1. Introduction
Forensic odontology involves the correct collection, management, interpretation, evaluation, and presentation of dental evidence for criminal or civil legal proceedings [
1]. It includes a broad range of components that play a significant role in the investigation of cases involving decedent or living individuals, including dental age estimation, personal identification, human abuse and neglect, bitemark examination and civil litigation [
2]. Among all these aspects, the core component of forensic odontology is the identification of human remains.
The process of identification of unknown remains generally starts with the reconstruction of the skeletal biological profile, which consists of the estimation of the individual’s ancestry, sex, age-at-death, and stature. The results of the biological profile analysis provide a general description of the individual that is used to narrow down the candidates for the identity [
3]. Although some dental traits can be informative for ancestry estimation, the most significant contribution of forensic odontology for the biological profile is without a doubt dental age estimation. Dental methods of age estimation are of particular value in cases of juvenile remains, since dental age estimation based on tooth formation and development is the most reliable means of skeletal age assessment. Additionally, dental age estimation based on post-formation changes can offer informative data in cases involving adults [
4].
Once one or more candidates are given for the identity, forensic odontologists conduct the comparison between the antemortem and postmortem records. This consists of objectively identifying areas of consistency and inconsistency, and analyzing the inconsistencies found in order to establish if they are irreconcilable (meaning that the antemortem and postmortem data sets do not correspond to the same individual) or if they are reconcilable (does not exclude an antemortem data set as a match to the postmortem data set). Evaluation of the consistencies and inconsistencies shown in the antemortem, and postmortem data sets will lead to the expert’s opinion on the identification of the remains.
This article focuses on the forensic odontological analyses that can be conducted to compare the antemortem and postmortem data sets and their relevance to the identification of human remains.
2. Postmortem Data Collection and Analysis
The goal of the postmortem data collection and analysis is to create a postmortem profile that establishes the dental condition of the decedent at the time of death [
2] for comparison to the antemortem records.
First, an overall observation of the dental and maxillofacial structures of the remains gives a general idea in respect of the age group of the individual (juvenile or adult), any dental treatment or pathology present in the recovered dentition, the condition of the remains in terms of fragmentation and preservation and any other major observation. All these preliminary observations provide the basis for the proper approach of the case. Photographic and radiographic documentation are essential parts of the postmortem examination. Dental photographs should show the maxillary and mandibular dentition in anterior, both laterals, occlusal and lingual views, along with any detail that should be considered in the postmortem analysis. Postmortem dental radiographs consist of periapical radiographs of all maxillary and mandibular dentition. Even edentulous areas should be radiographed in case any particular trait is observed in the internal structure of the maxillary bone or mandible. Using the results of the visual and radiographic examination of the dentition, the forensic odontologist creates the postmortem odontogram.
Information pertinent to identification, that should be recorded in the postmortem examination includes: the teeth present and missing, stating if the missing ones were lost antemortem or postmortem; the type of dental occlusion; the dental arches shape and teeth alignment; the presence of antemortem trauma or surgery; any dental or maxillofacial pathological conditions; morphology, location and materials of dental treatment, dentures and any other fixed or removable appliances (such as orthodontic treatment, dental implants, partial dentures, fixed crowns and bridges, etc.) [
1,
5]. Apart from postmortem photographs and radiographs, other imaging techniques can be applied to the remains such as Computed Tomography (CT) or surface scans. However, this is guided by the type of antemortem records provided for the case and the accessibility to the technology in question. Postmortem loss of teeth, exposure to fire or certain chemicals all can impair the preservation of dental evidence. However, the dentition is resilient to all stages of decomposition and most environmental agents. This resilience to postmortem changes is a clear advantage of using teeth as evidence for the identification of human remains.
3. Antemortem Data Collection and Analysis
The goal of the antemortem data collection and analysis is to reconstruct the latest dental condition that can be extracted from the records. The antemortem data can be presented in many forms including written dental records and clinical charting, photographs, radiographs, dental CT scans and surface scans of the dentition [
5,
6,
7,
8]. Other medical imaging techniques may include regions of the dentition; however, in most cases, teeth are poorly represented due to overlapping and superimposition artifacts [
2,
7]. With this, it is very difficult to determine the location and shape of the restorations present or distinguish the anatomical morphology of the crowns and roots.
Written dental records are among the least useful of all dental records since they are considered a subjective record interpreted by a dentist during examination, treatment, or by a scribe during transcription. Forensic odontologists often receive written dental records that are poorly documented, incomplete, or difficult to understand [
2,
9,
10,
11]. Though dental radiographs are still the gold standard antemortem dental record, other forms of antemortem data can be useful in the identification process such as photographs, dental casts, retainers and aligners, or mouthguards [
2,
12]. Although clinical photographs consist of an objective record, they only offer information about the crowns and the surfaces that are visible in the image.
The antemortem data with valuable information for the comparison include all items recorded in the postmortem examination: teeth present and missing, type of occlusion, arches shape and teeth alignment, evidence of trauma or surgery, dental treatment, dentures and appliances. However, depending on the type of record, only some of them can be extracted from the antemortem records. For instance, mouthguards can offer information about the teeth present and absent, the arch shape, and teeth alignment, but they do not give any information about restorations present or root canal treatment among others. So, the value of antemortem data depends on the nature of the antemortem records provided, making an accurate dental radiological image the most valuable resource due to its objectivity and the amount of information contained in it.
4. Postmortem vs. Antemortem Comparison
As previously mentioned in this article, the postmortem vs. the antemortem data comparison implies the evaluation of the consistencies and inconsistencies found in the data sets. This comparison is highly affected by the quality and completeness of the antemortem records, as well as the condition of the remains. The postmortem and antemortem odontograms and radiographs should be compared tooth-by-tooth [
7], evaluating all the similarities and inconsistencies, and assessing whether these inconsistencies are reconcilable or irreconcilable.
The principles of postmortem vs. antemortem odontological comparison are based on the differences in the dental and maxillofacial structures due to human variation, development and pathology, and the alteration caused by dental treatment, which can be visually and radiographically observed [
6,
7,
12]. As such, the individual’s dentition changes throughout life. However, the changes are unidirectional [
13], meaning that there are no reversals; this progressive change is fundamental to consider forensic odontology a reliable means of human identification.
A match consists of several concordances between the postmortem and antemortem records. A restoration present in both data sets located in the same tooth, covering the same surfaces, and of the same restorative material represents a match (). A reconcilable inconsistency consists of a discrepancy between the postmortem and antemortem records that may be explained by dental development or postformation changes, orodental disease and dental loss, new dental treatment or extension of a preexisting one, and skeletal trauma or surgery (). Essentially, a reconcilable inconsistency will include all changes in the dentition that are plausible to have happened between the date in which the antemortem radiograph (or other record) was taken and the date in which the remains were found [
5,
6,
8]. Reconcilable inconsistencies do not exclude the postmortem and antemortem records from corresponding to the same individual. An irreconcilable inconsistency includes any discrepancy between the postmortem and antemortem records that is not possible to occur (). Tooth development and postformation changes are unidirectional, so the postmortem data cannot show an earlier stage of development for the same individual; a tooth presenting caries or a restoration cannot appear as healthy and not restored in the postmortem. Only one irreconcilable discrepancy is enough to exclude the antemortem and postmortem datasets from corresponding to the same individual.
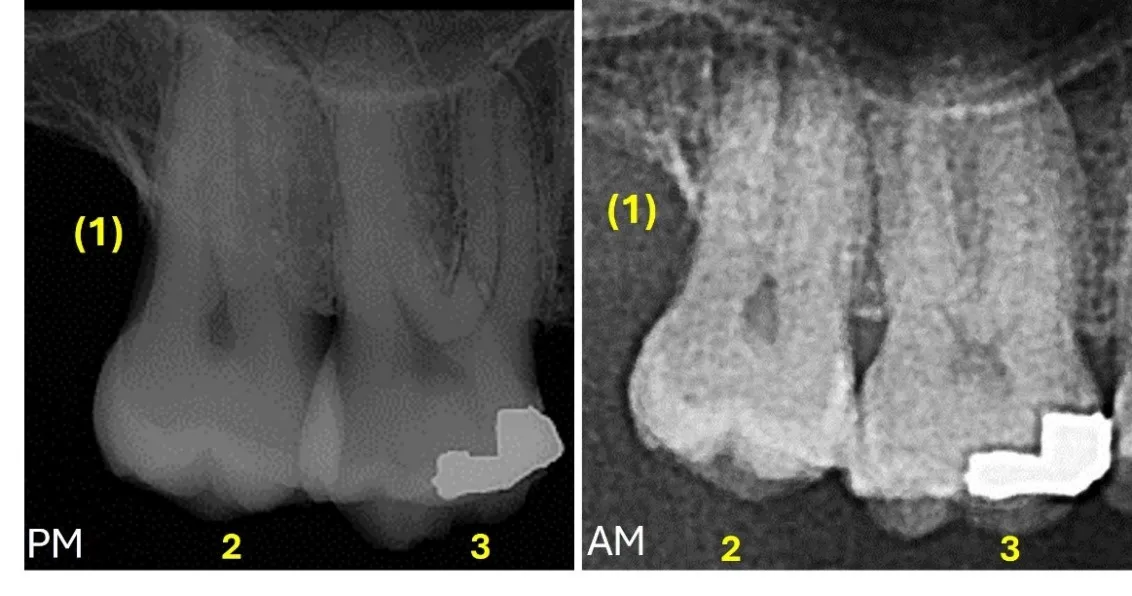
Figure 1. Postmortem radiograph (PM) and antemortem (AM) radiograph where the consistencies are noted: #1 is missing antemortem (concordant characteristic), #2 is present and not restored (concordant tooth), #3 presents an occluso-mesial amalgam restoration (concordant feature), the shape of the sinus floor (concordant characteristic). Moreover, both #2 and 3 present consistent morphology of crowns, roots and pulp cavities (concordant features) (Universal Dental Numbering System).
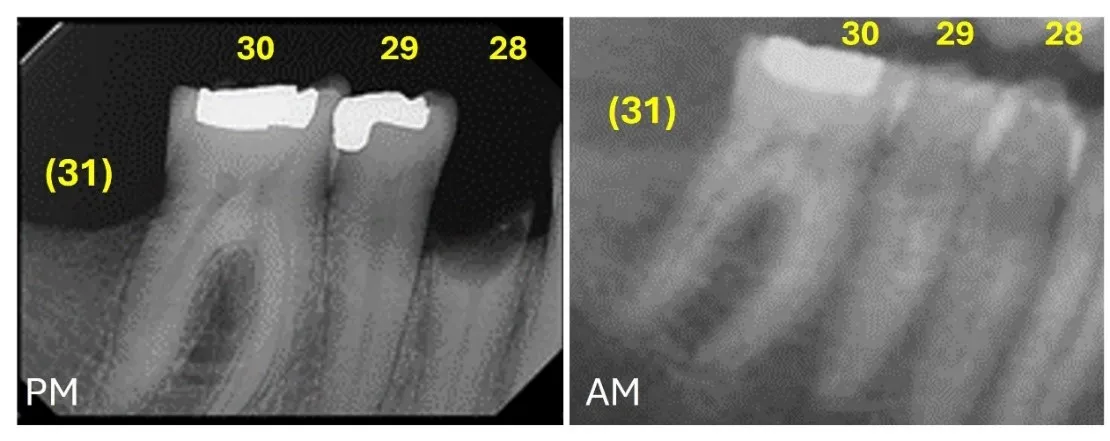
. Postmortem radiograph (PM) where #29 shows a disto-occlusal amalgam restoration and #28 shows only a root fragment present. Antemortem (AM) radiograph where #29 and 28 appear present and not restored (both reconcilable inconsistencies (Universal Dental Numbering System).
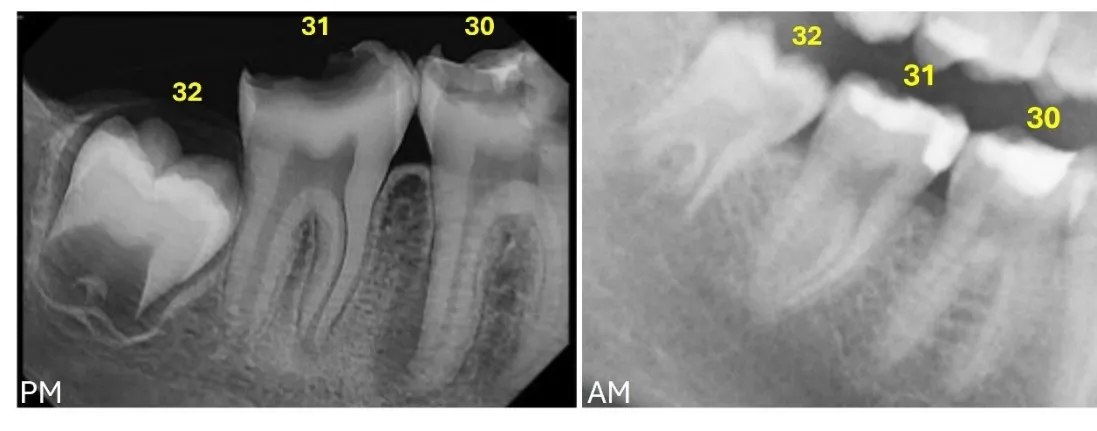
. Postmortem radiograph (PM) where #32 shows the initial formation of the bifurcation presenting a semilunar shape, whereas the antemortem (AM) radiograph shows #32 in a more advanced developmental stage, with a more extensive root bifurcation, the longer roots with divergent distal root canals (irreconcilable inconsistency) (Universal Dental Numbering System).
Consistencies found between the postmortem and antemortem records can represent dental treatment, dental anatomy, pathological signs and anatomical variations in the associated structures. Thus, a consistency between the postmortem and antemortem records can be defined at multiple levels.
A concordant feature describes any single characteristic of a tooth, restoration, associated anatomical structure or pathological process that has an individually distinct, biometrically measurable or describable characteristic, such as a caries or a restoration on a tooth. A concordant tooth describes a tooth matching in the postmortem and antemortem data sets, such that if a tooth with a restoration is found to be matching in both data sets, the consistency will still represent a concordant tooth. A concordant characteristic describes any physiological, anatomical or pathological feature external to the tooth that has distinct concordant features, such as a periapical cyst, amalgam tattoo, extraction socket or trabecular bone pattern, among others [
14,
15].
5. Features and Characteristics to Compare
The value or weight of a consistent feature in both data sets (postmortem and antemortem) depends on the level of individuality of that particular feature; meaning that the most valuable features are those that are entirely unique to an individual. Therefore, they cannot be found in the population or the probability of finding them in another individual is very low. In most cases, the level of individuality of a trait is based on the expert’s knowledge.
(a) Restorative dental treatment: Generally, the most valuable features to compare between the postmortem and antemortem data sets is dental treatment [
2,
5,
7]. Dental restorations, root canal treatment, crowns, bridges and veneers are made specifically for each patient. The location, material and morphology of the treatment are the main characteristics to compare between the antemortem and postmortem records.
(b) Osseointegrated dental implants: Although dental implant companies may not label their products, antemortem imaging is recoded post-operation in most cases. The radiological images of the implants provide highly valuable information for the antemortem-postmortem comparison [
16].
(c) Fixed orthodontic appliances: The material, shape and size of fixed orthodontic appliances vary between manufacturer’s and even within the different products of a manufacturer. Additionally, the location of the brackets in the dentition and the presence of ligatures and wire covers can provide useful information for the identification process [
7].
(d) Dentures and other removable dental appliances: Complete and partial dentures, even though they are designed for each patient and may be labelled in some cases, are removable appliances, so the first step should be to check if the denture fits in the individual’s maxillary and mandibular arches. Of all the removable dental appliances, metal-framed partial dentures provide the most distinctive information [
8].
In some cases, complete or partial dentures are labelled with the patient’s information. Several methods of denture labeling have been explored from inserting a metal band, computer-printed microlabeling the patient’s data in the acrylic, bar code or QR code, or radiofrequency identification tags (RFID) [
17]. The labelling on dentures can assist and expedite the identification process, however the forensic odontologist should check how the denture fits in the decedent’s mouth and support the identification with anatomical features, or additional identifiers.
(e) Dental and maxillofacial anatomy: Anatomical variation of the dental and maxillofacial structures is highly useful in antemortem vs. postmortem comparisons, especially in those cases where no dental treatment can be compared. Teeth present and absent; crown, root and pulp morphology; maxillary sinus morphology and its relationship with the maxillary dental roots; location and morphology of the mental foramen and inferior alveolar canal; or the trabecular patterns are some informative features that can be compared in the antemortem and postmortem images.
The value of anatomical variation for identification relies on their frequency of appearance within the population, but there is a lack of knowledge on frequencies of certain anatomical variants. Thus, establishing the hierarchy of the consistent anatomical traits according to their frequency relies on the forensic odontologist’s experience. Nevertheless, combining different anatomical features increases the robustness of the comparison.
The above-described features are the most common and reliable in the comparison of postmortem and antemortem data sets. Additional features can be used in certain identification cases such as the palatal rugae and lip prints. Some research has been made in dental imaging superimposition due the recent increase of smiling photographs in social media, representing a source of antemortem data [
8].
(f) Palatal rugae: Palatal rugae have been shown to be highly individualistic and consistent in shape throughout life [
18]. Palatal rugae are well represented in intraoral scans, which have increased in frequency in recent years. Studies have shown that the use of intraoral scans of the anterior aspect of the palate, including the rugae can be a reliable mean of identification [
19].
(g) Cheiloscopy: Cheiloscopy studies the patterns formed by the wrinkles and grooves of the labial mucosa forming a characteristic pattern described as “lip prints” [
19,
20]. Lip prints can be useful to identify the deceased in seldom cases, and its use was better justified when the use of DNA was not a possibility. Nowadays, the primary efforts should be put in trying to extract DNA from the evidence as finding a lip print that could be useful in identifying the deceased (or even in any other criminal cases).
(h) Dental imaging superimposition: Teeth constitute the only dental structures that are exposed during life. The craniofacial superimposition process involves superimposing an image of the recovered skull over an antemortem image of the suspected individual [
21] by correlating the landmarks in the skeletal tissue with those in the soft tissues. This correlation between the skeletal and soft tissue landmarks is an estimation, except for the dental tissues, in which a direct superimposition is made. Therefore, the accuracy of the superimposition increases when dental structures are visible. A number of studies have focused on the reliability of craniofacial and dental superimpositions, where the dentition of the unidentified skull is superimposed to the visible teeth of an antemortem photograph [
22,
23,
24]. Serious disadvantages of the techniques used to conduct dental superimpositions include the number of visible teeth and the quality of the antemortem image(s) provided. Often, the quality of the image is poor, and the visible teeth are limited to the incisors, canines and sometimes premolars, which have only their anterior surfaces visible (and occasionally part of their lateral surfaces).
Whilst advances in dental and craniofacial superimposition have been achieved with the use of 3D imaging techniques, further research is needed mainly due to the small sample size and the lack of validation studies for these techniques [
6,
11,
22]. Moreover, when comparing a 3D model of the dentition with a 2D photograph, it is often more efficient to simply compare the dental traits observed in both images rather than conduct the superimposition, which may not be needed to show the similarities and differences between the two antemortem and postmortem dentition images. Nowadays, a positive identification should not solely be made with a dental superimposition, and other biological evidence should be investigated.
6. Expert’s Final Conclusion of the Analysis
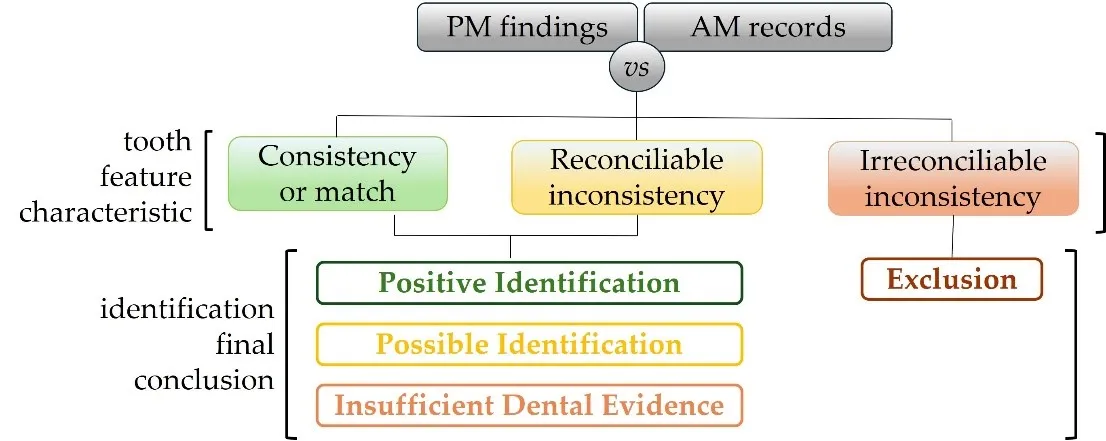
After all teeth and anatomical structures available in both data sets are compared, the forensic odontologist evaluates the compilation of matches, reconcilable and irreconcilable inconsistencies. This leads to an opinion that, according to the ABFO, can represent: (i) a positive identification, if the antemortem and postmortem data sets are consistent in sufficient detail to establish that they are from the same individual, and no irreconcilable discrepancies are found; (ii) a possible identification, if the antemortem and postmortem data sets have consistent features, but they are not enough to positively establish dental identification; (iii) insufficient dental evidence, if the available information is insufficient to form a conclusion; (iv) an exclusion, if the antemortem and postmortem data sets are clearly inconsistent [
5] ().
. Stages of the postmortem (PM) and antemortem (AM) odontological comparison process.
In the past, some studies have suggested that a minimum number of points of concordance should be stablished in the comparison of the postmortem and antemortem records. Stimson, 1975 considered eight (8) points of concordance as the minimum to establish a positive identification [
25]. Sognnaes in 1976 and Keiser-Nielsen in 1980 both considered twelve (12) points of concordance as the minimum to establish a positive identification [
26,
27]. However, none of these studies presented a dental based rationale of the reason behind the threshold considered for the minimum number of points of concordance, other than a simile of the fingerprint comparison. Acharya and Taylor in 2003 proved that no basis exists for defining a minimum number of concordant points to achieve a positive identification in forensic odontology [
14,
15]. So, a positive identification by dental evidence can be established from just a few teeth, a single tooth or even in edentulous individuals using a combination of concordant features [
1,
14,
15,
28].
While the first step of comparing all teeth and maxillofacial areas identifying consistencies and discrepancies is an objective task, decisions as to whether the discrepancy can be reconciled is a subjective task that depend on the expertise of the forensic odontologist. Likewise, the final conclusion of the identification where the forensic odontologist forms an opinion based on their knowledge and proficiency is also subjective [
6].
Nonetheless, literary references and the use of Odontosearch can increase the objectivity of the expert’s opinion. Odontosearch is a computer program that provides statistical values and, therefore, an objective means of quantifying the relative frequency that a dental pattern occurs in the general population. Currently, the OdontoSearch database includes dental records of 107,002 adults where present and missing teeth as well as restorations are recorded [
29].
7. Computer Comparison Programs
Computer comparison programs can assist in the identification process, especially in cases where no candidates for the identity are suspected, as well as in mass fatality incidents, where large number of data are managed.
The postmortem and antemortem information are entered into their respective and separate databases. These are interconnected with an interface that can generate thousands of comparisons and provide a rank-ordered list of possible candidates that can then be confirmed or rejected by the expert’s evaluation [
15].
Nowadays there are three main software packages with dental identification modules: WinID, DVI System International and UVIS.
WinID is an identification computer software developed by Dr. James McGivney in the late 1990’s, consisting of a stand-alone dental identification computer program in which only dental information is considered. Dental data is entered using primary codes, with the option of entering secondary codes, as well as expert’s comments. The ranking comparisons can be given according to numerous sorting options: Most Dental Hits; Least Dental Mismatches; Most Restoration Hits; and Fuzzy Dental Logic. The system allows users to upload radiographic data and includes a bridge with the DEXIS digital radiography application that permits the linking of demographic information to the radiography application. In 2014, the source code was assigned to the American Board of Forensic Odontology, and WinID is now available on its website at http://www.abfo.org/winid/ [
14,
30]. Recently, WinID was adapted to a web version within the PhotoDoc software. WinID has been widely used in the United States for numerous multiple fatality incidents such as Hurricane Katrina and the World Trade Center, among others. It must be noted there are no specific dental codes for certain descriptors and those must be coded as a combination of codes (such as dental implants). Despite the recent adaptation to the web, the dental coding system has not been revised.
The DVI System International is a paid commercial software package, product of Plass Data Software (https://www.kmd.net/solutions-and-services/data-and-ai/kmd-plassdata-dvi/). It contains a dental module within the multiple levels of the disaster management system. DVI System International is the official software for INTERPOL DVI operations, ever since the agreement between the two entities in 2005. The visual and graphic design of this software is based on the INTERPOL DVI forms, but it has incorporated additional color codes and symbols, and allows users to upload photographs and radiological images. The complete integration of both paper and electronic data allows the system to work under any circumstances. In 2014 the INTERPOL Forensic Odontology Sub-Working Group simplified the coding system, given the high number of descriptors the system presented. The comparisons are created through and interface between the antemortem and the postmortem data entry, where it rank-orders possible matches. This software is continually reviewed and updated.
UDIM (UVIS Dental Identification Module) was developed by Dr. Kenneth Aschheim (in conjunction with the forensic odontologists of OCME and ICRA Sapphire Inc.) as the dental module of UVIS (Unified Victim Identification System). The system was created after the 9/11 World Trade Center attack, by the Office of Chief Medical Examiner of the City of New York (NYC-OCME) as a web browser-based application to handle mass disaster situations. UDIM presents a simple coding system that can be complemented by adding optional descriptors. It has a self-correcting interface that detects and highlights any coding that cannot be possible. As of today, UDIM is the only dental identification software that offers a simple option to reassociate fragments, which is extremely useful in incidents involving fragmentation [
14,
30]. The system allows image importation and creates a rank-ordered list with all possible matches. UVIS and UDIM, although initially developed for DVI management purposes, have adapted their system for use on a regular basis, having now a special option setting for DVI. The everyday use of the system represents an enormous advantage if the DVI mode is activated, since the Forensic Odontology Team at NYC-OCME use the software regularly, which eases the operation of the dental team in case of a mass disaster.
All these dental identification software packages generate a rank-ordered list with all possible matches between the antemortem and postmortem data entered. Forensic odontologists must review and evaluate these possible matches in order to form an opinion on the identification of the remains. These computer-based systems are a useful tool, but the eyes and judgement of an expert is required to achieve a positive identification, or an exclusion.
8. Future (or Actually Present) Directions
New technologies are evolving and are rapidly implemented in the clinical setting, dictating the evolution of antemortem records provided in casework.
Three-dimensional imaging techniques and modalities are emerging disruptive technologies, which, driven by technological advances, continue to get cheaper, smaller, more reliable, and easier to use [
31].
Digital 3D models of the dental arches are replacing the traditional dental impressions. The 3D tissue models are the result of optical impressions and represent the digital alternative to traditional plaster models [
32].
As digital impressions begin to move into the mainstream of modern dental practice, antemortem 3D datasets are increasingly presented as part of the AM dental profile [
8]. Thus, it is important for forensic odontologists to be familiar with this format of 3D antemortem data, and what information it offers for the identification process.
Nowadays, computed tomography in all its modalities is a conventional imaging tool for diagnosis and treatment. The applications of this technology include all aspects of odontology such as orthodontics, endodontics, oral surgery and periodontics [
33].
The images obtained by conventional radiography and computed tomography offer information about the external surfaces and the internal structure of the tissues, while the images obtain by surface scanners offer only information of the tissues external surface. Thus, radiography and computed tomography contain more information to be compared in the postmortem and antemortem datasets than the surface scans (though all can be critical pieces of information in identification cases).
The use of artificial intelligence (AI) in forensic odontological identifications has been explored in the recent years, bringing new technological challenges to this field. The AI-based technologies applied to forensic odontology include deep neural networks, artificial neural networks, machine learning, and computational technology [
34].
Machine learning aims to enable computers to learn from data sets and solve problems on their own without the need for human intervention. Neural networks are algorithms structured to produce similar functions to the human brain. A subset of machine learning known as “deep learning” analyzes input data by employing a deep neural network with several computational layers. Building a neural network with automatic pattern recognition is the aim of deep learning, hoping to enhance feature identification [
35]. Deep neural networks have been applied to dental identification, attempting to overcome human subjectivity and expedite the identification process [
36,
37]. Initial limitations of automatic comparisons included the inability of finding significant differences when only few teeth were present, as well as detecting significant reconcilable changes in the dentition. However, recent studies have shown successful attempts at overcoming these limitations, allowing the models to rely not only on teeth characteristics but also other skeletal markers [
37].
Extensive research is needed to properly implement AI in forensic casework, which would expedite the process of identification and report generation, but as of now, the expert’s assessment will be required to render a final opinion about the identity of the decedent.
9. Conclusions
Human identification is undoubtedly the core element of forensic odontology, involving the comparison of postmortem findings and antemortem records. Considering all types of dental records, clinical images are the most informative and objective form of data to conduct the comparisons, including radiographs, computed tomography, 3D surface scans and photographs. Forensic odontologists must be familiar with the formats of these different modalities and the data they can provide to assist in the identification process. Computer software packages can assist in the postmortem vs. antemortem comparison, connecting the postmortem and antemortem information and creating a ranking of possible matches. Moreover, deep machine learning models are being explored automate the comparison process. However, all comparison procedures still require the expert’s final assessment. Forensic odontology is constantly evolving and adapting to improve identification techniques and methods, while maintaining the standards required for forensic casework.
Acknowledgments
We acknowledge with profound gratitude the privilege of working with the forensic cases that have provide us the experience included in this article. Every case serves as reminders of the responsibility entrusted to us, emphasizing the importance of meticulous attention to detail and rigorous analysis. All our appreciation to the deceased and their loved ones of past (and future) cases.
Author Contributions
Conceptualization: J.A.-G.; Writing—Original Draft Preparation: J.A.-G., J.R.; Writing—Review & Editing: J.R., S.D.H.; Graphic material preparation: J.A.-G., J.R., S.D.H.
Ethics Statement
This article does not contain any studies with human participants or animals performed by the authors.
Informed Consent Statement
Not applicable.
Funding
This research received no funding.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
1.
Hinchliffe J. Forensic odontology, Part 1. Dental identification.
Br. Dent. J. 2011,
210, 219–224. doi:10.1038/sj.bdj.2011.146.
[Google Scholar]
-
2.
Miller R, Bush M. 21st Century Forensic Odontology.
NY State Dent. J. 2020,
86, 19–23.
[Google Scholar]
-
3.
Sweet D. Forensic dental identification.
Forensic Sci. Int. 2010,
201, 3–4.
[Google Scholar]
-
4.
Adserias-Garriga J. Age-at-Death Estimation by Dental Means as a Part of the Skeletal Analysis.
Forensic Sci. 2023,
3, 357–367. doi:10.3390/forensicsci3020027.
[Google Scholar]
-
5.
American Board of Forensic Odontology (ABFO). Body Identification Information & Guidelines. 2017. Available online: https://abfo.org/wp-content/uploads/2012/08/ABFO-Body-ID-Information-Guidelines-Feb-2017.pdf (accessed on 14 July 2024).
-
6.
Sims CA, Berketa J, Higgins D. Is human identification by dental comparison a scientifically valid process?
Sci. Justice 2020,
60, 403–405. doi:10.1016/j.scijus.2020.05.002.
[Google Scholar]
-
7.
Berman GM, Bush MA, Bush PJ, Freeman AJ, Loomis PW, Miller RG. Chapter 4. Dental Identification. In Manual of Forensic Odontology, 5th ed.; Senn DR, Weems RA, Eds.; CRC Press Taylor and Francis Group: Boca Raton, FL, USA, 2013.
-
8.
Forrest A. Forensic odontology in DVI: Current practice and recent advances.
Forensic Sci. Res. 2019,
4, 316–330. doi:10.1080/20961790.2019.1678710.
[Google Scholar]
-
9.
Brown LF. Inadequate record keeping by dental practitioners.
Aust. Dent. J. 2015,
60, 497–502.
[Google Scholar]
-
10.
Manica S. A New Website to Aid the Interpretation of Antemortem Dental Records: www.international dentalcharts.org.
J. Forensic Odontostomatol. 2014,
32, 1–7.
[Google Scholar]
-
11.
Forrest AS, Wu HY. Endodontic imaging as an aid to forensic personal identification.
Aust. Endod. J. 2010,
36, 87–94.
[Google Scholar]
-
12.
Silver WE, Souviron RR. Chapter 8, Antemortem Records. In Dental Autopsy; CRC Press Taylor and Francis Group: Boca Raton, FL, USA, 2009; pp. 81–87.
-
13.
Lorton L, Langley WH. Design and use of a computer-assisted postmortem identification system.
J. Forensic Sci. 1986,
31, 972–981.
[Google Scholar]
-
14.
Acharya AB, Taylor JA. Are a minimum number of concordant matches needed to establish identity in forensic odontology?
J. Forensic Odontostomatol. 2003,
21, 6–13.
[Google Scholar]
-
15.
American Dental Association (ADA) Technical Report No. 1088. Available online: https://www.nist.gov/system/files/documents/2021/12/06/Revised%20ADA%20Technical%20Report%20No%201088%20Final%20July%202020.pdf (accessed on 14 July 2024).
-
16.
Howell K, Farley N. Available online: www.whatimplantisthat.com (accessed on 14 July 2024).
-
17.
Thomas T, Muruppel AM, Dinesh N, Gladstone S, George N. Dentures in Forensic Identification-A Review of Methods & Benefits.
J. Adv. Med. Dent. Sci. 2014,
2, 85–94.
[Google Scholar]
-
18.
Stuart LS, Leonard G. Forensic Application of Palatal Rugae in Dental Identification; Forensic Examiner Spring, Thompson, CT, USA, 2005; pp. 44–47.
-
19.
Mikolicz A, Simon B, Gáspár O, Shahbazi A, Vag J. Reproducibility of the digital palate in forensic investigations: A two-year retrospective cohort study on twins.
J. Dent. 2023,
135, 104562. doi:10.1016/j.jdent.2023.104562.
[Google Scholar]
-
20.
Santhosh Kumar S, Chacko R, Kaur A, Ibrahim G, Ye D. A Systematic Review of the Use of Intraoral Scanning for Human Identification Based on Palatal Morphology.
Diagnostics 2024,
14, 531. doi:10.3390/diagnostics14050531.
[Google Scholar]
-
21.
Ubelaker DH, Wu Y, Cordero QR. Craniofacial photographic superimposition: New developments.
Forensic Sci. Int. Synerg. 2019,
1, 271–274. doi:10.1016/j.fsisyn.2019.10.002.
[Google Scholar]
-
22.
Miranda GE, Freitas SG, Maia LVA, Melani RFH. An unusual method of forensic human identification: Use of selfie photographs.
Forensic Sci. Int. 2016,
263, e14–e17. doi:10.1016/j.forsciint.2016.04.028.
[Google Scholar]
-
23.
Santoro V, Mele F, Introna F, De Donno A. Personal identification through digital photo superimposition of dental profile: A pilot study.
J. Forensic Odontostomatol. 2019,
37, 21–26.
[Google Scholar]
-
24.
Damas S, Cordón O, Ibáñez O. Handbook on Craniofacial Superimposition the MEPROCS Project; Springer: Cham, Switzerland, 2020; ISBN 978-3-319-11136-0; ISBN 978-3-319-11137-7.
-
25.
Stimson PG. Radiology in forensic odontology.
Dent. Radiogr. Photogr. 1975,
48, 51–55.
[Google Scholar]
-
26.
Sognnaes RF. Dental science as evidence in court.
Int. J. Forensic Dent. 1976,
3, 14–16.
[Google Scholar]
-
27.
Keiser-Nielsen S. Person Identification by Means of the Teeth: A Practical Guide; John Wright and Sons Ltd.: Bristol, UK, 1980.
-
28.
Lundberg E, Mihajlovic NS, Sjöström M, Ahlqvist J. The use of panoramic images for identification of edentulous persons’.
J. Forensic Odonto-Stomatol. 2019,
37, 18–24.
[Google Scholar]
-
29.
Aschheim KW, Adams BJ. 2018. Available online: https://www.odontosearch.com/en/3.2/about.html (accessed on 14 July 2024).
-
30.
Berman GM, Nawrocki L, Hermsen K, Miller RG, Weems R. Chapter 6. Disaster Victim Identification. In Manual of Forensic Odontology, 5th ed.; Senn DR, Weems RA, Eds.; CRC Press Taylor and Francis Group: Boca Raton, FL, USA, 2013.
-
31.
Farahani N, Braun A, Jutt D, Huffman T, Reder N, Liu Z, et al. Three-dimensional Imaging and Scanning: Current and Future Applications for Pathology.
J. Pathol. Inform. 2017,
8, 36. doi:10.4103/jpi.jpi_32_17.
[Google Scholar]
-
32.
Angelone F, Ponsiglione AM, Ricciardi C, Cesarelli G, Sansone M, Amato F. Diagnostic Applications of Intraoral Scanners: A Systematic Review.
J. Imaging 2023,
9, 134. doi:10.3390/jimaging9070134.
[Google Scholar]
-
33.
Jain S, Choudhary K, Nagi R, Shukla S, Kaur N, Grover D. New evolution of cone-beam computed tomography in dentistry: Combining digital technologies.
Imaging Sci. Dent. 2019,
49, 179–190. doi:10.5624/isd.2019.49.3.179.
[Google Scholar]
-
34.
Mohammad N, Ahmad R, Kurniawan A, Mohd Yusof MYP. Applications of contemporary artificial intelligence technology in forensic odontology as primary forensic identifier: A scoping review.
Front. Artif. Intell. 2022,
5, 1049584. doi:10.3389/frai.2022.1049584.
[Google Scholar]
-
35.
Backiyalakshmi A, Divya VC. Artificial intelligence in forensic odontology: A review.
IP Int. J. Maxillofac. Imaging 2024,
10, 6–10.
[Google Scholar]
-
36.
Choi H-R, Siadari TS, Kim J-E, Huh K-H, Yi W-J, Lee S-S, et al. Automatic detection of teeth and dental treatment patterns on dental panoramic radiographs using deep neural networks.
For. Sci. Res. 2022,
7, 456–466. doi:10.1080/20961790.2022.203 4714.
[Google Scholar]
-
37.
Enomoto A, Lee AD, Sukedai M, Shimoide T, Katada R, Sugimoto K, et al. Automatic identification of individuals using deep learning method on panoramic radiographs.
J. Dent. Sci. 2024,
18, 696–701.
[Google Scholar]