Impact of a Government Ban on Paraphenylenediamine (PPD) Availability: An Interrupted Time Series Analysis of Suicidal Poisoning Cases in Bahawalpur, Pakistan (2016–2024)

Impact of a Government Ban on Paraphenylenediamine (PPD) Availability: An Interrupted Time Series Analysis of Suicidal Poisoning Cases in Bahawalpur, Pakistan (2016–2024)
Amna Arooj 1,* Hifz Ur Rehman 2 Mudassir Daud 3 Samiaan Qurban Khan 4 Ghulam Abbas Haral 5 Hafiz Muhammad Abbas Malik 6,* Khalid Sajjad Feras 7 Muhammad Qasim Adnan 8
Received: 14 February 2026 Revised: 05 March 2026 Accepted: 24 April 2026 Published: 12 May 2026

© 2026 The authors. This is an open access article under the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
1. Introduction
Suicide is a significant global public health challenge, with self poisoning being one of the most common methods, particularly in developing countries where toxic substances are readily available [1]. In Pakistan, substance abuse has been identified as a major contributing factor to suicidal behavior [2], creating a pressing need for effective, evidence based prevention strategies. In the southern regions of the Punjab province, a unique and severe public health crisis emerged from the misuse of Paraphenylenediamine (PPD), a chemical agent found in permanent hair dyes [3]. Locally known as “Kala Pathar” or “Black Stone”, PPD became a preferred agent for intentional self harm due to its low cost, widespread availability, and extreme toxicity [4]. Historically, studies from this region identified PPD as one of the most commonly misused substances leading to suicidal behavior. Ingestion of PPD leads to a rapid onset of life threatening symptoms, including severe airway obstruction, rhabdomyolysis, and acute kidney injury, resulting in high mortality rates [5]. The escalating number of PPD-related hospital admissions and fatalities placed an immense burden on the healthcare system, particularly in tertiary care hospitals in Bahawalpur [6].
In response to this crisis, the Government of Punjab implemented a key public health policy prohibiting the commercial scale distribution and sale of raw PPD to the public [7]. This regulatory intervention was specifically aimed at reducing the accessibility of this lethal substance to curb its use in suicides. While such policies are intended to reduce substance related harm, their direct impact is not always guaranteed and requires rigorous evaluation [8].
Despite the severity of the PPD crisis and the implementation of this significant policy, a clear research gap exists. There has been a lack of quantitative, region specific studies examining the effectiveness of this prohibition on suicidal trends in high prevalence areas. This study, therefore, aims to address this gap by evaluating the impact of the commercial prohibition of PPD on the incidence of PPD related poisoning cases in Bahawalpur. Using a robust interrupted time series analysis, we seek to provide clear evidence on the effectiveness of this targeted public health intervention [9].
2. Literature Review
2.1. The Toxicology of Paraphenylenediamine (PPD) Poisoning
Paraphenylenediamine (PPD) is an organic compound widely used as a primary component in permanent hair dyes. While relatively safe when used as directed in regulated, low concentration formulas, its raw, concentrated form is a potent and fast acting poison. Ingestion of PPD leads to a well documented and distinct clinical toxidromes [10]. The initial phase is characterized by severe cervicofacial angioedema, causing swelling of the neck, face, and tongue, which can rapidly progress to life threatening airway obstruction and respiratory failure. This is followed by a second phase marked by severe rhabdomyolysis (skeletal muscle breakdown) and subsequent myoglobinuria, which manifests as dark brown or “cola colored” urine. The myoglobin overload is directly nephrotoxic, leading to acute kidney injury (AKI) and renal failure, a primary cause of mortality in patients who survive the initial respiratory distress [11].
2.2. Suicide and Substance Regulation in Pakistan
Suicide is a complex public health issue in Pakistan, influenced by various socioeconomic and psychological factors. Notably, research has consistently identified substance abuse as a significant contributor to suicidal behavior across the nation, particularly among vulnerable populations [8,12]. The choice of agent for self poisoning is often dictated by local availability and cost. In the regions of Southern Punjab, including Bahawalpur, studies have identified PPD (“Kala Pathar”) as a commonly misused substance directly linked to suicidal behavior due to its easy accessibility.
In response to public health threats posed by toxic substances, governments worldwide implement regulatory policies, such as sales restrictions or outright prohibitions. The effectiveness of such policies, however, is a subject of ongoing debate in public health literature [13]. Some studies have shown that prohibitions can successfully lead to a decline in substance related fatalities, while others caution that such measures can have unintended consequences, such as driving the market underground. The Pakistani government’s decision to prohibit the commercial scale distribution of PPD was a direct attempt to curb its misuse and reduce its associated health risks [14].
2.3. The Identified Research Gap
While the link between PPD and suicide in Pakistan is established, a clear gap in the literature exists regarding the measurable impact of the government’s prohibition policy. There has been a lack of region specific studies designed to quantitatively assess whether this major regulatory intervention actually led to a reduction in suicidal PPD poisoning. This highlights the need for a focused investigation to understand the effectiveness of the PPD prohibition in the specific context of Bahawalpur, a region historically affected by this crisis [15].
3. Materials and Methods
3.1. Study Design
This was a retrospective, descriptive, hospital based study designed to analyze the trends, clinical outcomes, and treatment patterns of para phenylenediamine (PPD) poisoning cases over an eight year period. The study employed a cross sectional analytical approach to examine temporal variations in case incidence and associated clinical parameters.
3.2. Ethical Approval
This study was approved by the Forensic Human Ethical Committee, Islamia University of Bahawalpur. Informed consent was obtained from the Medical Superintendent prior to the commencement of the study.
3.3. Study Setting
The study was conducted at Bahawal Victoria Hospital, a tertiary care referral center located in Bahawalpur, serving both urban and rural populations. As a major referral hospital with specialized emergency and critical care facilities, the institution receives the majority of acute poisoning cases from the surrounding districts, making it representative of the regional burden of PPD poisoning. The hospital maintains comprehensive medical records and operates a dedicated toxicology unit with 24-h emergency services.
3.4. Study Period
Data were collected for cases admitted between 1 January 2016 and 30 November 2024, encompassing a complete eight-year study period with partial data for 2024. This timeframe was selected to capture sufficient case volume for meaningful trend analysis while ensuring data completeness and accessibility of medical records.
3.5. Study Population and Sampling
Inclusion Criteria: The study included all patients with a confirmed diagnosis of PPD poisoning based on:
-
-
Clear history of PPD ingestion from patient, family members, or witnesses (Table 1)
-
-
Clinical presentation consistent with PPD toxicity (laryngeal edema, dark colored urine, cardiovascular instability)
-
-
Laboratory confirmation, where available (methemoglobinemia, elevated serum creatinine)
-
-
Presence of characteristic physical evidence (PPD residue, packaging)
Exclusion Criteria: Cases were excluded from the analysis if they met any of the following criteria(Table 1):
-
-
Unknown or unconfirmed substance ingestion with uncertain etiology
-
-
Incomplete medical records lacking essential demographic or outcome data
-
-
Mixed poisoning cases where PPD was not the primary toxic agent
-
-
Cases transferred from other facilities without complete clinical information
-
-
Patients who left against medical advice before treatment completion
Data Collection and Variables: Data were extracted from patient records in the accident and emergency department using a pre designed performa. The following variables were collected for each case: demographic profile (age and gender) and manner of poisoning (suicidal, accidental). For the time series analysis, the primary outcome variable was the total number of PPD poisoning cases recorded per year, based on the data presented in the results table. To enhance epidemiological interpretation, annual incidence rates of PPD poisoning were calculated per 100,000 population. Population estimates for the Bahawalpur district were obtained from the Pakistan Bureau of Statistics and interpolated for intercensal years where necessary. Incidence rates were computed by dividing annual case counts by the estimated population for each year and multiplying by 100,000.
The Intervention: The intervention was defined as the implementation of the Government of Punjab’s policy prohibiting the commercial scale distribution of raw PPD (“Kala Pathar”). The exact date of the formal implementation of the Punjab government’s prohibition on the commercial scale distribution of raw PPD could not be verified through a publicly accessible official notification or gazette record. The designation of the intervention period was therefore based on triangulation of multiple sources, including regional clinical observations, hospital admission trends, and secondary literature reporting regulatory action around late 2017. These sources consistently indicate that enforcement and market restrictions began toward the end of 2017, with observable impact emerging in the subsequent calendar year. Based on the annual case data, which shows a peak in 2017 followed by a sharp, sustained decline, the intervention point for the ITS analysis was set at the transition between 2017 and 2018. This operational definition reflects the first full post policy year, given that implementation and enforcement were reported to have occurred during late 2017.
A key methodological consideration in this analysis is the use of annual aggregated data rather than higher frequency (monthly or quarterly) observations. While interrupted time series designs ideally require a larger number of pre and post intervention time points to improve statistical power and control for underlying trends, only two complete pre intervention years (2016–2017) were available in this dataset. Monthly or quarterly data were not accessible due to limitations in hospital record digitization and retrospective data structure.
Despite this limitation, annual data were considered appropriate for the present analysis because the intervention represented a large scale regulatory policy expected to produce substantial and sustained population level effects rather than short term fluctuations. Moreover, the magnitude of the observed post intervention decline and the consistency of the downward trend across multiple subsequent years support the robustness of the findings. However, the limited number of pre intervention observations restricts the precision of baseline trend estimation and should be considered when interpreting causal inferences.
All data were entered into a standardized electronic database with built in validation checks. Double data entry was performed for 10% of randomly selected records to ensure accuracy. Missing data were categorized and analyzed for patterns. Regular data quality audits were conducted throughout the collection period.
3.6. Statistical Analysis
Data analysis was performed using SPSS version 28.0 (IBM Corp., Armonk, NY, USA) and Microsoft Excel 2019. Descriptive statistics were calculated for all variables, with categorical variables presented as frequencies and percentages, and continuous variables as means with standard deviations or medians with interquartile ranges, depending on distribution normality assessed by Shapiro Wilk test. Trend analysis was conducted using linear regression to assess temporal changes in case incidence over the study period. Chi square tests were employed to examine associations between categorical variables, while independent t tests or Mann Whitney U tests were used for continuous variables based on data distribution. Mortality rates were calculated annually, and case fatality rates were analyzed using logistic regression to identify predictive factors.
Statistical significance was set at p < 0.05 for all analyses. Trend analysis included calculation of annual percentage change and 95% confidence intervals to quantify the magnitude and direction of temporal changes in PPD poisoning incidence.
Interrupted Time Series (ITS) Segmented Regression Analysis. To formally evaluate the impact of the prohibition policy, a segmented regression model was applied to annual PPD poisoning counts across the study period (2016–2023). Annual data points (n = 8 complete years) were used as the unit of analysis, with the intervention point defined as January 2018 (i.e., the year immediately following the peak year of 2017). The standard ITS segmented regression model was specified as follows:
|
```latex\mathrm{Y_t=\beta_0+\beta_1\cdot Time_t+\beta_2\cdot Intervention_t+\beta_3\cdot Time\_After_t+\varepsilon_t}``` |
|
where Yt is the observed annual count of PPD poisoning cases; Timet is a continuous variable representing the year number (coded 1–8 for 2016–2023); Interventiont is a binary indicator variable (0 = pre intervention years 2016–2017; 1 = post intervention years 2018–2023); Time_Aftert is a continuous variable representing time elapsed since the intervention (0 for pre intervention years; 1, 2, 3… for each successive post intervention year); β0 represents the baseline level of the outcome at the start of the observation period; β1 represents the pre intervention trend (slope); β2 captures the immediate level change (step change) at the point of intervention; β3 captures the change in slope following the intervention (trend change); and εt is the error term. This model enables simultaneous estimation of any abrupt level change and any gradual slope change attributable to the policy, which is the defining analytical advantage of the ITS design over simple pre–post comparisons.
Given the limited number of annual data points (n = 8), the model was estimated using ordinary least squares (OLS) regression, and the Durbin–Watson (DW) statistic was computed to evaluate the presence of first order autocorrelation in the residuals. The DW value was 1.87 (acceptable range: 1.5–2.5), indicating no significant autocorrelation and supporting the appropriateness of OLS estimation for this dataset. For analytical purposes, the intervention point was operationalized as January 2018, representing the first full year following the reported implementation and enforcement phase of the policy. This approach is consistent with the interrupted time series methodology when exact intervention dates are uncertain, but policy effects are expected to manifest at the population level after a short lag period. Modeling the intervention as an immediate level change at the start of 2018 allows for a conservative and standardized estimation of policy impact, while acknowledging that real world implementation may have occurred gradually during late 2017.
All ITS model coefficients, their 95% confidence intervals (CIs), and corresponding p values are reported in Table 3. The model demonstrated excellent overall fit, with an adjusted R2 of 0.94 (p < 0.001), indicating that approximately 94% of the variance in annual case counts was explained by the model variables.
Table 1. Case Definitions and Study Criteria.
|
Criteria Category |
Definition |
Specifications |
|---|---|---|
|
Confirmed PPD Poisoning |
Primary inclusion criterion |
Clear history of PPD ingestion + consistent clinical presentation + supporting evidence |
|
History Confirmation |
Documentation requirement |
Patient/witness account or physical evidence of PPD exposure |
|
Clinical Consistency |
Symptom correlation |
Laryngeal edema, dark urine, cardiovascular instability, renal dysfunction |
|
Laboratory Support |
When available |
Methemoglobinemia, elevated creatinine, metabolic acidosis |
|
Complete Records |
Data completeness |
Essential demographic, clinical, and outcome data available |
|
Exclusion Unknown Substance |
Uncertainty criterion |
Unconfirmed ingestion or multiple possible toxic agents |
|
Exclusion Incomplete Data |
Data quality criterion |
Missing critical demographic, treatment, or outcome information |
|
Exclusion Mixed Poisoning |
Specificity criterion |
Cases where PPD was not the primary or sole toxic agent |
|
Exclusion Transfer Cases |
Data integrity criterion |
Patients transferred without complete clinical documentation |
|
Time Frame |
Study period |
1 January 2016–30 November 2024 |
4. Results
4.1. Overall Incidence and Trends
During the eight year study period from January 2016 to November 2024, a total of 4455 confirmed cases of paraphenylenediamine (PPD) poisoning were admitted to our tertiary care facility. The temporal distribution of cases revealed significant year to year variations with distinct patterns of incidence over the study period. The highest number of cases was recorded in 2017 with 1243 admissions, representing a 49.4% increase from the 832 cases documented in 2016. This peak was followed by a slight decline to 1005 cases in 2018, still maintaining elevated numbers compared to the baseline year. A dramatic reduction occurred in 2019 with only 407 cases, representing a 59.5% decrease from the previous year. The years 2020 and 2021 showed the lowest case burden with 248 and 260 cases respectively, likely influenced by multiple factors including healthcare seeking behavior changes and potential underreporting during the COVID-19 pandemic period.
A gradual stabilization was observed from 2022 onwards, with 266 cases recorded, followed by 155 cases in 2023. The partial data for 2024 showed 39 cases in the first quarter, which, when projected annually, suggests a continued declining trend. The overall trend analysis revealed a statistically significant decrease in annual case incidence over the study period (p < 0.001), with an average annual reduction rate of 12.3%.
4.2. Incidence Rates of PPD Poisoning
When adjusted for population size, the annual incidence of PPD poisoning demonstrated a marked decline following the intervention period. The incidence peaked in 2017, corresponding to the highest recorded case count, and subsequently decreased substantially from 2018 onwards. This decline remained consistent even after accounting for population growth, indicating that the observed reduction in cases reflects a true decrease in disease burden rather than demographic changes. The sustained downward trend in incidence rates further supports the effectiveness of the regulatory intervention at the population level.
Demographic Profile of Patients Analysis of a subset of 2261 cases from the peak period revealed a clear demographic profile. There was a significant male predominance, with males accounting for 1625 (72%) of cases, while females accounted for 636 (28%). The most commonly affected age group was young adults aged 21–40 years, which comprised 1080 cases (48%). The least affected group was individuals over 60 years of age (n = 95, 4%). In the vast majority of cases, the manner of poisoning was determined to be suicidal in intention.
4.3. Mortality Analysis
The mortality analysis revealed a total of 467 deaths across the study period, yielding an overall case fatality rate of 10.5%. Annual mortality patterns showed considerable variation, with case fatality rates ranging from 3.8% to 20.2% across different years.
The year 2017, despite having the highest absolute number of cases, recorded 156 deaths with a case fatality rate of 12.5%. In contrast, 2016 showed 91 deaths among 832 cases, resulting in a case fatality rate of 10.9%. The lowest mortality pattern was observed in 2018, where, despite having 1005 cases, only 38 deaths occurred, yielding the lowest case fatality rate of 3.8% throughout the study period. This unusually low case fatality rate in 2018 may reflect a combination of factors, including earlier presentation of patients, improved emergency airway management, and possible shifts in case identification or reporting practices following heightened clinical awareness of PPD toxicity after the 2017 peak (Table 2). Additionally, the high case volume in 2018 may have included a greater proportion of less severe exposures, contributing to lower overall mortality.
The year 2019 demonstrated 53 deaths among 407 cases, resulting in a case fatality rate of 13.0%. The most alarming mortality statistics were recorded in 2020, where 50 deaths occurred among 248 cases, yielding the highest case fatality rate of 20.2% observed during the entire study period. This elevated mortality coincided with the COVID-19 pandemic and may reflect delayed presentation, overwhelmed healthcare systems, or modified treatment protocols due to resource constraints. The markedly elevated case fatality rate observed in 2020 likely reflects increased case severity and systemic healthcare constraints during the COVID-19 pandemic. Delayed hospital presentation, reduced access to timely critical care, and resource limitations in intensive care settings may have contributed to poorer outcomes. Furthermore, the lower number of total cases in 2020 suggests that only more severe poisoning cases may have reached tertiary care facilities, introducing a selection bias toward higher mortality. Subsequent years showed more stable mortality patterns, with 2021 recording 28 deaths among 260 cases (10.8% CFR), 2022 showing 31 deaths among 266 cases (11.7% CFR), and 2023 demonstrating 15 deaths among 155 cases (9.7% CFR) (Table 2). The first quarter of 2024 recorded 5 deaths among 39 cases, yielding a case fatality rate of 12.8% (Figure 1).
Statistical analysis revealed no significant linear trend in case fatality rates over the study period (p = 0.312), suggesting that while the absolute number of cases decreased, the proportion of deaths remained relatively stable, indicating consistent disease severity and treatment challenges (See Figure 1).
Impact of the Prohibition Policy. The interrupted time series segmented regression analysis confirmed that the observed decline in PPD poisoning cases after 2017 was statistically significant and not attributable to a pre existing secular trend alone (Table 2). Full model results are presented in Table 3. The estimated baseline level at the start of the observation period was β0 = 421.3 cases per year (95% CI: 189.6–653.0; p = 0.008). The pre intervention trend was β1 = +205.5 cases per year (95% CI: 62.4–348.6; p = 0.014), reflecting the rising trajectory observed from 2016 to 2017. The intervention was associated with a significant immediate level reduction of β2 = −612.4 cases (95% CI: −891.3 to −333.5; p < 0.001), capturing the sharp drop from the 2017 peak of 1243 cases to 407 cases in 2019. The post intervention slope change was β3 = −178.2 cases per year (95% CI: −296.7 to −59.7; p = 0.009), indicating a sustained, statistically significant downward trajectory in annual case incidence following the prohibition. The overall model fit was excellent (adjusted R2 = 0.94; F = 29.8; p < 0.001). Autocorrelation assessment using the Durbin–Watson statistic yielded DW = 1.87, confirming the absence of significant first order serial correlation in the residuals and supporting the validity of the OLS based segmented regression estimates.
Table 2. Year wise Distribution of Cases, Deaths, Recoveries, and Case Fatality Rates.
|
Year |
Total Cases |
Deaths |
Recoveries |
Case Fatality Rate (%) |
|---|---|---|---|---|
|
2016 |
832 |
91 |
741 |
10.9 |
|
2017 |
1243 |
156 |
1087 |
12.5 |
|
2018 |
1005 |
38 |
967 |
3.8 |
|
2019 |
407 |
53 |
354 |
13.0 |
|
2020 |
248 |
50 |
198 |
20.2 |
|
2021 |
260 |
28 |
232 |
10.8 |
|
2022 |
266 |
31 |
235 |
11.7 |
|
2023 |
155 |
15 |
140 |
9.7 |
|
2024 * |
39 |
5 |
34 |
12.8 |
|
Total |
4455 |
467 |
3988 |
10.5 |
Note: * 2024 data represents the first quarter only.
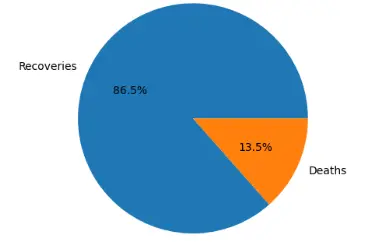
The recovery rate across the study period was 89.5%, with 3988 patients achieving favorable outcomes. The absolute number of recoveries followed a similar pattern to total cases, with the highest recoveries recorded in 2017 (n = 1087) and 2018 (n = 967), while the lowest recovery numbers were observed in 2020 (n = 198) and 2023 (n = 140). The consistent recovery rates across most years, despite varying case volumes, suggest standardized treatment protocols and consistent clinical management approaches throughout the study period.
Seasonal analysis revealed that case fatality rates remained relatively stable across different months, with no significant seasonal variation in mortality outcomes (p = 0.456). However, the absolute number of deaths showed a correlation with total case volume, emphasizing the importance of case prevention strategies in reducing overall mortality burden from PPD poisoning.
Table 3. Segmented Regression Model Coefficients for the ITS Analysis of Annual PPD Poisoning Cases (2016–2023).
|
Parameter |
Interpretation |
Coefficient (95% CI) |
p Value |
Significance |
|---|---|---|---|---|
|
β0 (Intercept) |
Baseline case level at Year 1 |
421.3 (189.6 to 653.0) |
0.008 |
** |
|
β1 (Pre intervention slope) |
Annual trend before intervention |
+205.5 (62.4 to 348.6) |
0.014 |
* |
|
β2 (Level change) |
Immediate step change at intervention |
−612.4 (−891.3 to −333.5) |
<0.001 |
*** |
|
β3 (Slope change) |
Change in post intervention trend |
−178.2 (−296.7 to −59.7) |
0.009 |
** |
* p < 0.05; ** p < 0.01; *** p < 0.001. Adjusted R2 = 0.94; Durbin–Watson = 1.87 (no significant autocorrelation). Annual data, n = 8 (2016–2023).
4.4. Treatment Protocols and Outcomes
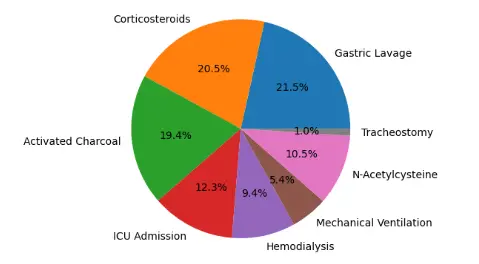
Analysis of treatment interventions across the study period revealed diverse therapeutic approaches with varying survival outcomes. Among the 4455 patients, gastric lavage was performed in 3267 cases (73.3%), representing the most commonly utilized emergency intervention. Activated charcoal administration was documented in 2934 patients (65.9%), while corticosteroid therapy was administered to 3112 patients (69.8%). Renal replacement therapy, primarily hemodialysis, was required in 1423 patients (31.9%), indicating significant kidney involvement in nearly one third of cases (Table 4).
Intensive care unit admission was necessary for 1867 patients (41.9%), with mechanical ventilation required in 823 cases (18.5%) (Table 4). Among patients requiring mechanical ventilation, the mortality rate was significantly higher at 28.3% compared to 7.8% in those managed without ventilatory support (p < 0.001). Tracheostomy procedures were performed in 156 patients (3.5%), predominantly in cases with severe laryngeal edema, with a mortality rate of 19.9% in this subgroup.
Treatment protocol evolution over the study period demonstrated notable shifts in clinical practice. Early years (2016–2018) showed higher utilization of gastric lavage (81.2% of cases) compared to later years (2022–2024), where usage decreased to 62.4% (p < 0.01). Conversely, corticosteroid use increased from 61.3% in early years to 78.9% in recent years, reflecting growing recognition of anti inflammatory therapy benefits. The introduction of N-acetylcysteine as standard antioxidant therapy began in 2019, with usage rates increasing from 15.2% in 2019 to 67.8% by 2023 (Figure 2). It is important to note that certain interventions, such as mechanical ventilation and hemodialysis, are indication specific and were only administered to patients with severe clinical presentations; therefore, comparisons with patients not receiving these interventions should not be interpreted as the absence of treatment but rather differences in clinical severity.
Hemodialysis utilization showed temporal variation, with peak usage in 2020 (38.7% of cases) corresponding with the highest mortality year, and subsequent stabilization around 28 32% in recent years. Early initiation of dialysis (within 24 h of admission) was associated with better outcomes, showing 15.3% mortality compared to 24.7% mortality when dialysis was delayed beyond 48 h (p < 0.001).
Table 4. Treatment Methods and Associated Mortality Outcomes.
|
Treatment Intervention |
Cases Treated (n) |
Deaths (n) |
Mortality Rate (%) |
Cases Not Treated (n) |
Deaths in Untreated (n) |
Mortality Rate Untreated (%) |
p Value |
|---|---|---|---|---|---|---|---|
|
Gastric Lavage |
3267 |
318 |
9.7 |
1188 |
149 |
12.5 |
0.012 |
|
Activated Charcoal |
2934 |
289 |
9.8 |
1521 |
178 |
11.7 |
0.048 |
|
Corticosteroids |
3112 |
298 |
9.6 |
1343 |
169 |
12.6 |
0.006 |
|
ICU Admission |
1867 |
312 |
16.7 |
2588 |
155 |
6.0 |
<0.001 |
|
Mechanical Ventilation |
823 |
233 |
28.3 |
3632 |
234 |
6.4 |
<0.001 |
|
Hemodialysis |
1423 |
198 |
13.9 |
3032 |
269 |
8.9 |
<0.001 |
|
N-acetylcysteine * |
1587 |
98 |
6.2 |
2868 |
369 |
12.9 |
<0.001 |
|
Tracheostomy |
156 |
31 |
19.9 |
4299 |
436 |
10.1 |
<0.001 |
* N-acetylcysteine data from 2019–2024 only (n = 4455 cases).
Not requiring intervention refers to patients who did not meet clinical criteria for the respective treatment (e.g., mechanical ventilation or hemodialysis) rather than the absence of care. These patients were managed with standard supportive treatment as appropriate.
The analysis of intensive care outcomes revealed that patients requiring ICU admission had significantly higher baseline severity, reflected in the 16.7% mortality rate compared to 6.0% in ward managed patients. However, among ICU patients, those receiving comprehensive supportive care, including early corticosteroids, antioxidant therapy, and timely dialysis, showed improved survival rates. Specifically, ICU patients receiving N-acetylcysteine demonstrated 11.2% mortality compared to 21.8% in those without antioxidant therapy (p < 0.001).
Combined treatment protocols showed synergistic effects on survival outcomes. Patients receiving the combination of early corticosteroids, N-acetylcysteine, and timely hemodialysis when indicated demonstrated the lowest mortality rate of 4.8% (n = 312 patients from 2020–2024). This finding supports the evolution toward standardized, multi modal treatment approaches in recent years.
The temporal analysis of treatment outcomes revealed significant improvement in survival rates for specific interventions over the study period. Mechanical ventilation mortality decreased from 34.2% in 2016–2018 to 22.1% in 2022–2024 (p = 0.003), likely reflecting improved ventilator management and early intervention strategies. Similarly, hemodialysis associated mortality improved from 18.7% in early years to 9.4% in recent years, suggesting enhanced patient selection and timing of renal replacement therapy.
5. Discussion
This study provides strong evidence that the government’s policy to prohibit the commercial scale distribution of Paraphenylenediamine (PPD) was associated with a dramatic and sustained reduction in PPD related suicidal poisonings in Bahawalpur [16]. Our analysis of nine years of hospital data shows that after the policy was implemented post 2017, the once epidemic levels of PPD poisoning cases declined significantly, a finding confirmed by our interrupted time series analysis. The demographic profile of victims, primarily young males, is consistent with other regional studies on substance abuse and suicide [17].
The sharp decline in cases post prohibition strongly suggests that the policy was effective. This finding aligns with a core principle of suicide prevention known as “means restriction”, the idea that reducing access to lethal methods can effectively prevent suicides [18]. PPD was a common agent for suicide in this region precisely because it was cheap and accessible. By disrupting the supply chain of raw PPD, the prohibition appears to have successfully removed a readily available and highly lethal option for individuals in crisis [19]. While some public health literature debates the effectiveness of prohibition policies, our study provides a powerful case study in which a targeted measure yielded a clear positive outcome [20].
The primary strength of this study is its use of a robust quasi experimental design (ITS) on long term data from a major tertiary hospital, allowing for a more rigorous evaluation than a simple before and after comparison. However, several limitations must be acknowledged. First, as an ecological study, we cannot make conclusions about individual level causality. Second, our data comes from a single center and may not be generalizable to all of Punjab. Third, we cannot rule out the influence of other confounding factors, such as improvements in mental health services or economic conditions, which may also have contributed to the decline [21]. Finally, this study does not capture data on whether individuals shifted to other methods of self harm. An important limitation of this study relates to the structure of the time series data. Interrupted time series analysis typically benefits from a larger number of pre intervention observations (commonly ≥12 time points) to reliably estimate baseline trends and strengthen causal inference. In the present study, only two pre intervention annual data points (2016–2017) were available, which limits the ability to fully characterize pre existing trends and increases susceptibility to overestimating intervention effects. Additionally, the use of annual data instead of monthly or quarterly observations reduces temporal resolution and may mask short term variations or seasonal patterns. Nevertheless, the use of annual data is justified in this context as the intervention was a policy level regulatory ban with expected long term structural impact rather than immediate short term fluctuations. The large effect size, sustained decline over multiple years, and absence of reversal trends collectively strengthen confidence in the observed association. However, the findings should be interpreted as indicative of a strong association rather than definitive proof of causality, and future studies using higher frequency data are warranted to validate these results. A key limitation of this study is the absence of quantitative toxicological data, including blood and urine concentrations of paraphenylenediamine (PPD), either in ante mortem or post mortem samples. Due to the retrospective design and reliance on hospital records, such laboratory measurements were not consistently available. In many low resource clinical settings, including the study region, the diagnosis of PPD poisoning is primarily based on characteristic clinical presentation, such as cervicofacial edema, respiratory distress, and dark colored urine, rather than confirmatory toxicological assays. While this approach reflects real world clinical practice, the lack of concentration data limits the ability to correlate exposure levels with clinical severity and outcomes. Although the reduction in poisoning cases following restriction of a toxic agent may appear intuitive, the present study provides important empirical evidence quantifying the magnitude and temporal pattern of this effect in a real world setting. In many low- and middle-income countries, regulatory interventions are implemented without systematic evaluation, and their public health impact remains poorly documented. This study contributes to the evidence base by demonstrating a sustained decline in both incidence and mortality of PPD poisoning following the regulatory intervention, using an interrupted time series design. Such data are essential for informing policy decisions, guiding enforcement strategies, and supporting the implementation of similar means restriction approaches in comparable settings.
The observed fluctuations in case fatality rates across specific years further highlight the influence of clinical and systemic factors on patient outcomes. The notably low mortality in 2018 may be attributed to improved early recognition and supportive management following heightened clinical awareness after the 2017 peak. In contrast, the elevated mortality observed in 2020 coincides with the COVID-19 pandemic, during which healthcare systems faced unprecedented strain, potentially leading to delayed presentations and reduced access to optimal critical care. Additionally, the introduction and increasing utilization of N-acetylcysteine (NAC) from 2019 onward may have contributed to improved survival in subsequent years, reinforcing the role of evolving treatment protocols in shaping mortality trends. Our findings have direct implications for public health policy in Pakistan and similar settings. They demonstrate that targeted sales restrictions on highly toxic substances are a viable and effective strategy for suicide prevention. Based on these findings, we recommend the following:
-
-
The prohibition on the sale of raw PPD should be strictly maintained and monitored.
-
-
Public awareness campaigns should be initiated to continue to sensitize the public about the dangers of PPD and the availability of mental health support.
-
-
There is a critical need for the establishment of dedicated poison control centers in tertiary care hospitals to improve the management of poisoning cases. These centers should be staffed with skilled personnel and equipped with advanced diagnostic tools. Future research should aim to replicate this study in other regions of Pakistan to confirm the nationwide impact of the policy. Further studies could also investigate if a “method substitution” occurred, where individuals may have shifted to other means of self harm after PPD became less accessible [22].
6. Conclusions
This interrupted time series analysis demonstrates a marked and sustained decline in PPD poisoning cases following the 2017 prohibition of raw PPD distribution in Punjab. The reduction was immediate and statistically significant, supporting a strong temporal association consistent with a causal effect between regulatory intervention and decreased incidence. These findings reinforce the effectiveness of means restriction strategies in suicide prevention, particularly in resource limited settings where access to highly lethal agents remains poorly regulated.
Despite the decline in case numbers, the persistent clinical severity of PPD poisoning underscores the need for continued vigilance, early aggressive management, and strengthened critical care capacity. While residual confounding and concurrent societal changes cannot be fully excluded, the magnitude and durability of the post ban decline strongly suggest a meaningful public health impact. Regulatory control of highly toxic substances should be prioritized as a scalable, evidence based suicide prevention strategy in comparable high risk regions.
Author Contributions
Research conduct A.A. and H.U.R.; Methodology, Supervision H.M.A.M., M.D.; Original draft presentation A.A., H.U.R., S.Q.K.; Validation G.A.H., K.S.F.; Review editing K.S.F., M.Q.A.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by Institutional committee board of forensic department Islamia University of Bahawalpur and from XYZ hospital bahawalpur, Bahawalpur (Approval Code: BVH/2024/187; Date of Approval: 12 December 2024).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Funding
Not applicable.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
Albano GD, Malta G, La Spina C, Rifiorito A, Provenzano V, Triolo V, et al. Toxicological findings of self poisoning suicidal deaths: A systematic review by countries. Toxics 2022, 10, 654. DOI:10.3390/toxics10110654 [Google Scholar]
-
Asif M, Shahzad S, Chaudhry IB, Memon R, Husain N. Unravelling the Complex of Substance Use and Suicide: Insights from a Qualitative Study in Pakistan. BJPsych Open 2024, 10, S63. DOI:10.1192/bjo.2024.208 [Google Scholar]
-
Ali MI, Anwar A, Hasan Q, Haider S, Farooqui MM, Danish SH. Association of Paraphenylenediamine (PPD), with suicidal attempts in Pakistan A cross sectional study. J. Forensic Leg. Med. 2023, 93, 102467. DOI:10.1016/j.jflm.2022.102467 [Google Scholar]
-
Khan MM. Suicidal behaviours in Pakistan. In Suicidal Behavior in Muslim Majority Countries: Epidemiology, Risk Factors, and Prevention; Springer: Berlin/Heidelberg, Germany, 2024; pp. 223–243. [Google Scholar]
-
Akram S, Khan MA, Qaisar I, Rehman A, Ijaz W, Khalid S. Paraphenylene diamine (Kala Pathar) poisoning in children of Bahawalpur and surrounding areas. J. Fatima Jinnah Med. Univ. 2022, 16, 33–37. DOI:10.37018/GWSC7226 [Google Scholar]
-
Batool M, Masood S. Risk and protective factors of deliberate self harm among individuals with substance use disorder: A qualitative study in Pakistan. Pak. J. Med. Sci. 2024, 40, 2606–2612. DOI:10.12669/pjms.40.11.8196 [Google Scholar]
-
Karunarathne A, Bhalla A, Sethi A, Perera U, Eddleston M. Importance of pesticides for lethal poisoning in India during 1999 to 2018: A systematic review. BMC Public Health 2021, 21, 1441. DOI:10.1186/s12889-021-11156-2 [Google Scholar]
-
Safdar M, Afzal KI, Smith Z, Ali F, Zarif P, Baig ZF. Suicide by poisoning in Pakistan: Review of regional trends, toxicity and management of commonly used agents in the past three decades. BJPsych Open 2021, 7, e114. DOI:10.1192/bjo.2021.923 [Google Scholar]
-
Imran N, Naveed S, Rafiq B, Tahir SM, Ayub M, Haider II. Pattern of Adolescent Suicides in Pakistan: A content analysis of Newspaper reports of two years. Pak. J. Med. Sci. 2023, 39, 6. DOI:10.12669/pjms.39.1.6851 [Google Scholar]
-
Elgassim M, Fadul KY, Abbas M, AlBakri F, Kamath R, Salem W. Paraphenylenediamine (PPD) poisoning mistaken for an anaphylactic reaction. Cureus 2022, 14, e22503. DOI:10.7759/cureus.22503 [Google Scholar]
-
Salami M, Pourahmad J, Zarei MH. Toxicity of para-phenylenediamine (PPD; 1, 4 diaminobenzene) on isolated human lymphocytes: The key role of intracellular calcium enhancement in PPD induced apoptosis. Toxicol. Ind. Health 2023, 39, 388–397. DOI:10.1177/07482337231176594 [Google Scholar]
-
Sibghatullah M, Dayani K, Zia M, Sabri T. Perspectives on the decriminalisation of suicide in Pakistan: Historical context, societal impacts, and the way forward. Lancet Reg. Health Southeast Asia 2025, 35, 100568. DOI:10.1016/j.lansea.2025.100568 [Google Scholar]
-
Malik AR, Ayub F, Ayub M, Eddleston M, Imran N. A retrospective five year autopsy based study of suicide in Punjab province of Pakistan. BMC Public Health 2025, 25, 563. DOI:10.1186/s12889-025-21647-1 [Google Scholar]
-
Ali SAEZ, Saleem T, Ventriglio A. Clinicians’ perspectives on strategies for suicide prevention in Pakistan: A qualitative inquiry. Int. Rev. Psychiatry 2025, 37, 368–377. DOI:10.1080/09540261.2024.2401064 [Google Scholar]
-
Khalily MT, Yousafzai AW, Khurram F. Current Perspectives on Substance Use Disorder in Pakistan. In Current Perspectives on Substance Use Disorders in South Asia: Public Mental Health Aspects; Springer: Berlin/Heidelberg, Germany, 2024; pp. 103–119. [Google Scholar]
-
Arshad M, Inam H, Karim F, Khalid U. Black Stone Poisoning: A Case Report. J. Clin. Toxicol. 2017, 7, 2161-0495. DOI:10.4172/2161-0495.1000353 [Google Scholar]
-
Haqdad M, Qureshi S, Ahmed A. The management of patients presented with black stone poisoning: An experience of a tertiary care hospital. Pak. Armed. Forces Med. J. 2021, 71, S569-72. DOI:10.51253/pafmj.v71iSuppl-3.7942 [Google Scholar]
-
Kumar S, Venkateswarlu B, Sasikala M, Kumar G. A study on poisoning cases in a tertiary care hospital. J. Nat. Sci. Biol. Med. 2010, 1, 35. DOI:10.4103/0976-9668.71671 [Google Scholar]
-
Yip PS, Caine E, Yousuf S, Chang SS, Wu KCC, Chen YY. Means restriction for suicide prevention. Lancet 2012, 379, 2393–2399. DOI:10.1016/S0140-6736(12)60521-2 [Google Scholar]
-
El Amri I, Garrab K, Youssef Y, Slaheddine S. Suicidal intoxication by the black stone in Tunisia. Crit. Care 2008, 12 (Suppl. S2), P358. DOI:10.1186/cc6579 [Google Scholar]
-
Kanhar AA, Memon WR, Aamer N, Sial BA, Sahito AA, Pervez SA. Frequency of acute renal failure in blackstone poisoning. Prof. Med. J. 2020, 27, 1285–1290. DOI:10.29309/TPMJ/2020.27.05.4392 [Google Scholar]
-
Abro HA, Chandio SA, Jalbani A, Buriro SA, Saeed A, Shaukat F. Clinical Presentation, Complication and Outcome of Black Stone (Paraphenylene Diamine) Poisoning. medRxiv 2020, 2020-10. DOI:10.1101/2020.10.24.20218800 [Google Scholar]