognitive processing bias, self-control, and depression network.
Statement of the Use of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this manuscript, the authors used ChatGPT in order to improve the readability of language. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Acknowledgments
The authors acknowledge all participants in this study.
Author Contributions
Conceptualization, S.L., J.G., Q.L. and B.D.; Methodology, S.L. and B.D.; Software, S.L.; Validation, S.L., J.G.; Formal analysis, S.L.; Resources, B.D.; Data Curation, J.G. and G.Z.; Writing—Original Draft, S.L.; Writing—Review & Editing, S.L., J.G., Q.L., G.Z., J.C. and B.D.; Visualization, S.L.; Supervision, B.D.; Project administration, Q.L. and B.D.; Funding acquisition, B.D.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Tianjin Medical University (study number: TMuhMEC2022019) on 19 May 2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Funding
This research was funded by the 2021 Tianjin Municipal Education Commission Scientific Research Plan Special Task Project (Mental Health Education) Key Project (Grant Number: 2021ZDGX08).
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
1.
Institute for Health Metrics and Evaluation. Global Health Data Exchange (GHDx). 2023. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 4 March 2023).
-
2.
Liu X-Q, Guo Y-X, Zhang W-J, Gao W-J. Influencing factors, prediction and prevention of depression in college students: A literature review.
World J. Psychiatry 2022,
12, 860.
[Google Scholar]
-
3.
Fu X, Zhang K, Chen X, Chen Z. Report on National Mental Health Development in China (2021–2022); Social Sciences Academic Press (China): Beijing, China, 2023.
-
4.
Gao L, Xie Y, Jia C, Wang W. Prevalence of depression among Chinese university students: A systematic review and meta-analysis.
Sci. Rep. 2020,
10, 15897.
[Google Scholar]
-
5.
Awadalla S, Davies EB, Glazebrook C. A longitudinal cohort study to explore the relationship between depression, anxiety and academic performance among Emirati university students.
BMC Psychiatry 2020,
20, 1–10.
[Google Scholar]
-
6.
Deroma VM, Leach JB, Leverett JP. The relationship between depression and college academic performance.
Coll. Stud. J. 2009,
43, 325–335.
[Google Scholar]
-
7.
Chen T, Lucock M. The mental health of university students during the COVID-19 pandemic: An online survey in the UK.
PLoS One 2022,
17, e0262562.
[Google Scholar]
-
8.
Cai H, Bai W, Liu H, Chen X, Qi H, Liu R, et al. Network analysis of depressive and anxiety symptoms in adolescents during the later stage of the COVID-19 pandemic.
Transl. Psychiatry 2022,
12, 98.
[Google Scholar]
-
9.
Casey SM, Varela A, Marriott JP, Coleman CM, Harlow BL. The influence of diagnosed mental health conditions and symptoms of depression and/or anxiety on suicide ideation, plan, and attempt among college students: Findings from the Healthy Minds Study, 2018–2019.
J. Affect. Disord. 2022,
298, 464–471.
[Google Scholar]
-
10.
Phillips WJ, Hine DW. Exploring the factor structure of implicit and explicit cognitions associated with depression.
Assessment 2013,
20, 474–483.
[Google Scholar]
-
11.
Van Bockstaele B, Tibboel H, Larsen H, Wiers RW, Bögels SM, Salemink E. Dual processes in fear and anxiety: No effects of cognitive load on the predictive value of implicit measures.
Cogn. Emot. 2021,
35, 859–873.
[Google Scholar]
-
12.
Weil R, Feist A, Moritz S, Wittekind CE. Approaching contamination-related stimuli with an implicit Approach-Avoidance Task: Can it reduce OCD symptoms? An online pilot study.
J. Behav. Ther. Exp. Psychiatry 2017,
57, 180–188.
[Google Scholar]
-
13.
Carver CS, Johnson SL, Joormann J. Serotonergic function, two-mode models of self-regulation, and vulnerability to depression: What depression has in common with impulsive aggression.
Psychol. Bull. 2008,
134, 912–943.
[Google Scholar]
-
14.
Strack F, Deutsch R. Reflective and impulsive determinants of social behavior.
Pers. Soc. Psychol. Rev. 2004,
8, 220–247.
[Google Scholar]
-
15.
Beevers CG. Cognitive vulnerability to depression: A dual process model.
Clin. Psychol. Rev. 2005,
25, 975–1002.
[Google Scholar]
-
16.
Beck AT, Haigh EA. Advances in cognitive theory and therapy: The generic cognitive model.
Annu. Rev. Clin. Psychol. 2014,
10, 1–24.
[Google Scholar]
-
17.
Clark DA, Beck AT, Alford BA, Bieling PJ, Segal ZV. Scientific foundations of cognitive theory and therapy of depression.
J. Cogn. Psychother. 2000,
14, 100–106.
[Google Scholar]
-
18.
Mogg K, Bradbury KE, Bradley BP. Interpretation of ambiguous information in clinical depression.
Behav. Res. Ther. 2006,
44, 1411–1419.
[Google Scholar]
-
19.
Hofmann W, Friese M, Strack F. Impulse and self-control from a dual-systems perspective. Perspect.
Psychol. Sci. 2009,
4, 162–176.
[Google Scholar]
-
20.
Gotlib IH, Joormann J. Cognition and depression: Current status and future directions.
Annu. Rev. Clin. Psychol. 2010,
6, 285–312.
[Google Scholar]
-
21.
Mathews A, MacLeod C. Cognitive vulnerability to emotional disorders.
Annu. Rev. Clin. Psychol. 2005,
1, 167–195.
[Google Scholar]
-
22.
LeMoult J, Gotlib IH. Depression: A cognitive perspective.
Clin. Psychol. Rev. 2019,
69, 51–66.
[Google Scholar]
-
23.
LeMoult J, Kircanski K, Prasad G, Gotlib IH. Negative self-referential processing predicts the recurrence of major depressive episodes.
Clin. Psychol. Sci. 2017,
5, 174–181.
[Google Scholar]
-
24.
Platt B, Sfärlea A, Löchner J, Salemink E, Schulte-Körne G. The role of cognitive biases and negative life events in predicting later depressive symptoms in children and adolescents.
J. Exp. Psychopathol. 2023,
14, 20438087231184753.
[Google Scholar]
-
25.
Platt B, Waters AM, Schulte-Koerne G, Engelmann L, Salemink E. A review of cognitive biases in youth depression: Attention, interpretation and memory.
Cogn. Emot. 2017,
31, 462–483.
[Google Scholar]
-
26.
Duyser F, Van Eijndhoven P, Bergman M, Collard R, Schene A, Tendolkar I, et al. Negative memory bias as a transdiagnostic cognitive marker for depression symptom severity.
J. Affect. Disord. 2020,
274, 1165–1172.
[Google Scholar]
-
27.
Marchetti I, Everaert J, Dainer-Best J, Loeys T, Beevers CG, Koster EH. Specificity and overlap of attention and memory biases in depression.
J. Affect. Disord. 2018,
225, 404–412.
[Google Scholar]
-
28.
Orchard F, Pass L, Reynolds S. Associations between interpretation bias and depression in adolescents.
Cogn. Ther. Res. 2016,
40, 577–583.
[Google Scholar]
-
29.
Lee J-S, Mathews A, Shergill S, Yiend J. Magnitude of negative interpretation bias depends on severity of depression.
Behav. Res. Ther. 2016,
83, 26–34.
[Google Scholar]
-
30.
Beevers CG, Mullarkey MC, Dainer-Best J, Stewart RA, Labrada J, Allen JJ, et al. Association between negative cognitive bias and depression: A symptom-level approach.
J. Abnorm. Psychol. 2019,
128, 212–227.
[Google Scholar]
-
31.
Lichtenstein-Vidne L, Okon-Singer H, Cohen N, Todder D, Aue T, Nemets B, et al. Attentional bias in clinical depression and anxiety: The impact of emotional and non-emotional distracting information.
Biol. Psychol. 2017,
122, 4–12.
[Google Scholar]
-
32.
Disner SG, Shumake JD, Beevers CG. Self-referential schemas and attentional bias predict severity and naturalistic course of depression symptoms.
Cogn. Emot. 2017,
31, 632–644.
[Google Scholar]
-
33.
Tangney JP, Baumeister RF, Boone AL. High Self-Control Predicts Good Adjustment, Less Pathology, Better Grades, and Interpersonal Success.
J. Pers. 2004,
72, 271–324.
[Google Scholar]
-
34.
Geng Y, Gu J, Wang J, Zhang R. Smartphone addiction and depression, anxiety: The role of bedtime procrastination and self-control.
J. Affect. Disord. 2021,
293, 415–421.
[Google Scholar]
-
35.
DeWall CN, Gilman R, Sharif V, Carboni I, Rice KG. Left out, sluggardly, and blue: Low self-control mediates the relationship between ostracism and depression.
Pers. Individ. Differ. 2012,
53, 832–837.
[Google Scholar]
-
36.
Nie Y-G, Li J-B, Dou K, Situ Q-M. The associations between self-consciousness and internalizing/externalizing problems among Chinese adolescents.
J. Adolesc. 2014,
37, 505–514.
[Google Scholar]
-
37.
Unger A, Bi C, Xiao YY, Ybarra O. The revising of the Tangney Self-control Scale for Chinese students.
PsyCh J. 2016,
5, 101–116.
[Google Scholar]
-
38.
Yang X, Zhao J, Chen Y, Zu S, Zhao J. Comprehensive self-control training benefits depressed college students: A six-month randomized controlled intervention trial.
J. Affect. Disord. 2018,
226, 251–260.
[Google Scholar]
-
39.
Zeidi IM, Divsalar S, Morshedi H, Alizadeh H. The effectiveness of group cognitive-behavioral therapy on general self-efficacy, self-control, and internet addiction prevalence among medical university students.
Asian J. Soc. Health Behav. 2020,
3, 93–102.
[Google Scholar]
-
40.
Strauman TJ, Vieth AZ, Merrill KA, Kolden GG, Woods TE, Klein MH, et al. Self-system therapy as an intervention for self-regulatory dysfunction in depression: A randomized comparison with cognitive therapy.
J. Consult. Clin. Psychol. 2006,
74, 367–376.
[Google Scholar]
-
41.
Watkins ER, Roberts H. Reflecting on rumination: Consequences, causes, mechanisms and treatment of rumination.
Behav. Res. Ther. 2020,
127, 103573.
[Google Scholar]
-
42.
Sinha R. Modeling stress and drug craving in the laboratory: Implications for addiction treatment development.
Addict. Biol. 2009,
14, 84–98.
[Google Scholar]
-
43.
Ward A, Mann T. Don’t mind if I do: Disinhibited eating under cognitive load.
J. Pers. Soc. Psychol. 2000,
78, 753–763.
[Google Scholar]
-
44.
Fried EI, Epskamp S, Nesse RM, Tuerlinckx F, Borsboom D. What are’good’depression symptoms? Comparing the centrality of DSM and non-DSM symptoms of depression in a network analysis.
J. Affect. Disord. 2016,
189, 314–320.
[Google Scholar]
-
45.
Fried EI, Nesse RM. Depression sum-scores don’t add up: Why analyzing specific depression symptoms is essential.
BMC Med. 2015,
13, 1–11.
[Google Scholar]
-
46.
Borsboom D. A network theory of mental disorders.
World Psychiatry 2017,
16, 5–13.
[Google Scholar]
-
47.
Borsboom D, Cramer AO. Network analysis: An integrative approach to the structure of psychopathology.
Annu. Rev. Clin. Psychol. 2013,
9, 91–121.
[Google Scholar]
-
48.
McNally RJ, Robinaugh DJ, Wu GW, Wang L, Deserno MK, Borsboom D. Mental disorders as causal systems: A network approach to posttraumatic stress disorder.
Clin. Psychol. Sci. 2015,
3, 836–849.
[Google Scholar]
-
49.
Bringmann LF, Eronen MI. Don’t blame the model: Reconsidering the network approach to psychopathology.
Psychol. Rev. 2018,
125, 606–615.
[Google Scholar]
-
50.
Robinaugh DJ, Millner AJ, McNally RJ. Identifying highly influential nodes in the complicated grief network.
J. Abnorm. Psychol. 2016,
125, 747–757.
[Google Scholar]
-
51.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: Validity of a brief depression severity measure.
J. Gen. Intern. Med. 2001,
16, 606–613.
[Google Scholar]
-
52.
Zhang YL, Liang W, Chen ZM, Zhang HM, Zhang JH, Weng XQ, et al. Validity and reliability of Patient Health Q uestionnaire-9 and Patient Health Q uestionnaire-2 to screen for depression among college students in China.
Asia-Pac. Psychiatry 2013,
5, 268–275.
[Google Scholar]
-
53.
Hou X, Lai X, Lin Y, Cao L, Zhong B, Zheng Y, et al. Influence of neuroticism on depression among college students by gender: The mediating roles of negative cognitive bias and anhedonia.
Curr. Psychol. 2024,
43, 5901–5913.
[Google Scholar]
-
54.
Yan X, Zhang R, Feng Z. Development of negative cognitive processing bias questionnaire.
Mil. Med. Univ. 2017,
39, 2329–2334.
[Google Scholar]
-
55.
Luo T, Cheng L, Qin L, Xiao S. Reliability and validity of Chinese version of brief self-control scale.
Chin. J. Clin. Psychol. 2021,
29, 83–86.
[Google Scholar]
-
56.
R Core Team. R: A Language and Environment for Statistical Computing. In R Foundation for Statistical Computing. 2013. Available online: https://www.Rproject.org/ (accessed on 13 March 2023).
-
57.
Friedman J, Hastie T, Tibshirani R. Sparse inverse covariance estimation with the graphical lasso.
Biostatistics 2008,
9, 432–441.
[Google Scholar]
-
58.
Chen J, Chen Z. Extended Bayesian information criteria for model selection with large model spaces.
Biometrika 2008,
95, 759–771.
[Google Scholar]
-
59.
Epskamp S, Cramer AO, Waldorp LJ, Schmittmann VD, Borsboom D. qgraph: Network visualizations of relationships in psychometric data.
J. Stat. Softw. 2012,
48, 1–18.
[Google Scholar]
-
60.
Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: A tutorial paper.
Behav. Res. Methods 2018,
50, 195–212.
[Google Scholar]
-
61.
Jones PJ, Ma R, McNally RJ. Bridge centrality: A network approach to understanding comorbidity.
Multivar. Behav. Res. 2021,
56, 353–367.
[Google Scholar]
-
62.
Liang K, Chen S, Zhao Y, Ren Y, Ren Z, Chi X. A new PHQ-2 for Chinese adolescents: Identifying core items of the PHQ-9 by network analysis.
Child Adolesc. Psychiatry Ment. Health 2023,
17, 11.
[Google Scholar]
-
63.
Zimmerman M, Ellison W, Young D, Chelminski I, Dalrymple K. How many different ways do patients meet the diagnostic criteria for major depressive disorder?
Compr. Psychiatry 2015,
56, 29–34.
[Google Scholar]
-
64.
Kendler KS. The phenomenology of major depression and the representativeness and nature of DSM criteria.
Am. J. Psychiatry 2016,
173, 771–780.
[Google Scholar]
-
65.
Kapfhammer H-P. Somatic symptoms in depression.
Dialogues Clin. Neurosci. 2006,
8, 227–239.
[Google Scholar]
-
66.
APA. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5) (Vol. 5); American Psychiatric Association: Washington, DC, USA, 2013.
-
67.
WHO. International Statistical Classification of Diseases and Related Health Problems, 11th Revision; World Health Organization: Geneva, Switzerland, 2019.
-
68.
Hards E, Ellis J, Fisk J, Reynolds S. Negative view of the self and symptoms of depression in adolescents.
J. Affect. Disord. 2020,
262, 143–148.
[Google Scholar]
-
69.
Zahn R, Lythe KE, Gethin JA, Green S, Deakin JFW, Young AH, et al. The role of self-blame and worthlessness in the psychopathology of major depressive disorder.
J. Affect. Disord. 2015,
186, 337–341.
[Google Scholar]
-
70.
Harrison P, Lawrence AJ, Wang S, Liu S, Xie G, Yang X, et al. The psychopathology of worthlessness in depression.
Front. Psychiatry 2022,
13, 818542.
[Google Scholar]
-
71.
Beevers CG, Clasen PC, Enock PM, Schnyer DM. Attention bias modification for major depressive disorder: Effects on attention bias, resting state connectivity, and symptom change.
J. Abnorm. Psychol. 2015,
124, 463–475.
[Google Scholar]
-
72.
Fried EI, Nesse RM. The impact of individual depressive symptoms on impairment of psychosocial functioning.
PLoS One 2014,
9, e90311.
[Google Scholar]
-
73.
Clasen PC, Wells TT, Ellis AJ, Beevers CG. Attentional biases and the persistence of sad mood in major depressive disorder.
J. Abnorm. Psychol. 2013,
122, 74–85.
[Google Scholar]
-
74.
Kaiser RH, Snyder HR, Goer F, Clegg R, Ironside M, Pizzagalli DA. Attention bias in rumination and depression: Cognitive mechanisms and brain networks.
Clin. Psychol. Sci. 2018,
6, 765–782.
[Google Scholar]
-
75.
Beck AT, Bredemeier K. A unified model of depression: Integrating clinical, cognitive, biological, and evolutionary perspectives.
Clin. Psychol. Sci. 2016,
4, 596–619.
[Google Scholar]
-
76.
Del Valle C, Mateos P. Implicit mood congruent memory bias in subclinical depression.
Int. J. Cogn. Ther. 2018,
11, 287–298.
[Google Scholar]
-
77.
Benau EM, Hill KE, Atchley RA, O’Hare AJ, Gibson LJ, Hajcak G, et al. Increased neural sensitivity to self-relevant stimuli in major depressive disorder.
Psychophysiology 2019,
56, e13345.
[Google Scholar]
-
78.
Orchard F, Reynolds S. The combined influence of cognitions in adolescent depression: Biases of interpretation, self-evaluation, and memory.
Br. J. Clin. Psychol. 2018,
57, 420–435.
[Google Scholar]
-
79.
Everaert J, Bronstein MV, Cannon TD, Joormann J. Looking through tinted glasses: Depression and social anxiety are related to both interpretation biases and inflexible negative interpretations.
Clin. Psychol. Sci. 2018,
6, 517–528.
[Google Scholar]
-
80.
Mehu M, Scherer KR. The appraisal bias model of cognitive vulnerability to depression.
Emot. Rev. 2015,
7, 272–279.
[Google Scholar]
-
81.
Gorbunovs A, Kapenieks A, Cakula S. Self-discipline as a key indicator to improve learning outcomes in e-learning environment.
Procedia. Soc. Behav. Sci. 2016,
231, 256–262.
[Google Scholar]
-
82.
Olatunji BO, Knowles KA, Adamis AM, Cole DA. Linking a latent variable trait-state-occasion model of emotion regulation to cognitive control.
Cogn. Emot. 2024,
38, 898–912.
[Google Scholar]
-
83.
Haukaas RB, Gjerde IB, Varting G, Hallan HE, Solem S. A randomized controlled trial comparing the attention training technique and mindful self-compassion for students with symptoms of depression and anxiety.
Front. Psychol. 2018,
9, 827.
[Google Scholar]
-
84.
Raynor DA, Levine H. Associations between the five-factor model of personality and health behaviors among college students.
J. Am. Coll. Health 2009,
58, 73–82.
[Google Scholar]
-
85.
Kotelnikova Y, Mackrell SV, Jordan PL, Hayden EP. Longitudinal associations between reactive and regulatory temperament traits and depressive symptoms in middle childhood.
J. Clin. Child Adolesc. Psychol. 2015,
44, 775–786.
[Google Scholar]
-
86.
Everaert J. Interpretation of ambiguity in depression.
Curr. Opin. Psychol. 2021,
41, 9–14.
[Google Scholar]
-
87.
Alquist J, Baumeister RF. Self-control: Limited resources and extensive benefits. Wiley Interdiscip.
Rev. Cogn. Sci. 2012,
3, 419–423.
[Google Scholar]
-
88.
Li J-B, Delvecchio E, Lis A, Nie Y-G, Di Riso D. Positive coping as mediator between self-control and life satisfaction: Evidence from two Chinese samples.
Pers. Individ. Differ. 2016,
97, 130–133.
[Google Scholar]
-
89.
Gross JJ. Emotion regulation: Current status and future prospects.
Psychol. Inq. 2015,
26, 1–26.
[Google Scholar]
-
90.
Raines EM, Viana AG, Trent ES, Woodward EC, Candelari AE, Zvolensky MJ, et al. Effortful control, interpretation biases, and child anxiety symptom severity in a sample of children with anxiety disorders.
J. Anxiety Disord. 2019,
67, 102136.
[Google Scholar]
-
91.
de Ridder DT, de Boer BJ, Lugtig P, Bakker AB, van Hooft EA. Not doing bad things is not equivalent to doing the right thing: Distinguishing between inhibitory and initiatory self-control.
Pers. Individ. Differ. 2011,
50, 1006–1011.
[Google Scholar]
-
92.
Bauer-Staeb C, Griffith E, Faraway JJ, Button KS. Trajectories of depression and generalised anxiety symptoms over the course of cognitive behaviour therapy in primary care: An observational, retrospective cohort.
Psychol. Med. 2023,
53, 4648–4656.
[Google Scholar]
-
93.
Everaert J, Bernstein A, Joormann J, Koster EH. Mapping dynamic interactions among cognitive biases in depression.
Emot. Rev. 2020,
12, 93–110.
[Google Scholar]
-
94.
Hoorelbeke K, Van den Bergh N, De Raedt R, Wichers M, Koster EH. Preventing recurrence of depression: Long-term effects of a randomized controlled trial on cognitive control training for remitted depressed patients.
Clin. Psychol. Sci. 2021,
9, 615–633.
[Google Scholar]